S-ar putea să vă placă și
- Plague Dystopias Volume Six: The Black Death & the Dancing ManiaDe la EverandPlague Dystopias Volume Six: The Black Death & the Dancing ManiaÎncă nu există evaluări
- Who Discovered Hemophilia?: Abdul Nasser Kaadan MD, PHD, Mahmud Angrini MDDocument9 paginiWho Discovered Hemophilia?: Abdul Nasser Kaadan MD, PHD, Mahmud Angrini MDMOHAMMAD TARIQ CHADHARÎncă nu există evaluări
- The History of the World in 100 Pandemics, Plagues and EpidemicsDe la EverandThe History of the World in 100 Pandemics, Plagues and EpidemicsEvaluare: 5 din 5 stele5/5 (1)
- The Early Yeqrs, 1564-LsbsDocument5 paginiThe Early Yeqrs, 1564-LsbsgslauraÎncă nu există evaluări
- Protocols 1stDocument7 paginiProtocols 1sttiahamyÎncă nu există evaluări
- The Emperor's New Clothes: EssayDocument5 paginiThe Emperor's New Clothes: EssayAndy BerdóÎncă nu există evaluări
- The Plague of 1665: Daniel Defoe’s Journal of the Plague Year and other contemporary accountsDe la EverandThe Plague of 1665: Daniel Defoe’s Journal of the Plague Year and other contemporary accountsÎncă nu există evaluări
- Psy5995 6421Document4 paginiPsy5995 6421KingroyÎncă nu există evaluări
- Biography of Karl LandsteinerDocument3 paginiBiography of Karl LandsteinerZairin ZulaikhaÎncă nu există evaluări
- Bio4844 9712Document4 paginiBio4844 9712belajarÎncă nu există evaluări
- Hist8357 6985Document4 paginiHist8357 6985umi pukÎncă nu există evaluări
- This Content Downloaded From 195.114.150.19 On Sun, 03 Oct 2021 16:08:47 UTCDocument11 paginiThis Content Downloaded From 195.114.150.19 On Sun, 03 Oct 2021 16:08:47 UTCFredgar22Încă nu există evaluări
- In the Wake of the Plague: The Black Death and the World It MadeDe la EverandIn the Wake of the Plague: The Black Death and the World It MadeEvaluare: 3.5 din 5 stele3.5/5 (373)
- Genealogy of The Bliss Family in AmericaDocument820 paginiGenealogy of The Bliss Family in Americavwindrow7070Încă nu există evaluări
- Bio3776 7461Document4 paginiBio3776 7461sandraÎncă nu există evaluări
- A Doctor at War: The story of Colonel Martin Herford - the most decorated doctor of World War IIDe la EverandA Doctor at War: The story of Colonel Martin Herford - the most decorated doctor of World War IIÎncă nu există evaluări
- Barlow, King's EvilDocument26 paginiBarlow, King's Evilliuy921Încă nu există evaluări
- Narratives of the New England Witchcraft CasesDe la EverandNarratives of the New England Witchcraft CasesEvaluare: 3 din 5 stele3/5 (1)
- PBL 2-Historical Review ArticalDocument8 paginiPBL 2-Historical Review ArticalCeazaan Nezreen MosesÎncă nu există evaluări
- EFA Pembahasan Strategi 4 ReadingDocument24 paginiEFA Pembahasan Strategi 4 ReadingFitria AndrinaÎncă nu există evaluări
- A study guide for Daniel Defoe's "A Journal of the Plague Year"De la EverandA study guide for Daniel Defoe's "A Journal of the Plague Year"Încă nu există evaluări
- Uas7455 6708Document4 paginiUas7455 6708Bagas KaraÎncă nu există evaluări
- The Black Death The Dancing ManiaDe la EverandThe Black Death The Dancing ManiaÎncă nu există evaluări
- HemophiliaDocument5 paginiHemophiliaGlen Norwel LabayogÎncă nu există evaluări
