Documente Academic
Documente Profesional
Documente Cultură
Diabetes app selection made simple
Încărcat de
Juan Miguel PangilinanTitlu original
Drepturi de autor
Formate disponibile
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentDrepturi de autor:
Formate disponibile
Diabetes app selection made simple
Încărcat de
Juan Miguel PangilinanDrepturi de autor:
Formate disponibile
Updates and advances
in technology for diabetes
self-management
Introduction Andrew Bzowyckyj, PharmD, BCPS, CDE,
associate professor, Pacific University Oregon
Diabetes management is constantly evolving, including new treatment options School of Pharmacy, Hillsboro
with innovative mechanisms of action, a shift toward more shared decision mak-
Correspondence: Andrew Bzowyckyj, Pacific
ing and person-centered care, and increased interest in and availability of diabe- University Oregon School of Pharmacy, 222
tes technology. Recent changes in diabetes technology have been so significant SE 8th Ave., Ste. 451, Hillsboro, OR 97123;
that the American Diabetes Association (ADA) Standards of Medical Care in Dia- bzowyckyj@pacificu.edu
betes–2019 has an entirely new section devoted to diabetes technology.1 This new
section now contains the information about self-monitoring of blood glucose (pre-
viously located within section 6, “Glycemic Targets”). It also contains new recom-
mendations on insulin delivery devices, blood glucose meters, continuous glucose
monitors, and automated insulin delivery devices.1
According to ADA, the term diabetes technology describes “the hardware, de-
vices, and software that people with diabetes use to manage blood glucose lev-
els, stave off diabetes complications, reduce the burden of living with diabetes,
and improve quality of life.”1 This article discusses how these topics relate to the
pharmacist’s role in helping people with diabetes manage their diabetes and other
chronic conditions.
Selecting the right mobile app
As of February 2018, 77% of Americans owned a smartphone, including 46% of
people aged 65 years and older.2 As these devices become more engrained in our
everyday lives, mobile applications for health care–related uses—such as help-
ing patients manage their diabetes—are a logical development. Mobile applica-
tions, or “apps,” are a type of software designed to run on a mobile device, such
as a smartphone or tablet computer.3 As of 2017, there were 325,000 mobile health
apps available for users to download, and industry projections estimated approxi-
mately 3.7 billion downloads of these apps in 2017.4
Accreditation information Learning objectives
Activity type: Knowledge based ACPE Universal Activity Number: After participating in this activity, pharmacists
Provider: APhA 0202-0000-19-152-H01-P will be able to
Target audience: Pharmacists CPE credit: 2 hours (0.2 CEUs) ■■ Identify useful diabetes-related mobile
Release date: May 1, 2019 Fee: There is no fee associated with this activ- applications based on their characteristics
Expiration date: May 1, 2022 ity for APhA members. There is a $25 fee for and functionalities.
nonmembers. ■■ Describe the role of mobile applications in
helping patients manage their diabetes.
APhA is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a
■■ Discuss the criteria that should be used to
provider of continuing pharmacy education (CPE). The ACPE Universal Activity Number
evaluate a mobile application (app).
assigned to this activity by the accredited provider is 0202-0000-19-152-H01-P.
■■ Explain the importance of device accuracy
Advisory board: Jennifer Trujillo, PharmD, associate professor, Department of Clini-
when helping patients select technology for
cal Pharmacy, University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences,
glucose monitoring.
Aurora.
■■ Describe the most useful diabetes
Disclosures: Jennifer Trujillo, PharmD, declares that she is an advisory board member for
self-management devices and support
Sanofi and BD Pharmaceuticals. Andrew Bzowyckyj, PharmD, BCPS, CDE, and APhA’s editorial
tools currently available to patients with
staff declare no conflicts of interest or financial interests in any product or service mentioned in
diabetes.
this activity, including grants, employment, gifts, stock holdings, and honoraria. For complete staff
■■ Compare the various insulin pens and
disclosures, please see www.pharmacist.com/apha-disclosures.
injectable devices that are commercially
Development: This home-study CPE activity was developed by APhA.
available.
www.pharmacist.com MAY 2019 • PharmacyToday 43
CPE_05_19_JD.indd 43 4/22/2019 4:36:54 PM
CPE UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT
media query within professional and/or patient networks,
Preassessment questions
pilot testing the app, and eliciting feedback from patients.5
Before participating in this activity, test your knowledge by an-
swering the following questions. These questions will also be part A clearinghouse website is another practical source for
of the CPE assessment. verifying information about an app. iMedicalApps and
AppScript are two examples of health-related clearinghouse
1. A patient with type 2 diabetes is started on insulin glargine websites in the United States. In addition to these general
U-300 at 10 units once daily. Which of the following apps can health-related sites is a clearinghouse focused entirely on
help him titrate his basal insulin to a safe and effective dose? diabetes, the Diabetes Advanced Network Access (DANA).6
a. Fooducate Last, the United Kingdom’s (U.K.) National Health Service
b. Glooko has developed a clearinghouse that may be of use to indi-
c. Insulia
viduals living outside the U.K., if the specific app of interest
d. Glucose Buddy
is available internationally. Table 1 gives a general overview
of these app clearinghouse websites.
2. A patient heard from a friend about a new app that seems too It is important to emphasize that most health-related apps
good to be true. She is thinking about purchasing the app but are not considered medical apps, which would require meet-
is not sure if it is worth the high upfront cost. Which of the ing the definition and approval criteria of a medical device
following sources of information would be the most helpful and subsequent regulation by FDA. This means that many
for her decision? apps are widely available to the public without formal
a. iTunes App Store User Ratings review or verification of the information provided.7 Before
b. FDA Medical Device Database recommending an app for patient use, therefore, practitio-
c. iMedicalApps Clearinghouse
ners should consult one of these clearinghouse websites
d. National Library of Medicine Mobile Apps
to check the app’s validity and ensure it is of high quality.
Furthermore, when evaluating an app, there are various
3. Which of the following statements is correct about the accu- other aspects to consider beyond the quality of information
racy of continuous glucose monitoring devices? provided. Table 2 provides some additional characteristics
a. Abbott Freestyle Libre requires calibration twice daily. that are important to evaluate.8
b. Senseonics Eversense requires a 2-hour warm-up before One important factor to consider is that not all apps offer
reporting data.
the same set of functionalities. For example, an app may pro-
c. Medtronic Guardian Connect requires calibration every
12 hours.
vide a social outlet (e.g., chat forums, data sharing within a
d. Dexcom G6 sensors can be worn for only 7 days before network), offer a two-way communication medium between
needing replacement. a patient and his or her health care provider(s), or enable a
patient to log self-monitored data (e.g., meals eaten, glucose
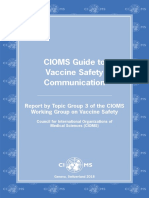
However, many patients and health professionals alike levels, weight measurements) solely for personal use. Before
are easily confused by the vast array of apps available on the encouraging a patient to use an app, it is important to deter-
market today, resulting in an inconsistent uptake of these mine what the patient hopes to accomplish. Figure 1 depicts
valuable resources. With this many apps available, it is not the most common strategies mobile apps use to activate
possible to keep track of all of them. However, picking a few patients. Each level of the pyramid represents an increase
favorites to recommend isn’t ideal, either. Each app offers a in the extent to which an app enables patients to engage in
different set of features, and recommendations should be their own health care, though the exact correlation between
patient-specific. This review discusses some basic principles the two factors has not been directly researched (i.e., it is not
for evaluating apps and highlights several of the more popu- guaranteed that higher engagement with an app correlates
lar apps currently available to assist people with diabetes. directly with an improvement in health outcomes).9
Websites featuring the top diabetes apps Do mobile apps work?
■■ The best diabetes apps of 2018: www.healthline.com/health/
Several systematic reviews have evaluated the efficacy of
diabetes/top-iphone-android-apps
■■ Twelve apps for managing diabetes—blood glucose trackers, food apps in improving diabetes-related health outcomes, with
and exercise logs, and more: www.everydayhealth.com/hs/type- somewhat conflicting results. Interpreting these trials is
2-diabetes-care/diabetes-apps/ complicated because the term app is used to describe a broad
■■ Top four apps for managing diabetes: www.verywellhealth.com/ array of communication methods that would not necessarily
top-apps-for-diabetes-management-1087237 be considered apps by today’s standards, such as software
■■ The best free diabetes apps and trackers: https://dlife.com/the- programs that are desktop computer–based and two-way
best-free-diabetes-apps-and-trackers/
text messaging. Overall, limited evidence suggests that use of
When considering health-related apps, most people typi- some commercially available apps, in conjunction with sup-
cally wonder, “Where do I start?” and “What do I look for?” port from a health care provider or study staff, may improve
Fortunately, several strategies have been proposed for evalu- several short-term diabetes-related outcomes (mainly A1C),
ating and selecting mobile apps: consulting the scientific lit- with the long-term impact unclear.10,11
erature, searching app stores, reviewing app characteristics One systematic review of 21 trials (n = 1,543) evaluated the
(e.g., descriptions, user ratings, reviews), conducting a social impact of using an app to reduce A1C levels in people with
44 PharmacyToday • MAY 2019 www.pharmacytoday.org
CPE_05_19_JD.indd 44 4/22/2019 4:37:28 PM
UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT CPE
Table 1. Overview of app clearinghouse websites
App clearinghouse How to access Developer Content/Description
iMedicalApps ■■ Imedicalapps.com ■■ Independent online ■■ Expert reviews written by
–No login required medical publication health professionals
■■ Collaboration with
MedPageToday
AppScript ■■ Appscript.net ■■ IQVIA (formerly Quintiles & AppScript Score (0–100)
–Free, but login required IMS Health) based on six weighted
domains:
1. Professional
2. Patient
3. Functional
4. Endorsement
5. Developer
6. Clinical
Diabetes Advanced Network ■■ Danaapps.org ■■ AADE ■■ Intelligence-driven curation
Access (DANA) –Free, but login required ■■ DHX Labs ■■ Adaptive privacy and secu-
■■ Danatech.org rity (APS) scan
–Paid AADE membership ■■ Standard review
required 1. App performance
2. Privacy and security
3. Data management
■■ Enhanced review
1. Functionality
2. Usability
3. Behavior science
4. Operability
5. Privacy and security
■■ Trust score
1. Exceptional
2. Good
3. Average
National Health Service (NHS) ■■ Apps.beta.nhs.uk ■■ NHS ■■ App pricing
Apps Library –No login required ■■ Prescription requirements
■■ Description
■■ Photos
■■ Ideal candidates
■■ Overview of operating
instructions
Sources: References 5 and 6.
type 1 and type 2 diabetes. People with type 1 diabetes (n with an A1C reduction of 1.12% (−1.32 to −0.91%, I2 = 0).12
= 516) saw an overall A1C decrease of 0.49% (95% CI [−0.94 The authors did not identify a potential cause for this phe-
to −0.04%]), while those with type 2 diabetes (n = 1,027) saw nomenon, although a separate study found similar results.13
a slightly higher A1C reduction of 0.57% (−0.82 to −0.32%), Two possibilities for this difference in impact between dia-
though there was significant heterogeneity noted among the betes types are 1) the small sample size in the studies inves-
trials within each study population (I2 = 84% and 77% for tigating health professional feedback in type 1 diabetes, and
type 1 and type 2 diabetes, respectively). Of interest, feed- 2) the different types of challenges faced daily by individuals
back from health professionals was negatively correlated living with type 1 and type 2 diabetes.
with A1C reduction in type 1 diabetes, while the opposite
held true for individuals with type 2 diabetes. In the type 2 Apps for calorie tracking and meal
diabetes population, low-frequency feedback (i.e., as needed planning
or once monthly) was associated with an A1C reduction of Numerous mobile apps are commercially available for calo-
0.33% (−0.59 to −0.07%, I2 = 47%), whereas high-frequency rie tracking and meal planning. Table 3 features some of the
feedback (i.e., more than once per month) was associated most common ones. The general functionalities of the apps
www.pharmacist.com MAY 2019 • PharmacyToday 45
CPE_05_19_JD.indd 45 4/22/2019 4:37:47 PM
CPE UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT
Table 2. Important factors to consider when evaluating an app
Factor Importance
Purpose / area of focus The content featured within the app should be of relevance to the patient seeking to use it.
