S-ar putea să vă placă și
- (Playbook Bible For Couples) Wagner, Alison - Sex Positions - Sex Tips & Techniques For 21 Steamy Sexual Positions (2017)Document48 pagini(Playbook Bible For Couples) Wagner, Alison - Sex Positions - Sex Tips & Techniques For 21 Steamy Sexual Positions (2017)Hariharan Ravichandran100% (1)
- Sex God Method ShortDocument15 paginiSex God Method ShortAti100% (2)
- Sexuality in Older AdultDocument10 paginiSexuality in Older AdultNisa100% (1)
- Female Sexual: Assessing & ManagingDocument8 paginiFemale Sexual: Assessing & ManagingJazmin GarcèsÎncă nu există evaluări
- College Avenue Magazine: Volume 5 Issue 2Document52 paginiCollege Avenue Magazine: Volume 5 Issue 2collegeavenue13% (8)
- Jerk To Gay Porn MoviesDocument4 paginiJerk To Gay Porn Movieslinnwotring0% (4)
- Questionaire CheckboxDocument22 paginiQuestionaire CheckboxRobÎncă nu există evaluări
- W9 Nelson Getting Dirty Rotated Ocr CombinedDocument17 paginiW9 Nelson Getting Dirty Rotated Ocr CombinedCaitlyn Cat Crandell100% (1)
- Gender Stereotypes in She's The Man and Twelfth Night.Document2 paginiGender Stereotypes in She's The Man and Twelfth Night.sushiushiÎncă nu există evaluări
- Female Sexual Function, Dysfunction, and PregnancyDocument9 paginiFemale Sexual Function, Dysfunction, and PregnancyDiana Sofia Castillo CabreraÎncă nu există evaluări
- What Is LGBTQ PaperDocument15 paginiWhat Is LGBTQ Paperapi-338540472Încă nu există evaluări
- 561117sacasc87 365 Sex PositionsDocument388 pagini561117sacasc87 365 Sex PositionsAlexandr TrotskyÎncă nu există evaluări
- Enteral NutritionDocument73 paginiEnteral NutritionYosep SutandarÎncă nu există evaluări
- Mystery Method - The Easiest Way To Pick-UpDocument3 paginiMystery Method - The Easiest Way To Pick-UpMike LyonsÎncă nu există evaluări
- Essay Same Sex MarriageDocument1 paginăEssay Same Sex MarriageErbert Medellin89% (18)
- The Quality of Life of Women SufferDocument8 paginiThe Quality of Life of Women SufferKritika AgarwalÎncă nu există evaluări
- Human Sexuality During Pregnancy and The Postpartum Period: ReviewDocument5 paginiHuman Sexuality During Pregnancy and The Postpartum Period: ReviewIoan-ovidiu CordisÎncă nu există evaluări
- Sexual Dysfunction 3Document23 paginiSexual Dysfunction 3Wael GaberÎncă nu există evaluări
- Sexual Dysfunction After Delivery: Faculty of Medicine, Menoufia UniversityDocument22 paginiSexual Dysfunction After Delivery: Faculty of Medicine, Menoufia UniversityWael GaberÎncă nu există evaluări
- Sexual DysfunctionDocument21 paginiSexual DysfunctionWael GaberÎncă nu există evaluări
- Sexuality During PregnancyDocument7 paginiSexuality During PregnancykakaÎncă nu există evaluări
- 06 Chapter 2Document48 pagini06 Chapter 2Prakash BalagurunathanÎncă nu există evaluări
- Infertility and Sexual Dysfunctions: A Systematic Literature ReviewDocument8 paginiInfertility and Sexual Dysfunctions: A Systematic Literature ReviewTantonio Tri PutraÎncă nu există evaluări
- Factors Associated With Menstrual Cycle Irregularity and MenopauseDocument11 paginiFactors Associated With Menstrual Cycle Irregularity and MenopauseRyan IlhamÎncă nu există evaluări
- 1 Monteiro Etal 2021Document6 pagini1 Monteiro Etal 2021Gabriel GursenÎncă nu există evaluări