- 6519432592 (1)Document8 pagini6519432592 (1)tomifrasheriÎncă nu există evaluări
- Biographical Notes: Aristotle BC)Document18 paginiBiographical Notes: Aristotle BC)Anonymous 2Dl0cn7Încă nu există evaluări
- The Parisian-Epistle To Albertus Otho FaberDocument4 paginiThe Parisian-Epistle To Albertus Otho FaberMiguel López PérezÎncă nu există evaluări
- Fa 21 RomanovassignmentDocument5 paginiFa 21 Romanovassignmentapi-583026766Încă nu există evaluări
- Bio 1009Document4 paginiBio 1009Armielyn PagaduanÎncă nu există evaluări
- Chem818 2701Document4 paginiChem818 2701John Linel D. DakingkingÎncă nu există evaluări
- Donahue 2010Document20 paginiDonahue 2010Μαρία ΓιαννούÎncă nu există evaluări
- Math2267 8477Document4 paginiMath2267 8477RAMIARÎncă nu există evaluări
- Chem7582 1395Document4 paginiChem7582 1395Bagus WahyudiÎncă nu există evaluări
- Psy7132 8726Document4 paginiPsy7132 8726amira najwaÎncă nu există evaluări
- History of Cholera: THE IN EthiopiaDocument8 paginiHistory of Cholera: THE IN EthiopiaHaile ManÎncă nu există evaluări
- Chem3130 1325Document4 paginiChem3130 1325Shinta AmalyaÎncă nu există evaluări
- Haemophelia Case StudyDocument8 paginiHaemophelia Case StudyPetro BricalliÎncă nu există evaluări
- Chem2135 3979Document4 paginiChem2135 3979StefiÎncă nu există evaluări
- John Randlett BIOL-294 Romanov Assignment April 22, 2022 HistoryDocument10 paginiJohn Randlett BIOL-294 Romanov Assignment April 22, 2022 Historyapi-608249881Încă nu există evaluări
- Class NotesDocument18 paginiClass NotesPrachi100% (1)
- Typhoid Spine: Somatic Versus Psychosomatic Diagnosis in Osler's TimeDocument10 paginiTyphoid Spine: Somatic Versus Psychosomatic Diagnosis in Osler's Timeaji gumelarÎncă nu există evaluări
- Chem4799 2730Document4 paginiChem4799 2730Just MeÎncă nu există evaluări
- Acc9189 8327Document4 paginiAcc9189 8327FəŕđîÎncă nu există evaluări
- Eng967 4317Document4 paginiEng967 4317Joke JokerÎncă nu există evaluări
- Medicine in ShakespeareDocument106 paginiMedicine in ShakespeareFernanda MelémÎncă nu există evaluări
- Bio783 1530Document4 paginiBio783 1530Nezer VergaraÎncă nu există evaluări
- Blood at 70: Its Roots in The History Of: Hematology and Its BirthDocument5 paginiBlood at 70: Its Roots in The History Of: Hematology and Its Birthslim boukhrisÎncă nu există evaluări
- Hist3465 7483Document4 paginiHist3465 7483Rai FazranÎncă nu există evaluări
- Bio9370 5824Document4 paginiBio9370 5824Arvin FernandezÎncă nu există evaluări
- Book Review (HIS Sp23)Document7 paginiBook Review (HIS Sp23)taksin200200Încă nu există evaluări
- sjsdcmd7391 6494Document4 paginisjsdcmd7391 6494dcuhjdÎncă nu există evaluări
- Historia de Las Venopunciones Perifericas AMRivera ActaAnaesthBelg2005Document12 paginiHistoria de Las Venopunciones Perifericas AMRivera ActaAnaesthBelg2005Luis CruzÎncă nu există evaluări
- UNESCO's World Network of Biosphere Reserves: General QuestionsDocument21 paginiUNESCO's World Network of Biosphere Reserves: General QuestionsKurt ZepedaÎncă nu există evaluări
- Concentration ChangesDocument11 paginiConcentration ChangesKurt ZepedaÎncă nu există evaluări