Device compatibility Ensure the app is available on the platform compatible with the patient’s specific device (e.g.,
iTunes, Google Play).
App usability The patient needs to be able to use the app, ideally with minimal instruction. The patient’s tech-
savviness may affect how critical this factor is.
Functionality In addition to being user-friendly, the app must interface with the patient’s daily routine fairly
easily to increase the likelihood of success.
Cost (initial and ongoing) Both the initial and ongoing costs are essential to evaluate to ensure the app is affordable. When
reading app descriptions, note that some app functionalities may only be available to individuals
who have a paid prescription or a premium membership.
User ratings Take a look at how many people have rated the app, in addition to reading some of the actual
comments. To get a broad perspective, one strategy is to read a few of the comments from indi-
viduals who rated the app very highly and then a few more from those who rated it very poorly.
Sometimes a low rating could be related to an experience that may be unique to that user, while a
high rating may be a paid testimonial.
Update frequency This is a good measure of not only how current the app material is but also how frequently the
app developers are working on software updates that enhance the patient’s experience.
Privacy and security policy It is critical to evaluate the relevant privacy and security policies any time health information
is involved. This is especially true for apps that require information to create a profile (e.g.,
name, date of birth) or logging of health-related data (e.g., blood glucose values, laboratory test
results).
HONcode principles (Health ■■ Authority: State the qualifications of authors/contributors.
On the Net Foundation) ■■ Complementarity: Provide information to support, not replace, the patient–provider relation-
ship.
■■ Privacy: Respect the privacy and confidentiality of personal data submitted to the site by the
visitor.
■■ Attribution: Cite sources and dates of medical information being provided.
■■ Justifiability: Provide balanced and objective claims with justifications.
■■ Transparency: Provide valid contact details.
■■ Financial disclosure: Always provide details of funding sources.
■■ Advertising: Clearly distinguish advertising from editorial content.
Sources: References 5 and 8.
vary, but most provide the ability to log meals, exercise, details about why the product received that specific grade
weight, and even water intake, at a minimum. and a list of healthier alternatives (if available). Additional
The more mainstream apps have internal databases that functionalities include somewhat-customizable meal plans
feature the nutrition information of foods from popular res- (e.g., person-specific calorie and macronutrient goals), social
taurants in addition to many foods and ingredients avail- elements (e.g., ability to comment on and applaud others’
able at your local grocery store. Most also feature the abil- entries), and general information on health and wellness
ity to turn a smartphone’s camera into a barcode scanner to (e.g., blog posts, articles, fitness videos).
instantly import the nutrition information from the product It is important to emphasize that the customized meal plan
packaging. For dishes that may not be found in a database, should not replace a dietitian’s expertise. If a patient is under
such as a family recipe, MyFitnessPal also provides the abil- a dietitian’s care, make sure the app’s recommendations are
ity to enter the full recipe for a specific dish on its website consistent with the dietitian’s specified clinical recommen-
(not on the smartphone app). This feature compiles the nutri- dations. This will prevent confusion and enhance collabora-
tion information of each ingredient and translates it into a tion among the care team. In addition, to maximize patient
per-serving breakdown, which in turn becomes accessible convenience, if a patient is using a specific device or app (e.g.,
within the user’s database on their smartphone when log- fitness tracker, running app) to track other meaningful data,
ging that meal. check whether it interfaces with the calorie tracking and
Another app that offers a unique functionality, Fooducate, meal planning app of interest.
provides “grades” for specific foods (range: A–F), including A drawback of using calorie tracking and meal planning
46 PharmacyToday • MAY 2019 www.pharmacytoday.org
CPE_05_19_JD.indd 46 4/22/2019 4:38:08 PM
UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT CPE
Figure 1. Strategies to activate patients using mobile applications based on level of engagement with health care
Source: Reprinted with permission from reference 9.
apps in diabetes is that they are not diabetes-specific, so The app can also use the individual data points to provide
there is no ability to log additional data that may be impor- the patient with an estimated A1C, although this practice can
tant for living well with diabetes, such as glucose readings have unintended consequences. For example, if the logged-in
and insulin doses. Comprehensive diabetes-specific apps do glucose levels are all within the goal range, but the patient’s
exist, however, and will be discussed later in this article. glucose levels are substantially elevated at other times of the
day (i.e., not captured in the log), this may create a false sense
Apps for logging glucose and other data of security for the patient and subsequent confusion when an
It is time to say goodbye to paper glucose logbooks with tiny actual lab test measure shows a discrepant value. Therefore,
boxes that are difficult to see and practically impossible to it is important to educate patients about the limitations
write in or read. Like calorie tracking apps, glucose monitor- (mainly related to sampling bias) of calculating an estimated
ing apps enable users to log their glucose readings as well A1C from a glucose log.
as other pertinent information (e.g., mealtimes, medications Other features of these apps may include feedback on the
administered, symptoms). Table 3 features some common results logged, ability to upload photos of meals and track
apps used for logging glucose readings. One benefit of log- additional data (i.e., weight, blood pressure), and social sup-
ging electronically is the app’s ability to quickly transform port. In addition, many of these types of apps sync with
the data into a visual or graphic representation of overall other apps, wearable technologies (e.g., smart watches, fit-
glucose patterns. These graphic renderings of data (e.g., per- ness trackers), glucometers, and even continuous glucose
centage of readings above or below a certain goal, averages monitors. This feature helps automate this data collection so
at certain times of day, trend lines) may be easier for a patient users don’t have to take the extra steps of logging the data
to understand. separately.
www.pharmacist.com MAY 2019 • PharmacyToday 47
CPE_05_19_JD.indd 47 4/22/2019 4:39:02 PM
CPE UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT
Table 3. Characteristics of common mobile apps
App User ratings Price General functionality
(as of December 2018) (varies by app)
Calorie tracking and meal planning
MyFitnessPal Apple: 4.7 out of 5 (494 K) Basic version is free. ■■ Ability to log
(iTunes: #5 in Health/Fitness) Android: 4.6 out of 5 (1.96 M) Premium version: – Meals
$9.99/mo – Exercise
$49.99/y
– Weight
SparkPeople Calorie Tracker Apple: 4.6 out of 5 (8 K) Basic version is free. – Water intake
(Calorie counter and diet tracker) Android: 4.5 out of 5 (33 K) Premium version: ■■ Internal nutrition lists and calorie
$4.99/mo database
My Diet Diary Calorie Counter Apple: 4.6 out of 5 (911) Free ■■ Customized meal plans
Android: 4.1 out of 5 (19 K) ■■ Sync with other apps, devices,
and wearable technology
Fooducate Nutrition Tracker Apple: 4.7 out of 5 (29 K) Basic version is free. ■■ Social element
(iTunes: #110 in Health/Fitness) Android: 4.4 out of 5 (15 K) Premium version: ■■ Articles
$0.99–$7.99/mo ■■ Fitness videos
$29.99–$99.99/y
Logging glucose and other data
mySugr Apple: 4.7 out of 5 (1.9 K) Basic version is free. ■■ Log glucose levels, meals, meds,
Android: 4.6 out of 5 (23.8 K) Premium versions: BP, weight, A1C
$2.99–19.99/mo ■■ Report estimated A1C (eA1C)
$27.99–199.99/y ■■ Motivating challenges and
feedback
Sugar Sense Diabetes App Apple: 4.6 out of 5 (4.1 K) Free
■■ Sync with other apps, devices,
Android: 4.2 out of 5 (1.2K)
and wearable technology
Health2Sync Diabetes Care Apple: 4.7 out of 5 (69) Basic version is free. ■■ Upload photos of meals
Android: 4.6 out of 5 (6.4 K) Premium versions: ■■ Social support (designated
$2.99/mo partners)
$7.99/3 mo
$14.99/6 mo
Comprehensive diabetes apps
Glucose Buddy Apple: 4.8 out of 5 (10.8 K) Basic version is free. ■■ Log glucose levels, insulin,
Android: 4.4 out of 5 (14.4 K) Premium version: meals, weight, ketones, eA1C,
$14.99/mo cholesterol, BP
$59.99/y ■■ Provide insights into daily trends
■■ Track carb intake, steps, and
MyNetDiary Diabetes Tracker Apple: 4.5 out of 5 (576) $9.99
activity
Android: 4.6 out of 5 (564)
■■ Scan food labels for carbs
Diabetes:M Apple: 4.6 out of 5 (403) Basic version is free. ■■ Sync with other apps, devices,
Android: 4.6 out of 5 (17.7 K) Premium versions: and wearable technology
$4.99/mo ■■ Import/export and reminder/
$49.99/y target capabilities
Glucosio Apple: 3 out of 5 (4) Free ■■ Receive help/motivation from
Android: 4 out of 5 (290) friends/community
■■ Calculate insulin bolus doses
Glooko Apple: 3 out of 5 (64) Free ■■ Set reminders to take meds,
Android: 4 out of 5 (928) Optional subscription: $5/mo with exercise
payment for the first year upfront ■■ Share data (either anonymously
Diabetes Connect Apple: 4.5 out of 5 (50) Free or with caregivers)
Android: 4.5 out of 5 (4.3 K) Optional in-app purchases ■■ Search food or medication
databases
PredictBGL Insulin Dose Calc Apple: 3.7 out of 5 (15) Free
■■ Insulin dose calculator with
Android: 3.5 out of 5 (47) Optional upgrade
predictive analytics
■■ Predict blood glucose levels; has
alerts warning of predictive low
■■ Coaching and just-in-time
education
Sources: References 5 and 6.
48 PharmacyToday • MAY 2019 www.pharmacytoday.org
CPE_05_19_JD.indd 48 4/22/2019 4:40:08 PM
UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT CPE
Apps for titrating basal insulin doses monitoring. These apps combine multiple aspects of the
Clinical inertia has been a significant and common barrier products previously discussed (e.g., logging glucose lev-
to helping patients achieve their diabetes-related goals.14 els, meals, insulin doses; scanning food labels; socializa-
This phenomenon is especially applicable to titrating basal tion aspects; syncing with other apps, devices, and wear-
insulin doses after initiation,15,16 despite previous research able technologies) as well as provide additional features for
leading to the development of simple treat-to-target insulin people living with diabetes. Depending on the amount and
algorithms that patients with type 2 diabetes can use on their quality of data compiled, the apps can provide insights into
own—without needing to schedule a clinic appointment or a patient’s daily trends, including use of predictive analytics
call a health professional for advice (e.g., increase two units to inform treatment considerations (e.g., calculating a meal-
every 3 days until the mean fasting glucose is 100 mg/dL).17,18 time insulin dose, warning of a predictive low, coaching/
Mobile apps that help patients feel more comfortable about just-in-time education). These apps can also facilitate sharing
increasing their basal insulin doses have sought to fill this of various data with family members, social networks, and
gap. Two examples are My Dose Coach and Insulia, which health professionals.
work very similarly. These apps integrate information a One particular app, mDiabetes, was evaluated in a
patient enters about their glucose patterns and apply an algo- 24-week, multicenter, randomized controlled trial in a South
rithm to recommend dose modifications. In addition to pro- Korean adult population with type 2 diabetes.23 In this study,
viding the patient a number, both apps explain why a spe- patients were randomized to use either the app (n = 90) or
cific dose was chosen. It is important to emphasize that these a paper logbook (n = 82). The primary outcome was change
apps are for basal insulin titrations only, as bolus insulin in A1C at 24 weeks. Use of the app resulted in an additional
doses are much more difficult to titrate based off a broadly 0.35% reduction in A1C over the paper logbook group (0.14–
generalizable algorithm. 0.55%, P = 0.001), as well as a larger percentage of patients
having an A1C below 7% without hypoglycemia (odds ratio
Apps for diabetes education and 1.82 [95% CI 1.03–3.21] P = 0.024).
empowerment
Recognizing that many people with diabetes have limited Modernizing diabetes management and
time to pursue formal education in diabetes self-manage- patient care
ment, developers have also created apps that help bridge this As people with diabetes can attest, living with the disease
gap. One such app, KingFit, features quick and convenient is not easy. Granted, advances in diabetes care over the last
videos, generally 10 minutes or less, on a variety of diabetes- 30 years have dramatically improved patients’ ability to
related topics. The app’s developers state on their website manage their diabetes. Development of recombinant insu-
that the educational information is provided by a certified lins in the 1980s resulted in fewer insulin hypersensitivity
diabetes educator, which is another positive attribute. reactions, and development of insulin analogs in the 1990s
Another app in this area is WellDoc BlueStar, an FDA- increased the likelihood of people safely achieving tighter
cleared Class II medical device.19 This app provides a vari- glucose goals. Portable glucometer technology has evolved
ety of features to enhance the patient experience, including continually throughout the 21st century, making them more
personalized messages analyzing glucose patterns based on accessible and accurate than ever before.24,25 These evolutions
patient-derived data and computerized algorithms, diabetes in technology have substantially decreased production costs,
education videos, tailored coaching messages, and weekly which over the years has generally driven down the costs
challenges to engage and motivate users. The app also has a to patients for obtaining these tools and devices. However,
prescription version (BlueStar Rx) that has all the same func- decreased production costs do not always translate directly
tionalities as the nonprescription version, in addition to an into affordability for patients.26–28
insulin dose calculator that aids in calculating the dose of Despite all these breakthroughs and developments, there
insulin needed for a given amount of carbohydrates and/or are still many challenges and limitations in helping people
current blood glucose value.20 with diabetes achieve their health goals. Barriers to medica-
In one randomized controlled trial, this app helped tion adherence will always be a problem, especially those
patients decrease A1C approximately 1% beyond that of the related to remembering when to take a medication and deter-
control group within 3 months (−2.03% vs. −0.68%, P < 0.02). mining if a patient actually took their medication. It is easy
In the intervention group, an additional 60% of patients had to look at a pillbox to see if the tablets that were supposed to
their medications titrated or changed by their health profes- be taken at a specific time are still in that cube. However, it
sional, compared with the standard of care group, over the is not possible to apply the same principle for an injectable
same time period (84% vs. 23%, P = 0.002).21 A sustained A1C medication, and the result may be a patient repeating one or
reduction of a similar magnitude was seen over 1 year in a more doses.
slightly longer study.22 Another challenge is the accuracy of the available data.
Although health data are abundant in today’s era of por-
Comprehensive diabetes apps table glucometers and wearable technologies, the infor-
This last app-related section considers apps that address mation derived from these sources is still limited by fac-
multiple facets of living with diabetes, such as meal plan- tors that affect their accuracy (e.g., approval standards for
ning, exercise habits, medication use, and blood glucose glucometers, limitations with A1C testing).29 Furthermore,
www.pharmacist.com MAY 2019 • PharmacyToday 49
CPE_05_19_JD.indd 49 4/22/2019 4:40:27 PM
CPE UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT
self-monitoring of blood glucose at specific time points does market (i.e., upon initial FDA approval). The manufacturers
not capture out-of-range values in between these checks (an are not required to update their technology to meet newer
issue affecting all individuals with diabetes, but especially standards that take effect after their meter is approved.32
those with type 1 diabetes). The information derived from these types of studies can
Last, developments in technology do not always consider be used to inform decisions about diabetes care, includ-
the patient’s experience (i.e., whether these new devices and ing which glucometer(s) to recommend to a patient, which
tools are user-friendly and convenient) or accessibility to the glucometer(s) a health plan should cover, and how to modify
average patient (e.g., affordability, coverage by third-party a patient’s medication regimen on the basis of self-monitored
payers). In light of these challenges and limitations, the next blood glucose data derived from a glucometer.
few sections of this article highlight some recent develop- Although the accuracy of the results derived from a glu-
ments in technology that can help patients and clinicians cometer is very important, practitioners must consider other
overcome these barriers to managing their diabetes. factors when determining the ideal glucometer for a patient.
Today’s meters have many more functions beyond simply
Glucometer considerations providing a glucose value. These include providing feed-
The accuracy of commercially available glucometers is inher- back, reminders, and alerts to the patient (and potentially to
ently at a crossroad between the accuracy of the results the caregivers/family members); integrating Bluetooth and USB
glucometer can provide and the cost associated with ensur- technology to communicate with mobile apps, and generat-
ing that level of accuracy. These two variables are directly ing reports for self-evaluation and/or dissemination to the
correlated, whereby increasing one undoubtedly increases patient’s health care provider. These functions are only ben-
the other. Realizing that there will likely never be a “perfect” eficial for patients who use them, so a discussion about the
meter, the Diabetes Technology Society (DTS) established basic functionalities a patient looks for in their meter and
the Blood Glucose Monitor Surveillance (BGMS) program whether they would actually use them is critical for evalu-
to determine the current level of accuracy of several meters ating whether a glucometer with more advanced functions
available on pharmacy shelves.30 would be helpful.
The DTS study evaluated 18 different meters (constituting For patients with retinopathy or other forms of visual
90% of the commercially available systems used between impairment, other factors to consider include screen size,
2013 and 2015) purchased directly off the shelves of various text display size, and backlighting. Patients with diminished
consumer outlets. Study participants (n = 1,035) were adults manual dexterity may have difficulty with certain glucom-
with type 1 diabetes, type 2 diabetes, prediabetes, or no dia- eters that have small parts, vials that need to be screwed on
betes. Three different clinical sites were used in a way that and off (vs. flip-tops), and complex lancet devices. Last, peo-
ensured all 18 blood glucose meters were tested at all three ple with type 1 diabetes who may need to test periodically for
sites. Each participant was tested on six different meters in ketones may benefit from a glucometer that can test for both
addition to having a capillary glucose drawn (i.e., control substances (e.g., Precision Xtra, NovaPlus Max), although test
value). The study implemented a triple-blinded methodology, strips designed specifically for measuring ketones will also
in which the investigators, laboratory staff, and statisticians need to be purchased separately.34
did not have enough information to break the code until after
all the results were calculated and finalized. The investiga- Continuous glucose monitoring (CGM)
tors compared each glucometer with standards derived from systems
the International Organization for Standardization and FDA CGM systems, a technology that is increasingly available,
2016 guidance.31,32 Glucose levels above 100 mg/dL needed to addresses the challenge of not knowing specific glucose
be within 15% of a reference plasma value, whereas glucose patterns between individual glucose checks. These systems
levels below 100 mg/dL needed to be within 15 mg/dL of a come with three components: a wearable sensor, a transmit-
reference plasma value. ter, and a receiver. Once the sensor is placed on the patient
To pass the test, at least 91% of the samples within each and calibrated (if applicable), the CGM system automatically
study had to be within the specified standard range. A seal and repeatedly checks the glucose levels of the interstitial
of approval was awarded to any glucometer that passed the fluid surrounding the sensor at regular time intervals (usu-
studies performed at all three study sites. Table 4 gives an ally 5–15 min).35 Depending on the device, this information
overview of the main results. Additional details are avail- is transmitted to a receiver—often the patient’s glucometer,
able at the DTS website (www.diabetestechnology.org/ insulin pump, or smartphone device—at regular intervals
surveillance.shtml), including the overall variation in each (i.e., real-time CGM) or when requested by the patient (i.e.,
meter’s data, percentage of values within specified error lim- flash CGM).
its, and other information.33 This technology is especially beneficial for people living
It is important to note that meters that did not receive a DTS with type 1 diabetes, and for anybody with diabetes of either
seal of approval are not inherently “bad” meters. However, type who is 1) taking multiple daily injections of insulin and
the study represents an important step for increasing trans- has a mismatch between their A1C values and glucometer
parency in glucometer accuracy. Many people do not know readings, 2) at high risk for hypoglycemia (including hypo-
that meters available for purchase today are only required to glycemia unawareness), and/or 3) experiencing clinically
meet the accuracy standards in place when they entered the significant glycemic variability.35–37 The first CGM systems
50 PharmacyToday • MAY 2019 www.pharmacytoday.org
CPE_05_19_JD.indd 50 4/22/2019 4:40:55 PM
UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT CPE
Table 4. Results of the 2018 Diabetes Technology Society (DTS) Blood Glucose Monitor System (BGMS)
Surveillance Program
Brand BGMS Test strip Study sites Compliant (N) Valid trials Compliant (%)
passed
Meters receiving a DTS seal of approval
Bayer Contour Next Contour Next 3 311 312 99.7%
Roche Accu-Chek Accu-Chek 3 306 311 98.4%
Aviva Plus Aviva Plus
Arkray Walmart ReliOn ReliOn 3 307 317 96.8%
Confirm/Micro Confirm/Micro
Agamatrix CVS Advanced CVS Advanced 3 307 318 96.5%
Abbott FreeStyle Lite FreeStyle Lite 3 298 312 95.5%
Roche Accu-Chek Accu-Chek 3 305 320 95.3%
SmartView SmartView
Meters NOT receiving a DTS seal of approval
Arkray Walmart ReliOn ReliOn Prime 2 288 312 92.3%
Prime
LifeScan OneTouch Verio OneTouch Verio 2 294 319 92.2%
Prodigy Prodigy Auto Prodigy No 2 282 312 90.4%
Code Coding
LifeScan OneTouch Ultra2 OneTouch Ultra 2 280 311 90.0%
Abbott Walmart ReliOn ReliOn Ultima 2 285 319 89.3%
Ultima
Bayer Contour Classic Contour 1 284 320 88.8%
Omnis Health Embrace Embrace No 1 282 319 88.4%
Code
HDI/Nipro TrueResult TrueResult 1 279 318 87.7%
HDI/Nipro TrueTrack TrueTrack 0 167 205 a
81.5%
BioSense SolusV2 Solus 0 244 320 76.2%
Medical
Diabetic Supply Advocate Advocate 0 241 319 75.5%
of Suncoast Redi-Code+
Philosys, Inc. Gmate Smart Gmate 0 226 320 70.6%
No study 3 data because of a test strip recall occurring during the time of this study.