- San PascualDocument1 paginăSan PascualKurt ZepedaÎncă nu există evaluări
- Albay Heritage Month Feature: St. Stephen The Protomartyr Church of LigaoDocument2 paginiAlbay Heritage Month Feature: St. Stephen The Protomartyr Church of LigaoKurt Zepeda100% (1)
- UNESCO's World Network of Biosphere Reserves: General QuestionsDocument21 paginiUNESCO's World Network of Biosphere Reserves: General QuestionsKurt ZepedaÎncă nu există evaluări
- SINGLE PAGE Issue No. 1 Volume No. 1 January December 2020Document40 paginiSINGLE PAGE Issue No. 1 Volume No. 1 January December 2020Kurt ZepedaÎncă nu există evaluări
- 2022 NCCA Call For Proposals - Competitive Grants ProgramDocument125 pagini2022 NCCA Call For Proposals - Competitive Grants ProgramKurt ZepedaÎncă nu există evaluări
- 'Natural' Traditions - Constructing Tropical Architecture in Transnational Malaysia and SingaporeDocument70 pagini'Natural' Traditions - Constructing Tropical Architecture in Transnational Malaysia and SingaporeKurt ZepedaÎncă nu există evaluări
- JacolbeDocument3 paginiJacolbeKurt ZepedaÎncă nu există evaluări
- NCCA Project Proposal FormDocument4 paginiNCCA Project Proposal FormKurt ZepedaÎncă nu există evaluări
- Scott PDFDocument19 paginiScott PDFWinzey Shane BaroniaÎncă nu există evaluări
- 2012 The Hittite Song of Going Forth CTHDocument62 pagini2012 The Hittite Song of Going Forth CTHKurt ZepedaÎncă nu există evaluări
- Structural Analysis of Three Selected FoDocument112 paginiStructural Analysis of Three Selected FoKurt ZepedaÎncă nu există evaluări
- Traditional Rice Farming Ritual Practices of The Magindanawn in Southern PhilippinesDocument4 paginiTraditional Rice Farming Ritual Practices of The Magindanawn in Southern PhilippinesKurt ZepedaÎncă nu există evaluări
- BalladsDocument4 paginiBalladsKurt ZepedaÎncă nu există evaluări
- Hinilawod EpicDocument3 paginiHinilawod EpicDianne Joy Arat-EnteraÎncă nu există evaluări
- TheGodsoftheCeltsandtheIndo EuropeansRevised2019Document517 paginiTheGodsoftheCeltsandtheIndo EuropeansRevised2019Kurt Zepeda100% (1)
- Neonatology I: Pediatrics 1.1Document15 paginiNeonatology I: Pediatrics 1.1Kurt ZepedaÎncă nu există evaluări
- Burial Systems of Ancient Mariana IslandersDocument2 paginiBurial Systems of Ancient Mariana IslandersKurt ZepedaÎncă nu există evaluări
- LeptoDocument16 paginiLeptoKurt ZepedaÎncă nu există evaluări
- Admission Conference: BRT TH Department of Surgery JULY 28, 2018Document3 paginiAdmission Conference: BRT TH Department of Surgery JULY 28, 2018Kurt ZepedaÎncă nu există evaluări
- Sociology of ReligionDocument61 paginiSociology of ReligionKurt ZepedaÎncă nu există evaluări
- JournalDocument3 paginiJournalKurt ZepedaÎncă nu există evaluări
- Quiz QuestionsDocument4 paginiQuiz QuestionsKurt Zepeda100% (1)
- Neolithic Landscapes of Ilocos NorteDocument13 paginiNeolithic Landscapes of Ilocos NorteKurt ZepedaÎncă nu există evaluări
- Neolithic Material Cultures of Oman and The Gulf Seashores From 5500-4500 BCE - S.mery, V.charpentier 2013Document13 paginiNeolithic Material Cultures of Oman and The Gulf Seashores From 5500-4500 BCE - S.mery, V.charpentier 2013ALACANAÎncă nu există evaluări