a
Source: Adapted with permission from Diabetes Technology Society (DTS) Blood Glucose Monitor System Surveillance (BGMS) Program website.
approved by FDA were professional, or “blinded,” CGM sys- over flash CGM technology is the ability to send alerts to the
tems, in which the sensor regularly recorded the patient’s patient and caregiver(s) regarding predicted dangerous glu-
glucose levels, but the data could not be obtained until the cose levels (i.e., hyperglycemia, hypoglycemia) if the current
sensor was brought back to the clinic to be uploaded and ana- trend is not corrected. Table 5 provides an overview of the
lyzed by a health professional retrospectively. Over time, the various FDA-approved personal CGM systems.38–42
technology has evolved to include personal, or “unblinded,” Glucose levels in the interstitial fluid often lag 5 to 15
CGM devices that provide information about glucose trends minutes behind blood glucose levels, especially when
directly to the patient.35 blood glucose levels are changing rapidly. Because the
Personal CGM systems can be further subdivided into sensor is measuring glucose in the interstitial fluid rather
real-time and flash CGM systems. Real-time systems actively than capillary glucose, complex calibration algorithms
report data at regular intervals independent of the patient’s embedded within CGM systems translate the data derived
actions, while flash systems require the patient to request into a useable blood glucose value that can be reported
the data at specific intervals to evaluate the information ret- on the patient’s receiver and acted upon.35 To increase the
rospectively. Although both systems have inherent benefits level of accuracy, some systems may require calibration
and drawbacks, one clear advantage of real-time systems with a capillary blood glucose measurement (check using
www.pharmacist.com MAY 2019 • PharmacyToday 51
CPE_05_19_NEW.indd 51 4/23/2019 7:52:13 AM
CPE UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT
Table 5. Comparisons of personal continuous glucose monitor (CGM) systems
Manufacturer FDA-approved Warm-up time Minimum Sensor Real-time vs. FDA approved
and device age calibration duration flash for treatment
model frequency decision
Dexcom G5 ≥2 y 2h Every 12 h 7d Real-time Yesa
Mobile
Dexcom G6 ≥2 y 2h Not required 10 d Real-time Yesa
Medtronic 14–75 y 2h Every 12 h 7d Real-time No
Guardian
Connect
Abbott ≥18 y 1h N/A 14 d Flash Yesa
Free-style
Libre 14-day
Senseonics ≥18 y 24 h Twice daily 90 d Real-time No
Eversense
(implant)
a
Assumes symptoms are consistent with the reading and there are no concurrent interactions.
Source: References 38 through 42.
patient’s glucometer) periodically (e.g., every 12 h). the cost, as this technology may still be more costly than tra-
CGM technology comes with its own set of terminology. ditional blood glucose monitoring with a glucometer.
One important term to be aware of is warm-up time: the time In evaluating the effect of these systems on patient out-
it takes for the sensor to calibrate once it is placed, before it comes, one review concluded that use of CGM in type 1 dia-
can start to accurately report data. This time period generally betes results in approximately 0.5% improvement in A1C and
ranges between 1 and 2 hours (Eversense implant requires a mild decrease in hypoglycemia.45 Another review evaluated
24 h). During this time, the patient must use a glucometer to the literature surrounding use in several patient populations,
check blood glucose. This time is an essential component for including patients at high risk for hypoglycemia (type 1 and
ensuring the accuracy of the sensor by allowing it to calibrate type 2 diabetes), hospitalized patients with type 2 diabetes,
after it is placed. and pregnant women with diabetes. These analyses generally
Another commonly used term with CGM systems is trend favored CGM use in these patient populations.46
arrows. These arrows are displayed next to the glucose level Although these data are positive, it is important to remem-
on the patient’s receiver and are designed to help the patient ber that these systems are solely for monitoring and still
put the number into context. For example, if the patient sees require the patient to act on the health information provided.
one or two upward arrows next to the current glucose read- A clinical benefit will not be seen unless the patient is appro-
ing, they will know what their current glucose level is, as well priately engaged in their own care and has the health literacy
as be notified that their glucose level is rapidly increasing at and numeracy skills to interpret and act on the information.
a rate greater than 2 mg/dL/min.43,44 This additional informa- Therefore, to get the most benefit from these systems, health
tion is especially helpful for informing treatment decisions, professionals will need to select the ideal patient candidates
particularly when compared with a glucometer, which can matching the characteristics previously described, train them
only give the current glucose reading without any additional on how to use the device and interpret the data derived from
context about the trends. it, and follow up with them periodically.
Because the cost of this technology has decreased substan-
tially over the years, access to these devices is becoming much Insulin pens and injectable devices
more mainstream, with some being sold right out of the local Disposable pens may not seem like a technological advance-
community pharmacy. Since there are multiple limitations in ment by today’s standards, but it is safe to say they have
using a 3-month average (i.e., for A1C) to evaluate a patient’s significantly improved diabetes care. Their convenience
overall approach to diabetes management, this technology and relative ease of use have increased their availability to
can provide an additional objective measure: time in range. patients (a welcome change from vials and syringes), which
Think of how much more useful it would be for a person in turn has been shown to improve adherence to therapy.47
to know that their glucose levels in the last 3 months were These disposable pen devices were subsequently adapted for
within the goal range approximately 80% of the time rather use in administering noninsulin injectable medications (e.g.,
than that their 3-month average (A1C) suggested they were glucagon-like peptide-1 agonists), as well as a safer way to
above goal at some point in the past 3 months. However, the administer concentrated insulin by eliminating the need to
benefit on patient outcomes must be robust enough to justify convert a U-100 syringe into its equivalent units.
52 PharmacyToday • MAY 2019 www.pharmacytoday.org
CPE_05_19_NEW.indd 52 4/23/2019 7:51:48 AM
UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT CPE
Despite these improvements in technology, patient safety automatically via Bluetooth and AppleHealth from a synced
concerns abound with the use of disposable pens. Concerns glucometer or CGM device), factor in active insulin time, and
center on keeping pen needles attached to the pen and/ document carbohydrate intake. It offers many of the same
or reusing pen needles, not removing the inner cap prior functionalities as an insulin pump without the high upfront
to injection, dialing the pen back down instead of pushing cost and requirement of having a device permanently con-
the plunger in to administer the dose, and using a syringe nected to the person using it. InPen is approved for use in
to withdraw the insulin out of the pen, among other behav- individuals aged 12 years and older taking multiple daily
iors.48 Therefore, it is critical that pharmacists employ the S.C. insulin injections (i.e., not on an insulin pump). It is com-
teach-back method to educate patients on proper use of these patible with insulin lispro and insulin aspart cartridges and
devices and periodically re-evaluate to determine if patients administers up to a maximum of 30 units per dose in 0.5-unit
are using good administration technique. increments. Available by prescription only, the InPen requires
A further complication is that whereas insulin pens used a health care provider to input patient-specific parameters
to be fairly standardized (i.e., 100 units/mL, 3 mL/pen, gener- (e.g., glucose targets, carb-to-insulin ratio, correction factor)
ally five pens/box, and a 28-day beyond-use dating at room into the mobile app.53
temperature), nowadays there are many different varia-
tions in product formulations and beyond-use dating. These Insulin pumps and the pursuit of the
options are meant to accommodate the highly variable insu- artificial pancreas
lin needs of people living with diabetes, but they increase the This article would be incomplete if it did not discuss recent
potential for medication errors and prescription discrepan- updates in insulin pump technology. As these devices are
cies.49 Pharmacists should be aware of the similarities and often sold and managed by the pump companies themselves
differences among the various pen devices so they can field and are limited to a very niche patient population, this will
questions that patients and other health professionals will not be an extensive review. However, it is important to be
undoubtedly have. aware of this technology should you come across a patient
Needle technology has also dramatically improved, from who may be an ideal candidate or is asking about obtaining
the original 12.7-mm needle length (suitable for an I.M. injec- an insulin pump.
tion), to a pen needle as short as 4 mm and syringe needle of 6 The basic premise behind an insulin pump is the ability to
mm. Because of the risk of I.M. injections and concerns about supply a continuous infusion of low-dose rapid- or short-act-
highly variable insulin absorption and kinetics, international ing insulin subcutaneously to satisfy the patient’s basal insu-
consensus recommendations on insulin delivery now advise lin needs. In addition, an insulin pump can provide larger
using the 4-mm needle for all adults and children. If 4-mm bolus doses to manage the body’s mealtime insulin needs.
needles are not readily available, the advice is to at least avoid The pump contains a reservoir that can store a range of 200 to
needles longer than 8 mm for adults and 6 mm for children.50 300 units of insulin. The pump is connected to the user’s body
Although the new pen and needle technologies are helpful via an infusion set that must be changed approximately every
for improving adherence, they do not necessarily help people 3 days. The pump can also factor in additional information it
remember if they actually administered their insulin dose. To receives from various sources to provide a situation-specific
address this problem, Novo Nordisk developed the NovoPen recommendation to the patient when determining an appro-
Echo, a reusable pen device that is compatible with insulin priate mealtime bolus dose. This information includes current
aspart cartridges. This pen is capable of administering half- blood glucose levels, blood glucose trends (if the patient has
unit doses, with a maximum of 30 units per dose. It also has CGM), anticipated amount of carbohydrate intake, patient-
a dose memory feature on the pen cap that displays how specific carb-to-insulin ratio and correction factor, glucose
much insulin was injected during the most recent adminis- target ranges, and active insulin time. A thorough overview
tration and how many hours have passed since that dose was of these terms specific to insulin pumps is available online
administered.51 from Medtronic.54
Another technological innovation to help remember Currently, three major companies manufacture insu-
whether a dose was administered (and how much) has been lin pumps: Insulet Corporation (Omnipod), MedTronic
developed by Diabnext. The device, called Clipsulin C3, sim- (MiniMed), and Tandem (T:slim). In addition to these more
ply clips on to most FDA-approved insulin pens that dial in traditional pumps is an emerging technology: the dispos-
1-unit increments. It subsequently transmits the informa- able insulin patch pump (e.g., V-Go), which provides a fixed
tion related to the dose of insulin being administered to the basal rate of insulin as well as customizable mealtime doses
patient’s smartphone via Bluetooth technology. The informa- in fixed-unit increments (e.g., up to 36 units for the V-Go in
tion is then automatically documented in a virtual logbook 2-unit increments). These types of insulin pumps adhere
that can be transmitted to others (e.g., caregiver, health care directly to a user’s skin and therefore require no tubing. The
provider) if desired.52 fixed parameters associated with these patch pumps make
One final product is InPen, a reusable pen that not only them difficult to meet every patient’s needs, but they offer a
documents how much and when the last insulin dose was substantially lower-cost option to the right patient.55
administered but can also assist with calculating bolus doses One misconception many patients have about insulin
using a Bluetooth-paired smartphone app. The app can be pumps is that the pump can “do all the work.” However, as
used to document glucose readings (either manually or you can see from the list above, the pump is merely a tool
www.pharmacist.com MAY 2019 • PharmacyToday 53
CPE_05_19_JD.indd 53 4/22/2019 4:41:50 PM
CPE UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT
to help inform the patient’s clinical decision making. The In addition to mobile devices and apps, the technologic
patient must still count carbohydrates, factor in the impact of innovations related to medication administration and glu-
other macronutrients (fat and protein) and activity level, and cose monitoring are also dramatically evolving. As the pro-
understand the patient-specific symptoms they may be expe- duction costs for this technology decrease, many of these
riencing. If interested in learning more about the nuances of products will likely be sold at the local community phar-
each individual insulin pump, see the comprehensive review macy. Therefore, pharmacists are in a critical position to
published annually by ADA.55 educate patients on these devices, periodically evaluate how
Fortunately, ongoing research is helping to further decrease patients are doing with them, and collaborate with the rest of
the impediments that remain with use of insulin pump tech- the patient’s care team to help patients manage their diabetes
nology. The initial evolutions in this process included the using the technology available, both now and in the future.
integration of CGM technology, which paved the way for the
pump to automatically initiate a low-glucose-threshold sus-
pend. This feature automatically stops the flow of insulin for References
a set time period (usually up to 2 h) once a patient’s glucose 1. American Diabetes Association. 7. Diabetes technology: Standards
enters (or is trending toward) the patient-specific hypoglyce- of Medical Care in Diabetes—2019. Diabetes Care. 2019;42(Suppl
1):S71–S80.
mia threshold, thereby decreasing the risk of serious hypo-
2. Pew Research Center. Mobile fact sheet. http://www.pewinternet.
glycemic events, especially nocturnal hypoglycemia.56 org/fact-sheet/mobile/. Accessed February 25, 2019.
From here, technology has advanced further with approval 3. Techopedia. Mobile application (mobile app). https://www.techope-
of the Medtronic 670G system, the first hybrid closed-loop dia.com/definition/2953/mobile-application-mobile-app. Accessed
system for people with type 1 diabetes. The pump is paired February 25, 2019.
with the Guardian CGM Sensor and is capable of a function 4. Research 2 Guidance. 325,000 mobile health apps available in
2017—Android now leading mHealth platform. https://research-
called “auto mode.” In auto mode, a built-in algorithm adjusts
2guidance.com/325000-mobile-health-apps-available-in-2017/.
the basal delivery of insulin every 5 minutes based on the Accessed February 25, 2019.
CGM data received and the predetermined target glucose 5. Boudreaux ED, Waring ME, Hayes RB, et al. Evaluating and se-
level. Auto mode is also able to suspend or decrease insulin lecting mobile health apps: strategies for healthcare providers and
delivery to prevent an expected hypoglycemic episode. One healthcare organizations. Transl Behav Med. 2014;4:363–71.
trial demonstrated an approximate 0.5% reduction in A1C, a 6. American Association of Diabetes Educators. Diabetes Advanced
time-in-range increase of about 5%, and an approximate 40% Network Access (DANA). https://www.danaapps.org/. Accessed
February 25, 2019.
decrease in hypoglycemic events.57
7. United States Food & Drug Administration. Mobile Medical Applica-
Despite these benefits, this system is still not a panacea tions. https://www.fda.gov/MedicalDevices/DigitalHealth/MobileMedi-
for people with type 1 diabetes. The user is still required to calApplications/ucm255978.htm. Accessed February 25, 2019.
count carbohydrates and enter this data into the pump, know 8. Health on the Net Foundation. The HON Code of Conduct for medi-
when and how to override the system if warranted, regularly cal and health websites (HONcode). https://www.hon.ch/HON-
change and rotate sites, and troubleshoot issues that may code/Patients/Conduct.html. Accessed February 25, 2019.
9. Singh K, Drouin K, Newmark LP, et al. Developing a framework for
arise (e.g., line occlusions, extreme hyperglycemia, discrep-
evaluating the patient engagement, quality, and safety of mobile
ancies between sensor and calibration value).58 Additional health applications. Issue Brief (Commonw Fund). 2016;5:1–11.
research is ongoing to achieve an ultimate goal in this line of 10. Veazie S, Winchell K, Gilber J, et al. Rapid evidence review of
study: a bionic pancreas that can autonomously administer mobile applications for self-management of diabetes. J Gen Intern
insulin or glucagon depending on the patient’s specific needs Med. 2018;33(7):1167–76.
and that does not require carbohydrate counting.59 11. Bonoto BC, de Araujo VE, Godoi IP, et al. Efficacy of mobile apps
to support the care of patients with diabetes mellitus: a systematic
review and meta-analysis of randomized controlled trials. JMIR
Staying up to date Mhealth Uhealth. 2017;5(3):e4.
As mobile devices and apps become even more prevalent, 12. Hou C, Xu Q, Diao S, et al. Mobile phone applications and self-
they will undoubtedly play an increasingly significant management of diabetes: a systematic review with meta-analysis,
role in helping patients live successfully with diabetes meta-regression of 21 randomized trials and GRADE. Diabetes
and other chronic conditions. Therefore, it is important Obes Metab. 2018;20(8):2009–13.
to stay up to date on advances in this area. This can be 13. Wu Y, Yao X, Vespasiani G, et al. Mobile app-based interventions
to support diabetes self-management: a systematic review of ran-
quite difficult to do. One strategy for staying up to date
domized controlled trials to identify functions associated with gly-
is to ask patients what apps they are seeing, using, or cemic efficacy. JMIR Mhealth Uhealth. 2017;5(3):e35.
hearing about. This will give you an idea of which ones 14. Giugliano D, Maiorino MI, Bellastella G, et al. Clinical inertia, re-
might be more specific to your patient population and verse clinical inertia, and medication non-adherence in type 2 dia-
therefore more beneficial to look into. Another strategy betes. J Endocrinol Invest. 2018;[Epub ahead of print]. doi: 10.1007/
is to check various sources online, including the app clear- s40618-018-0951-8.
15. Khunti K, Nikolajsen A, Thorsted BL, et al. Clinical inertia with re-
inghouses mentioned earlier (e.g., DANA at www.dan-
gard to intensifying therapy in people with type 2 diabetes treated
aapps.org), diabetes-specific blogs and websites (e.g., http:// with basal insulin. Diabetes Obes Metab. 2016;18(4):401–9.
www.diatribe.org), and general websites covering broader 16. Mocarski M, Yeaw J, Divino V, et al. Slow titration and delayed
health-related topics (e.g., http://www.everydayhealth.com/, intensification of basal insulin among patients with type 2 diabetes.
http://www.healthline.com/). J Manag Care Spec Pharm. 2018;24(4):390–400.
54 PharmacyToday • MAY 2019 www.pharmacytoday.org
CPE_05_19_NEW.indd 54 4/23/2019 7:52:56 AM
UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT CPE
17. Strange P. Treat-to-target insulin titration algorithms when initiat- tems. Intern Med. 2018;57(23):3407–12.
ing long or intermediate acting insulin in type 2 diabetes. J Diabe- 37. Lamounier RN, Geloneze B, Leite SO, et al. Hypoglycemia inci-
tes Sci Technol. 2007;1(4):540–8. dence and awareness among insulin-treated patients with diabe-
18. Davies M, Storms F, Shutler S, et al. Improvement of glycemic tes: the HAT study in Brazil. Diabetol Metab Syndr. 2018;10:83.
control in subjects with poorly controlled type 2 diabetes. Diabe- 38. Dexcom. The Dexcom G5 Mobile CGM System. https://www.dex-
tes Care. 2005;28(6):1282–8. com.com/g5-mobile-cgm. Accessed March 25, 2019.
19. WellDoc. BlueStar. https://www.welldoc.com/product/. Accessed 39. Dexcom. Dexcom Coninuous Glucose Monitoring. https://www.
February 25, 2019. dexcom.com/g6-cgm-system. Accessed March 25, 2019.
20. WellDoc. WellDoc receives FDA 510(k) clearance to offer a 40. Medtronic. Guardian Connect CGM. https://www.medtronicdia-
non-prescription version of BlueStar digital therapeutic for type betes.com/products/guardian-connect-continuous-glucose-mon-
2 diabetes. https://www.welldoc.com/news/welldoc-receives- itoring-system. Accessed March 25, 2019.
fda-510k-clearance-to-offer-a-non-prescription-version-of-blue- 41. Abbott. Freestyle Libre. https://www.freestylelibre.us. Accessed
star-digital-therapeutic-for-type-2-diabetes/. Accessed February March 25, 2019.
25, 2019. 42. Senseonics. Eversense. https://www.eversensediabetes.com/
21. Quinn CC, Clough SS, Minor JM, et al. WellDoc mobile diabetes products/. Accessed March 25, 2019.
management randomized controlled trial: change in clinical and 43. Kudva YC, Ahmann AJ, Bergenstal RM, et al. Approach to using
behavioral outcomes and patient and physician satisfaction. Dia- trend arrows in the FreeStyle Libre flash glucose monitoring sys-
betes Technol Ther. 2008;10(3):160–8. tems in adults. J Endocr Soc. 2018;2(12):1320–37.
22. Quinn CC, Shardell MD, Terrin ML, et al. Cluster-randomized trial 44. Laffel LM, Aleppo G, Buckingham BA, et al. A practical ap-
of a mobile phone personalized behavioral intervention for blood proach to using trend arrows on the Dexcom G5 CGM system to
glucose control. Diabetes Care. 2011;34(9):1934–42. manage children and adolescents with diabetes. J Endocr Soc.
23. Kim EK, Kwak SH, Jung HS, et al. The effect of a smartphone- 2017;1(12):1461–76.
based, patient-centered diabetes care system in patients with 45. Liebl A, Henrichs HR, Heinemann L, et al. Continuous glucose
type 2 diabetes: a randomized, controlled trial for 24 weeks. Dia- monitoring: evidence and consensus statement for clinical use. J
betes Care. 2019;42(1):3–9. Diabetes Sci Technol. 2013;7(2):500–19.
24. Quianzon C, Cheikh I. History of insulin. J Community Hosp Intern 46. Rodbard D. Continuous glucose monitoring: a review of recent
Med Perspect. 2012;2(2):10.3402/jchimp.v2i2.18701. studies demonstrating improved glycemic outcomes. Diabetes
25. Clarke SF, Foster JR. A history of blood glucose meters and Technol Ther. 2017;19(Suppl 3):S25–S37.
their role in self-monitoring of diabetes mellitus. Br J Biomed Sci. 47. Meece J. Effect of insulin pen devices on the management of dia-
2012;69(2):83–93. betes mellitus. Am J Health Syst Pharm. 2008;65(11):1076–82.
26. Cefalu WT, Dawes DE, Gavlk G, et al. Insulin access and afford- 48. Truong TH, Nguyen TT, Armor BL, et al. Errors in the adminis-
ability working group: conclusions and recommendations. Diabe- tration technique of insulin pen devices: a result of insufficient
tes Care. 2018;41(6):1299–311. education. Diabetes Ther. 2017;8(2):221–6.