- Lima Action Plan For UNESCO's Man and The Biosphere (MAB) Programme and Its World Network of Biosphere Reserves (2016-2025)Document11 paginiLima Action Plan For UNESCO's Man and The Biosphere (MAB) Programme and Its World Network of Biosphere Reserves (2016-2025)Kurt ZepedaÎncă nu există evaluări
- Quiz QuestionsDocument4 paginiQuiz QuestionsKurt Zepeda100% (1)
- Quiz QuestionsDocument4 paginiQuiz QuestionsKurt Zepeda100% (1)
- GEN ED Contemporary WorldDocument166 paginiGEN ED Contemporary WorldTom Fernando100% (1)
- Family Relations - San Luis v. San Luis (CJ CARABBACAN)Document2 paginiFamily Relations - San Luis v. San Luis (CJ CARABBACAN)juna luz latigayÎncă nu există evaluări
- Lenovo Legion Y920-17IKB LCFC-DS321 NM-B311 R 0.2 SchematicDocument61 paginiLenovo Legion Y920-17IKB LCFC-DS321 NM-B311 R 0.2 SchematicYetawa GuaviareÎncă nu există evaluări
- Land Use Management (LUMDocument25 paginiLand Use Management (LUMgopumgÎncă nu există evaluări
- Key Area IIIDocument26 paginiKey Area IIIRobert M. MaluyaÎncă nu există evaluări
- KTQTE2Document172 paginiKTQTE2Ly Võ KhánhÎncă nu există evaluări
- A Comparative Study On Financial Performance of Private and PublicDocument17 paginiA Comparative Study On Financial Performance of Private and PublicaskmeeÎncă nu există evaluări
- Front Desk Staff-Giezel Bell Staff - Marc Client - Augustus Friend - AthenaDocument4 paginiFront Desk Staff-Giezel Bell Staff - Marc Client - Augustus Friend - Athenagener magbalitaÎncă nu există evaluări
- Pointers To Review For Long QuizDocument1 paginăPointers To Review For Long QuizJoice Ann PolinarÎncă nu există evaluări
- Office of The Divisional Forest Officer, Durgapur DivisionDocument30 paginiOffice of The Divisional Forest Officer, Durgapur Divisionrchowdhury_10Încă nu există evaluări
- Blockchain in ConstructionDocument4 paginiBlockchain in ConstructionHasibullah AhmadzaiÎncă nu există evaluări
- Riph - Prelim ReviewerDocument12 paginiRiph - Prelim ReviewerNikoru100% (3)
- A List of The Public NTP ServersDocument11 paginiA List of The Public NTP ServersavinashjirapureÎncă nu există evaluări
- Botany DownsDocument5 paginiBotany DownsMayank PurwarÎncă nu există evaluări
- Andres Felipe Mendez Vargas: The Elves and The ShoemakerDocument1 paginăAndres Felipe Mendez Vargas: The Elves and The ShoemakerAndres MendezÎncă nu există evaluări
- BHMCT 5TH Semester Industrial TrainingDocument30 paginiBHMCT 5TH Semester Industrial Trainingmahesh kumarÎncă nu există evaluări
- Digest-China Banking Corp. v. CIRDocument9 paginiDigest-China Banking Corp. v. CIRjackyÎncă nu există evaluări
- Historical Perspective of Financial Reporting Regulations in MalaysiaDocument2 paginiHistorical Perspective of Financial Reporting Regulations in Malaysiauglore100% (6)
- India International SchoolDocument15 paginiIndia International Schoolazimmuhammed673790Încă nu există evaluări
- Ilm-e-Hadees Sikhne Wale Ke Liye Kuch AadaabDocument5 paginiIlm-e-Hadees Sikhne Wale Ke Liye Kuch AadaabSalman KhanÎncă nu există evaluări