27. Kirk JK, Stegner J. Self-monitoring of blood glucose: practical 49. Bzowyckyj AS. Embracing the insulin revolution in the ambulatory
aspects. J Diabetes Sci Technol. 2010;4(2):435–9. care setting. Diabetes Spectr. 2016;29(3):140–5.
28. Endocrine Society. Position Statement: Access to affordable and 50. Frid AH, Kreugel G, Grassi G, et al. New insulin delivery recom-
adequate diabetes supplies. https://www.endocrine.org/-/media/ mendations. Mayo Clin Proc. 2016;91(9):1231–55.
endosociety/files/advocacy-and-outreach/position-statements/ 51. Novo Nordisk. NovoPen Echo User Guide. https://www.novonord-
all/accesstoaffordableadequatediabetessupplies.pdf?la=en. Ac- isk.com/content/dam/Denmark/HQ/Patients/DiabetesCare/Pen-
cessed February 25, 2019. sNeedlesInjection/novoEcho/NovoPen-Echo-IFU.pdf. Accessed
29. American Diabetes Association. 6. Glycemic targets: Standards February 25, 2019.
of Medical Cere in Diabetes—2019. Diabetes Care. 2019;42(Sup- 52. Diabnext. Clipsulin C3 website. https://www.diabnext.com/insu-
pl 1):S61–S70. lin-clipsulin/. Accessed February 25, 2019.
30. Klonoff DC, Parkes JL, Kovatchev BP, et al. Investigation of the 53. Companion Medical. InPen website. https://www.companionmed-
accuracy of 18 marketed blood glucose monitors. Diabetes Care. ical.com/InPen/. Accessed February 25, 2019.
2018;41(8):1681–8. 54. Medtronic. The Basics of Insulin Pump Therapy. https://www.
31. International Organization for Standardization (ISO). ISO medtronicdiabetes.com/sites/default/files/library/download-library/
15197:2013: in-vitro diagnostic test systems – requirements for workbooks/BasicsofInsulinPumpTherapy.pdf. Accessed March 27,
blood-glucose monitoring systems for self-testing in managing 2019.
diabetes mellitus. https://www.iso.org/standard/54976.html. Ac- 55. American Diabetes Association. Diabetes Forecast Consumer
cessed February 25, 2019. Guide 2019. http://main.diabetes.org/dforg/pdfs/2019/2019-cg-
32. United States Food & Drug Administration. Self-monitoring blood insulin-pumps.pdf. Accessed March 27, 2019.
glucose test systems for over-the-counter use: guidance for in- 56. Tauschmann M, Hovorka R. Insulin delivery and nocturnal glu-
dustry and Food and Drug Administration staff. https://www.fda. cose control in children and adolescents with type 1 diabetes.
gov/downloads/ucm380327.pdf. Accessed February 25, 2019. Expert Opin Drug Deliv. 2017;14(12):1367–77.
33. Diabetes Technology Society (DTS). Blood Glucose Monitor- 57. Garg SK, Weinzimer SA, Tamborlane WV, et al. Glucose out-
ing System (BGMS) Surveillance Program. https://www.diabe- comes with the in-home use of a hybrid closed-loop insulin de-
testechnology.org/surveillance.shtml. Accessed February 25, livery system in adolescents and adults with type 1 diabetes.
2019. Diabetes Technol Ther. 2017;19(3):155–63.
34. Dolson L. How to test your blood with a home ketone meter. 58. Scheiner G. 670G and me: Insights and incites on Medtronic’s lat-
https://www.verywellhealth.com/how-to-test-your-blood-for-ke- est system. http://integrateddiabetes.com/670g-and-me-insights-
tones-2241625. Accessed February 25, 2019. and-incites-on-medtronics-latest-system/. Accessed February
35. Klonoff DC, Ahn D, Drincic A. Continuous glucose monitoring: 25, 2019.
a review of the technology and clinical use. Diabetes Res Clin 59. El-Khatib FH, Balliro C, Hillard MA, et al. Home use of a bihor-
Pract. 2017;133:178–92. monal bionic pancreas versus insulin pump therapy in adults with
36. Sugawa T, Murakami T, Yabe D, et al. Hypoglycemia unaware- type 1 diabetes: a multicenter randomized crossover trial. Lancet.
ness in insulinoma revealed with flash glucose monitoring sys- 2017;389(10067):369–80.
www.pharmacist.com MAY 2019 • PharmacyToday 55
CPE_05_19_JD.indd 55 4/22/2019 4:42:26 PM
CPE UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT
CPE assessment
This assessment must be taken online; please see “CPE information” in the sidebar below for further instructions. The
online system will present these questions in random order to help reinforce the learning opportunity. There is only one
correct answer to each question.
1. A patient with type 2 diabetes (on oral medications 4. Which of the following functionalities is only avail-
only) is looking for an app that can help her track her able in the prescription version of the WellDoc Blue-
calories and exercise. She would like something that Star app?
is easy to use and free, and she doesn’t want or need a. Diabetes education videos
extra features. Which app would be most appropriate b. Insulin dose calculator
to discuss with her? c. Tailored coaching messages
a. MyFitnessPal d. Weekly challenges to engage users
b. KingFit
c. MyNetDiary Diabetes Tracker 5. Scientific evidence suggests that use of commercially
d. Insulia available apps
a. May improve some short-term diabetes-related out-
2. A patient with type 2 diabetes is started on insulin comes such as A1C
glargine U-300 at 10 units once daily. Which of the fol- b. Are only effective when combined with frequent
lowing apps can help him titrate his basal insulin to a support from a health care provider
safe and effective dose? c. Improve quality of life but do not improve other
a. Fooducate diabetes-related outcomes
b. Glooko d. Improve A1C in patients with type 2 diabetes but not
c. Insulia in patients with type 1 diabetes
d. Glucose Buddy
6. Which one of the following patients can benefit most
3. A patient with type 1 diabetes is interested in finding from using a mobile app to help manage their
a free app that can help him log several diabetes-re- diabetes?
lated data points (i.e., glucose, insulin doses, carbohy- a. A 64-year-old woman with type 1 diabetes who does
drate intake) and also help him decide the appropriate not own a smartphone
dose to administer with meals based on his glucose b. A 43-year-old man who is in denial about his type 2
patterns. Which of the following apps is most appro- diabetes diagnosis
priate for this patient? c. A 37-year-old woman with type 2 diabetes who is
a. mySugr legally blind in both eyes
b. Health2Sync d. A 52-year-old man with type 2 diabetes who is into
c. MyNetDiary Diabetes Tracker wearable technology
d. PredictBGL Insulin Dose Calc
CPE information
To obtain the 2.0 contact hours (0.2 CEUs) of To claim credit Assistance is available Monday through Friday
CPE credit for this activity, you must complete 1. Go to http://apha.us/CPE0519. from 8:30 am to 5:00 pm ET at APhA InfoCenter
the online assessment with a passing grade 2. Log in to your APhA account or register as a at 800-237-APhA (2742) or by e-mailing info-
of 70% or better, complete the evaluation, and new user. center@aphanet.org.
CLAIM CREDIT at http://apha.us/CPE0519. 3. Select “Enroll Now” or “Add to Cart” (click
You will have two opportunities to successfully “View Cart” and “Check Out”).
complete the assessment, and the questions 4. Complete the assessment and evaluation.
will be in randomized order. The current policy 5. Click “Claim Credit.” You will need to provide
of the APhA Education Department is not to your NABP e-profile ID number to obtain and
release the correct answers to any of our CPE print your statement of credit.
tests. This policy is intended to maintain the
integrity of the CPE activity. Learners who suc-
cessfully complete this activity by the expiration
date can receive CPE credit. Please visit CPE
Monitor for your statement of credit/transcript.
56 PharmacyToday • MAY 2019 www.pharmacytoday.org
CPE_05_19_JD.indd 56 4/22/2019 4:42:45 PM
UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT CPE
7. Which of the following accurately describes the best c. Glucometer value is within 10 mg/dL of a reference
approach to enhancing diabetes care with use of plasma value for values below 70 mg/dL.
apps? d. Glucometer value is within 25 mg/dL of a reference
a. Advise patients to avoid using apps that are not ap- plasma value for values above 200 mg/dL.
proved by FDA.
b. Identify other apps that a patient may be using to 13. Which of the following is correct about the accuracy of
sync up with the app. continuous glucose monitoring (CGM) devices?
c. Recommend to patients three to four apps that are a. Abbott Freestyle Libre requires calibration twice daily.
your personal favorites. b. Senseonics Eversense requires a 2-hour warm-up
d. Refer patients to apps that rely solely on automated before reporting data.
feedback from the app. c. Medtronic Guardian Connect requires calibration
every 12 hours.
8. A patient heard from a friend about a new app that d. Dexcom G6 sensors can be worn for only 7 days
seems too good to be true. She is thinking about pur- before needing replacement.
chasing it but is not sure if it is worth the high upfront
cost. Which of the following sources of information 14. Which of the following CGM systems is considered a
would be the most helpful for her decision? flash CGM device?
a. iTunes App Store User Ratings a. Dexcom G6
b. FDA Medical Device Database b. Guardian Connect
c. iMedicalApps Clearinghouse c. Eversense
d. National Library of Medicine Mobile Apps d. FreeStyle Libre
9. Which of the following characteristics describes one 15. A patient at your pharmacy has a daughter with type 1
of the core HONcode principles of the Health On the diabetes. She heard on the news that an artificial pan-
Net Foundation? creas was recently approved by FDA. She is excited
a. Attribution about the idea but has some questions. Which of the
b. User ratings following most correctly describes what is currently
c. Functionality available for patients as an artificial pancreas?
d. Update frequency a. A fully automated insulin pump/CGM system that
allows the patient to be completely hands-off
10. Which of the following is important to consider when b. A hybrid, closed-loop insulin pump/CGM system
evaluating an app’s online user ratings? that automatically adjusts basal insulin delivery
a. Read only those reviews from people who rated the based on CGM data
app poorly. c. A partially automated insulin pump/CGM system
b. Read only those reviews from people who rated the that alerts the patient if CGM data indicate the pa-
app highly. tient is hypoglycemic
c. Read a mix of reviews from people who rated it d. A combination system that includes an insulin
highly and poorly. pump and a CGM, but the two devices do not inte-
d. Do not read the reviews; just focus on the numerical grate for clinical decision-making purposes
rating to save time.
16. Which of the following meters contains the functional-
11. Which of the following glucometers received a seal ity to test blood samples for both glucose and ketones?
of approval based on the results of the 2018 Diabetes a. Precision Xtra
Technology Society (DTS) Blood Glucose Monitor b. OneTouch Ultra2
System (BGMS) Surveillance Program? c. Accu-Chek Aviva Plus
a. TrueTrack d. Bayer Contour Next EZ
b. One Touch Ultra2
c. Prodigy AutoCode 17. CGM would be most beneficial for which one of the
d. Accu-Chek Aviva Plus following patients with type 2 diabetes?
a. A patient on multiple daily insulin injections and
12. Which of the following correctly describes the with hypoglycemia unawareness
standard used during the DTS BGMS Surveillance b. A patient taking metformin and a sulfonylurea who
Program? occasionally experiences nocturnal hypoglycemia
a. Glucometer value is within 5% of a reference plasma c. A patient who has a glucose log that is consistent
value for values below 150 mg/dL. with her or his most recent A1C
b. Glucometer value is within 15% of a reference d. A patient who is legally blind in both eyes with no
plasma value for all values above 100 mg/dL. permanent caregiver living with her or him
www.pharmacist.com MAY 2019 • PharmacyToday 57
CPE_05_19_NEW.indd 57 4/23/2019 8:48:34 AM
CPE UPDATES AND ADVANCES IN TECHNOLOGY FOR DIABETES SELF-MANAGEMENT
18. Which of the following statements is true about dis- 20. Which of the following devices is able to record the
posable insulin pen devices? times and amounts of insulin doses administered on
a. Can deliver insulin in half-unit increments a Bluetooth-paired smartphone app?
b. Can track the time of the last insulin dose to prevent a. NovoPen Echo
stacking b. Clipsulin C3
c. Should be stored without a pen needle attached c. Solostar Max
d. Can integrate with smartphone apps to deliver ac- d. FlexTouch
curate insulin doses based on carb-to-insulin ratios
and correction factors
19. Which of the following statements accurately repre-
sents the rationale for avoiding needles longer than 8
mm in adults when administering insulin injections?
a. Decreased cost associated with shorter needles
b. Higher amount of insulin wasted to prime longer
needles
c. Decreased perception of pain when administering
longer needles
d. Increased risk of variable insulin absorption with
longer needles
58 PharmacyToday • MAY 2019 www.pharmacytoday.org
CPE_05_19_JD.indd 58 4/22/2019 4:43:27 PM
S-ar putea să vă placă și
- Clinical Pharmacology in Healthcare, Teaching and ResearchDocument80 paginiClinical Pharmacology in Healthcare, Teaching and ResearchVNcomer100% (1)
- Nurse ExamDocument17 paginiNurse ExamRn nadeen100% (2)
- Hospital PharmacyDocument81 paginiHospital Pharmacypmily100% (9)
- Division of Malabon City Cluster Meet 2017: Black BlackDocument1 paginăDivision of Malabon City Cluster Meet 2017: Black BlackJuan Miguel PangilinanÎncă nu există evaluări
- SyllabusDocument2.235 paginiSyllabuselkaramanyÎncă nu există evaluări
- Safety Officer Resume - 6+ Years HSE ExperienceDocument3 paginiSafety Officer Resume - 6+ Years HSE ExperienceMuhammad Zeeshan Ahmed100% (1)
- How To Use Aquatabs - AfricaDocument1 paginăHow To Use Aquatabs - AfricaJuan Miguel PangilinanÎncă nu există evaluări
- Pharmacovigilance Blue BookDocument198 paginiPharmacovigilance Blue Bookparam540100% (1)
- Kap QuestionnaireDocument10 paginiKap QuestionnaireSowmi AnitaÎncă nu există evaluări
- JCI Whitepaper Cpgs Closing The GapDocument12 paginiJCI Whitepaper Cpgs Closing The GapMathilda UllyÎncă nu există evaluări
- DayTwo Microbiome App StrategyDocument10 paginiDayTwo Microbiome App Strategyap123 dklÎncă nu există evaluări
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsDe la EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsÎncă nu există evaluări
- Pharmacovigilance and Clinical ResearchDocument47 paginiPharmacovigilance and Clinical Researchdadimma100% (1)
- Drug Study - Hepatitis B VaccineDocument2 paginiDrug Study - Hepatitis B VaccineJustin AncogÎncă nu există evaluări
- Patient Apps For Improved HealthcareDocument65 paginiPatient Apps For Improved HealthcareojuÎncă nu există evaluări
- Ciy 745Document35 paginiCiy 745Fátima CarrascoÎncă nu există evaluări
- Ciy745 PDFDocument35 paginiCiy745 PDFPhúc LâmÎncă nu există evaluări
- Guias de InfeccionDocument35 paginiGuias de Infeccionjose quintanillaÎncă nu există evaluări
- Dionne, 2022 - Which Pharmacists Are Performing Antimicrobial StewardshipDocument7 paginiDionne, 2022 - Which Pharmacists Are Performing Antimicrobial StewardshipThuane SalesÎncă nu există evaluări
- 54e400890cf282dbed6e77d1 2Document6 pagini54e400890cf282dbed6e77d1 2Naela RizqiÎncă nu există evaluări
- MateriDocument25 paginiMateriRefki Okta TriadiÎncă nu există evaluări
- COV-19 GuidelinesDocument187 paginiCOV-19 GuidelinesRizky GumelarÎncă nu există evaluări
- Otc Advisor 1 - The Pharmacists Role in Self CareDocument20 paginiOtc Advisor 1 - The Pharmacists Role in Self CareNurhasna Sushmita SariÎncă nu există evaluări
- Metolitodologi PenelitianDocument11 paginiMetolitodologi PenelitianAyu Kurnia Kemala SariÎncă nu există evaluări
- Biblio Comp Guias Rol Farmaceutico en Gestion Informacion - ASHP - 2015Document5 paginiBiblio Comp Guias Rol Farmaceutico en Gestion Informacion - ASHP - 2015Lula BilloudÎncă nu există evaluări
- Idsa Covid 19 GL TX and MGMT v8.0.0Document232 paginiIdsa Covid 19 GL TX and MGMT v8.0.0Miguel VillalobosÎncă nu există evaluări
- Medication Safety: Protection Versus Production: Live Activity HandoutDocument56 paginiMedication Safety: Protection Versus Production: Live Activity HandoutOm PatelÎncă nu există evaluări
- Abx DosingDocument16 paginiAbx DosingckeshavaÎncă nu există evaluări
- General Psychiatry: Harmacy Ompetency Ssessment EnterDocument11 paginiGeneral Psychiatry: Harmacy Ompetency Ssessment EnterJeremy HamptonÎncă nu există evaluări
- Embedded R D China Interv Trial AMR 29.05.2019 V1aDocument17 paginiEmbedded R D China Interv Trial AMR 29.05.2019 V1aAnonymous gVgLS4Încă nu există evaluări
- A Case-Based Monograph Focusing On Pediatric IBD: FacultyDocument12 paginiA Case-Based Monograph Focusing On Pediatric IBD: FacultyVijayakanth VijayakumarÎncă nu există evaluări
- Recent Abstracts MPH 65 2020 NUTDocument3 paginiRecent Abstracts MPH 65 2020 NUTHasriniÎncă nu există evaluări
- 13 173 JordanProphylaxisCesareanSection - No PptsDocument84 pagini13 173 JordanProphylaxisCesareanSection - No Pptsnurul wahyuniÎncă nu există evaluări
- Digital Diabetes Management Tools US Healthcare 1711594288Document51 paginiDigital Diabetes Management Tools US Healthcare 1711594288atchyuth manindraÎncă nu există evaluări
- Do Not Copy Penalties Apply: Cosmetic Benefits of Natural IngredientsDocument9 paginiDo Not Copy Penalties Apply: Cosmetic Benefits of Natural IngredientsNgoc HaÎncă nu există evaluări
- Producing Competent Physicians - More Paper Work or IndeedDocument48 paginiProducing Competent Physicians - More Paper Work or Indeedapi-26176346Încă nu există evaluări
- Rapid Evidence Review of Mobile Applications For Self-Management of DiabetesDocument10 paginiRapid Evidence Review of Mobile Applications For Self-Management of DiabetesNersdilahÎncă nu există evaluări
- International Journal of Pharmacy Practice AbstractsDocument40 paginiInternational Journal of Pharmacy Practice AbstractsFabiola NogaÎncă nu există evaluări
- ssp articleDocument6 paginissp articleapi-740259455Încă nu există evaluări
- Streamline Your Office VisitsDocument5 paginiStreamline Your Office VisitsnpÎncă nu există evaluări
- Postgraduate and SpecializationDocument78 paginiPostgraduate and SpecializationAįmz DìvşÎncă nu există evaluări
- Idsa Covid 19 GL TX and MGMT v4.4.1Document173 paginiIdsa Covid 19 GL TX and MGMT v4.4.1Galaxy SatwaÎncă nu există evaluări
- 2021 Bald Et. Al - Usar EsseDocument7 pagini2021 Bald Et. Al - Usar EsseLuanna ResendeÎncă nu există evaluări
- Pharmacovigilance in India - A PerspectiveDocument4 paginiPharmacovigilance in India - A PerspectiveVijay Venkatraman JanarthananÎncă nu există evaluări
- Drug Information Centers - Need of The Hour: March 2011Document9 paginiDrug Information Centers - Need of The Hour: March 2011Shayan MaryamÎncă nu există evaluări
- Engineer's Choice: Solution Development For Advancing Health Informatics 1Document12 paginiEngineer's Choice: Solution Development For Advancing Health Informatics 1api-542948601Încă nu există evaluări
- A. Pozza, A. Coluccia, G. Gualtieri, F. FerrettiDocument7 paginiA. Pozza, A. Coluccia, G. Gualtieri, F. FerrettiGabyMaría DelValle Cordero Gómez ⃝⃤Încă nu există evaluări
- Corrected PicotDocument8 paginiCorrected Picotjosephmainam9Încă nu există evaluări
- Atu Kenechukwu FINAL YEAR PROJECT 222 (ALPHA) (AutoRecovered)Document21 paginiAtu Kenechukwu FINAL YEAR PROJECT 222 (ALPHA) (AutoRecovered)Kenny AtuÎncă nu există evaluări
- ISMP RTA Webinar Handouts 2024 - 0Document33 paginiISMP RTA Webinar Handouts 2024 - 0JyotiÎncă nu există evaluări
- 0514 Acute Otitis MediaDocument12 pagini0514 Acute Otitis MediaRozaÎncă nu există evaluări
- Pharmacovigilance: Masterkey To Drug Safety Monitoring and Its Status in IndiaDocument4 paginiPharmacovigilance: Masterkey To Drug Safety Monitoring and Its Status in IndiaSejal khumanÎncă nu există evaluări
- Pharmacy Daily For Mon 09 Sep 2013 - Registration Audit, FIP Education Report, E-Cigarettes, Generics and Much MoreDocument3 paginiPharmacy Daily For Mon 09 Sep 2013 - Registration Audit, FIP Education Report, E-Cigarettes, Generics and Much MorepharmacydailyÎncă nu există evaluări
- The Use of Smartphone Health Apps and Other Mobile Health (Mhealth) Technologies in Dietetic Practice - A Three Country StudyDocument14 paginiThe Use of Smartphone Health Apps and Other Mobile Health (Mhealth) Technologies in Dietetic Practice - A Three Country StudyUmialqyÎncă nu există evaluări