- 07 DecisionTreeTasksWeek8Document5 pagini07 DecisionTreeTasksWeek8Nebojša ĐukićÎncă nu există evaluări
- Devel Goth ArchDocument512 paginiDevel Goth ArchAmiee Groundwater100% (2)
- As SaaffatDocument39 paginiAs SaaffatAyesha KhanÎncă nu există evaluări
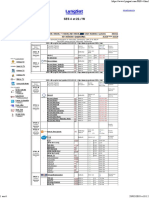
- SES 4 at 22. °W: Advertisements AdvertisementsDocument6 paginiSES 4 at 22. °W: Advertisements Advertisementsemmanuel danra10Încă nu există evaluări
- Bangalore CityDocument2 paginiBangalore CityRoomaÎncă nu există evaluări
- Practical TaskDocument3 paginiPractical TaskAAAAAAAÎncă nu există evaluări
- Order Confirmation 318155149Document3 paginiOrder Confirmation 318155149charisse mae rillortaÎncă nu există evaluări
- Introduction To Marketing - KotlerDocument35 paginiIntroduction To Marketing - KotlerRajesh Patro0% (1)
- Political Law vs. Constitutional LawDocument3 paginiPolitical Law vs. Constitutional LawJamilah DagandanÎncă nu există evaluări
- An Unfinished Love Story: A Personal History of the 1960sDe la EverandAn Unfinished Love Story: A Personal History of the 1960sEvaluare: 5 din 5 stele5/5 (3)
- Roxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueDe la EverandRoxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueEvaluare: 4.5 din 5 stele4.5/5 (26)
- Son of Hamas: A Gripping Account of Terror, Betrayal, Political Intrigue, and Unthinkable ChoicesDe la EverandSon of Hamas: A Gripping Account of Terror, Betrayal, Political Intrigue, and Unthinkable ChoicesEvaluare: 4.5 din 5 stele4.5/5 (499)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (29)
- Roxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueDe la EverandRoxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueEvaluare: 5 din 5 stele5/5 (3)
- Briefly Perfectly Human: Making an Authentic Life by Getting Real About the EndDe la EverandBriefly Perfectly Human: Making an Authentic Life by Getting Real About the EndÎncă nu există evaluări
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Broken: The most shocking childhood story ever told. An inspirational author who survived it.De la EverandBroken: The most shocking childhood story ever told. An inspirational author who survived it.Evaluare: 5 din 5 stele5/5 (45)
- Liar's Poker: Rising Through the Wreckage on Wall StreetDe la EverandLiar's Poker: Rising Through the Wreckage on Wall StreetEvaluare: 4 din 5 stele4/5 (1088)
- Autobiography of a Yogi (Unabridged)De la EverandAutobiography of a Yogi (Unabridged)Evaluare: 5 din 5 stele5/5 (122)
- Becky Lynch: The Man: Not Your Average Average GirlDe la EverandBecky Lynch: The Man: Not Your Average Average GirlEvaluare: 4.5 din 5 stele4.5/5 (15)
- The Rulebreaker: The Life and Times of Barbara WaltersDe la EverandThe Rulebreaker: The Life and Times of Barbara WaltersEvaluare: 4.5 din 5 stele4.5/5 (3)
- Stoicism The Art of Happiness: How the Stoic Philosophy Works, Living a Good Life, Finding Calm and Managing Your Emotions in a Turbulent World. New VersionDe la EverandStoicism The Art of Happiness: How the Stoic Philosophy Works, Living a Good Life, Finding Calm and Managing Your Emotions in a Turbulent World. New VersionEvaluare: 5 din 5 stele5/5 (51)