- CME Accreditation Page - EmcDocument2 paginiCME Accreditation Page - EmcFritz BoyaÎncă nu există evaluări
- 1 s2.0 S016926071931154X Main 1Document7 pagini1 s2.0 S016926071931154X Main 1wmn94Încă nu există evaluări
- 3 Medication AdherenceDocument19 pagini3 Medication AdherenceKrishelle Anne ObispoÎncă nu există evaluări
- Idsa COVIDDocument138 paginiIdsa COVIDkeylapireÎncă nu există evaluări
- Evaluating Cost of Pharmaceuticals CEADocument26 paginiEvaluating Cost of Pharmaceuticals CEAnurhayati novitaÎncă nu există evaluări
- Guia Idsa Manejo de Pacientes Covid-19Document61 paginiGuia Idsa Manejo de Pacientes Covid-19Paola RodriguezÎncă nu există evaluări
- Competency Assessment Module - Advanced Antimicrobial StewardshipDocument13 paginiCompetency Assessment Module - Advanced Antimicrobial StewardshipJeremy HamptonÎncă nu există evaluări
- Atu Kenechukwu FINAL YEAR PROJECT 222 (ALPHA) (AutoRecovered) (Repaired)Document22 paginiAtu Kenechukwu FINAL YEAR PROJECT 222 (ALPHA) (AutoRecovered) (Repaired)Kenny AtuÎncă nu există evaluări
- CME Accreditation Page 2015 Emergency Medicine Clinics of North AmericaDocument2 paginiCME Accreditation Page 2015 Emergency Medicine Clinics of North Americayorlis00Încă nu există evaluări
- Mobile Paper 1 Mhealth SLR PDFDocument10 paginiMobile Paper 1 Mhealth SLR PDFJules RosataseÎncă nu există evaluări
- A Case Study in Open Source Innovation: Developing The Tidepool Platform For Interoperability in Type 1 Diabetes ManagementDocument9 paginiA Case Study in Open Source Innovation: Developing The Tidepool Platform For Interoperability in Type 1 Diabetes ManagementJoseSolorzanoCabreraÎncă nu există evaluări
- Patient Education and Counseling: Juliana Chen, Luke Gemming, Rhona Hanning, Margaret Allman-FarinelliDocument8 paginiPatient Education and Counseling: Juliana Chen, Luke Gemming, Rhona Hanning, Margaret Allman-FarinelliAlvaro PalominoÎncă nu există evaluări
- Aarogya Margdarsh - Medical Camp Related Mobile AppDocument5 paginiAarogya Margdarsh - Medical Camp Related Mobile AppInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- MSD - SparshDocument10 paginiMSD - SparshGiridhar GaneshÎncă nu există evaluări
- Lindores Abbey Stars Cupar SCO 2019Document7 paginiLindores Abbey Stars Cupar SCO 2019Juan Miguel PangilinanÎncă nu există evaluări
- Highlights: 2017 G P, D, e M H B P ADocument2 paginiHighlights: 2017 G P, D, e M H B P AJamie LittleÎncă nu există evaluări
- WHO RHR 18.14 Eng PDFDocument4 paginiWHO RHR 18.14 Eng PDFJuan Miguel PangilinanÎncă nu există evaluări
- Robson Classification - Implementation ManualDocument56 paginiRobson Classification - Implementation ManualJuan Miguel PangilinanÎncă nu există evaluări
- WEB CIOMS Communication Guide 2018Document80 paginiWEB CIOMS Communication Guide 2018Juan Miguel PangilinanÎncă nu există evaluări
- UNFPA - Comprehensive Midwifery Programme Guidance 2014Document53 paginiUNFPA - Comprehensive Midwifery Programme Guidance 2014Juan Miguel PangilinanÎncă nu există evaluări
- Knowledge, Attitude and Practice of Pharmacovigilance Among Community Pharmacists in Delhi, IndiaDocument6 paginiKnowledge, Attitude and Practice of Pharmacovigilance Among Community Pharmacists in Delhi, IndiaJuan Miguel PangilinanÎncă nu există evaluări
- Robson Classification ExampleDocument11 paginiRobson Classification ExampleJuan Miguel PangilinanÎncă nu există evaluări
- WHO Assesing and Managing Children Obesity-EngDocument88 paginiWHO Assesing and Managing Children Obesity-EngsofiabloemÎncă nu există evaluări
- Cholesterol GuidelinesDocument2 paginiCholesterol GuidelinesJuan Miguel PangilinanÎncă nu există evaluări
- Pi Is 1042099119304979Document1 paginăPi Is 1042099119304979Juan Miguel PangilinanÎncă nu există evaluări
- PatientCareProcess With Supporting OrganizationsDocument6 paginiPatientCareProcess With Supporting OrganizationsJuan Miguel PangilinanÎncă nu există evaluări
- At-Home Diagnostic and Monitoring Tests - The Good and The BadDocument2 paginiAt-Home Diagnostic and Monitoring Tests - The Good and The BadJuan Miguel PangilinanÎncă nu există evaluări
- Pharmacists' Guide to OsteoarthritisDocument8 paginiPharmacists' Guide to OsteoarthritisJuan Miguel PangilinanÎncă nu există evaluări
- Update and Advances in Technology For Diabetes Self ManagementDocument6 paginiUpdate and Advances in Technology For Diabetes Self ManagementJuan Miguel PangilinanÎncă nu există evaluări
- FIDE Grand Prix 2019 RegulationsDocument11 paginiFIDE Grand Prix 2019 RegulationsJuan Miguel PangilinanÎncă nu există evaluări
- 12-Dose TB Treatment ExplainedDocument2 pagini12-Dose TB Treatment ExplainedJuan Miguel PangilinanÎncă nu există evaluări
- How To Use Aquatabs - PhilippinesDocument1 paginăHow To Use Aquatabs - PhilippinesJuan Miguel PangilinanÎncă nu există evaluări
- Your Medication Schedule: The 12-Dose Regimen For Latent Tuberculosis (TB) InfectionDocument2 paginiYour Medication Schedule: The 12-Dose Regimen For Latent Tuberculosis (TB) InfectionJuan Miguel PangilinanÎncă nu există evaluări
- DOH National TB Control Program - PhilippinesDocument5 paginiDOH National TB Control Program - PhilippinesJuan Miguel PangilinanÎncă nu există evaluări
- Ivanchuk Wins His 8th Capablanca MemorialDocument6 paginiIvanchuk Wins His 8th Capablanca MemorialJuan Miguel PangilinanÎncă nu există evaluări
- WHO Guidelines On Tuberculosis Infection, Prevention and Control - 2019 Update PDFDocument72 paginiWHO Guidelines On Tuberculosis Infection, Prevention and Control - 2019 Update PDFJuan Miguel PangilinanÎncă nu există evaluări
- Computer Packages Amd RyzenDocument4 paginiComputer Packages Amd RyzenJuan Miguel PangilinanÎncă nu există evaluări
- Computer Packages Amd RyzenDocument4 paginiComputer Packages Amd RyzenJuan Miguel PangilinanÎncă nu există evaluări
- Solar PackageDocument2 paginiSolar PackageJuan Miguel PangilinanÎncă nu există evaluări
- 6610 Assignment 4Document19 pagini6610 Assignment 4gyanendraÎncă nu există evaluări
- Physio Assess Form Oct 2022Document5 paginiPhysio Assess Form Oct 2022RishaadÎncă nu există evaluări
- IBM India Benefits - Emergency Transport Assistance GuidelinesDocument6 paginiIBM India Benefits - Emergency Transport Assistance GuidelinesSushovan NandiÎncă nu există evaluări
- PHILIPPINE HEALTH CARE PROVIDERS INC. vs. CIRDocument17 paginiPHILIPPINE HEALTH CARE PROVIDERS INC. vs. CIRDenee Vem MatorresÎncă nu există evaluări
- INITIAL DATA BASE Form For Family 1Document5 paginiINITIAL DATA BASE Form For Family 1Reignallienn Inocencio MartinÎncă nu există evaluări
- LRT (Light Rapid Transit) Pulo Gadung Accident Report 1. Description 1.1 Chronology of AccidentDocument4 paginiLRT (Light Rapid Transit) Pulo Gadung Accident Report 1. Description 1.1 Chronology of AccidentYogi GuntaraÎncă nu există evaluări
- PAR-Q Physical Activity Readiness QuestionnaireDocument3 paginiPAR-Q Physical Activity Readiness QuestionnaireMhervin BisisÎncă nu există evaluări
- Age Related ChangesDocument8 paginiAge Related ChangesEricson CandelariaÎncă nu există evaluări
- STIs O & GDocument59 paginiSTIs O & GNoraÎncă nu există evaluări
- Furosemide Drug ProfileDocument34 paginiFurosemide Drug ProfileNur Ilmi SofiahÎncă nu există evaluări
- NO Nama Pasien Tanggal Rujukan/Tujuan RsDocument44 paginiNO Nama Pasien Tanggal Rujukan/Tujuan RsfennyÎncă nu există evaluări
- Transgender Health and Rights Indonesia GWL-INADocument18 paginiTransgender Health and Rights Indonesia GWL-INAJihane YUKKÎncă nu există evaluări
- Food Contact Materials FDA NSF and Other StandardsDocument3 paginiFood Contact Materials FDA NSF and Other StandardsMuhammad Brilian Syifa HabibiÎncă nu există evaluări
- 243 471 1 SM PDFDocument6 pagini243 471 1 SM PDFFia lutfiahÎncă nu există evaluări
- Causes and Treatment of Onychauxis or Nail HypertrophyDocument3 paginiCauses and Treatment of Onychauxis or Nail HypertrophyKathleen BazarÎncă nu există evaluări
- University of Caloocan City: Bachelor of Arts Major in Political Science The Problem and Its BackgroundDocument7 paginiUniversity of Caloocan City: Bachelor of Arts Major in Political Science The Problem and Its BackgroundJericko Perez AvilaÎncă nu există evaluări
- Assignment 2 - Assignment Problem Tree AnalysisDocument2 paginiAssignment 2 - Assignment Problem Tree AnalysissadeadamÎncă nu există evaluări
- Activity Sheet in Food Processing Grade 11 Quarter 1, Week 4 & 5Document4 paginiActivity Sheet in Food Processing Grade 11 Quarter 1, Week 4 & 5Gabriel CabansagÎncă nu există evaluări
- COVID-19 Vaccine Arrives in IndonesiaDocument3 paginiCOVID-19 Vaccine Arrives in Indonesiawawan budiantoÎncă nu există evaluări
- HIV Testing and Management in IndonesiaDocument31 paginiHIV Testing and Management in IndonesiayurdiansyahÎncă nu există evaluări
- Disaster Readiness and Risk Reduction: Quarter 1-Module 3: Disasters and Its EffectsDocument11 paginiDisaster Readiness and Risk Reduction: Quarter 1-Module 3: Disasters and Its EffectsRenzelle Guilaran GerocheÎncă nu există evaluări
- Maternal and Child Health CareDocument12 paginiMaternal and Child Health CarePraachii SharmaÎncă nu există evaluări
- The New Jose L. Amante Emergency HospitalDocument29 paginiThe New Jose L. Amante Emergency HospitalRiah Ramirez FojasÎncă nu există evaluări
- Pediatric Schedule 3Document12 paginiPediatric Schedule 3Luis NepomucenoÎncă nu există evaluări
- Development of Protein Rich Flavored BarDocument6 paginiDevelopment of Protein Rich Flavored BarIJRASETPublicationsÎncă nu există evaluări
- New 2014 Joint Commission Accreditation Standards For Diagnostic Imaging Services - Ambulatory Care CentersDocument6 paginiNew 2014 Joint Commission Accreditation Standards For Diagnostic Imaging Services - Ambulatory Care CentersaegysabetterwayÎncă nu există evaluări