- Sexual - Life - and - Dysfunction - After - Maternal - Morbidi BGFNBRNDocument14 paginiSexual - Life - and - Dysfunction - After - Maternal - Morbidi BGFNBRNOctaria SaputraÎncă nu există evaluări
- NIH Public Access: Author ManuscriptDocument18 paginiNIH Public Access: Author ManuscriptAnca RaduÎncă nu există evaluări
- The Relationship Between Mode of Delivery and Sexual Health Outcomes After ChildbirthDocument10 paginiThe Relationship Between Mode of Delivery and Sexual Health Outcomes After Childbirthsipen poltekkesbdgÎncă nu există evaluări
- 7117 12364 1 PB PDFDocument5 pagini7117 12364 1 PB PDFNadya MagfiraÎncă nu există evaluări
- Endo Met RitisDocument9 paginiEndo Met RitisabdullahÎncă nu există evaluări
- Percepções de Mulheres Obesas Sobre A SexualidadeDocument5 paginiPercepções de Mulheres Obesas Sobre A SexualidadejoaomartinelliÎncă nu există evaluări
- Author Information Kafaei Atrian MDocument9 paginiAuthor Information Kafaei Atrian MabdullahÎncă nu există evaluări
- Endo Met RitisDocument9 paginiEndo Met RitisabdullahÎncă nu există evaluări
- JRJRJRJDocument7 paginiJRJRJRJlionfairwayÎncă nu există evaluări
- Postpartum Sexual Functioning and Its Predicting Factors Among Iranian WomenDocument10 paginiPostpartum Sexual Functioning and Its Predicting Factors Among Iranian WomenTahir AzizÎncă nu există evaluări
- Female SDysDocument6 paginiFemale SDysDheby PasoroÎncă nu există evaluări
- Peripartum Expectations, Mode of Delivery, and Perineal Injury On Women's Postpartum SexualityDocument14 paginiPeripartum Expectations, Mode of Delivery, and Perineal Injury On Women's Postpartum SexualityAhlem MtiraouiÎncă nu există evaluări
- Development of A Health-Related Quality-of-Life Questionnaire (PCOSQ) For Women With Polycystic Ovary Syndrome (PCOS)Document12 paginiDevelopment of A Health-Related Quality-of-Life Questionnaire (PCOSQ) For Women With Polycystic Ovary Syndrome (PCOS)Ke XuÎncă nu există evaluări
- PcosDocument5 paginiPcosAinul AzlindaÎncă nu există evaluări
- NIH Public Access: Author ManuscriptDocument14 paginiNIH Public Access: Author ManuscriptNurulDiniaPutriÎncă nu există evaluări
- BJOG - 2005 - Bartellas - Sexuality and Sexual Activity in PregnancyDocument5 paginiBJOG - 2005 - Bartellas - Sexuality and Sexual Activity in Pregnancyศุภชัย ศิลาวัชรพลÎncă nu există evaluări
- Jurnal Disfungsi Sex 1Document16 paginiJurnal Disfungsi Sex 1REGZahra Seleisyah TianmeÎncă nu există evaluări
- Lag Aert 2017Document8 paginiLag Aert 2017abdi syahputraÎncă nu există evaluări
- QOL of Women During PregnancyDocument5 paginiQOL of Women During PregnancyTehreem IrshadÎncă nu există evaluări
- Toksemia GravidarumDocument9 paginiToksemia GravidarumabdullahÎncă nu există evaluări
- 2019 PALACIOS Et Al - Effect of A Multi-Ingredient Based Food Supplement On Sexual Function in Women With Low Sexual DesireDocument7 pagini2019 PALACIOS Et Al - Effect of A Multi-Ingredient Based Food Supplement On Sexual Function in Women With Low Sexual DesireRenanÎncă nu există evaluări
- Our Data Showed That Sexual Disorders Were Highly PrevalentDocument5 paginiOur Data Showed That Sexual Disorders Were Highly Prevalentsheirly100% (1)
- Nejmoa 067423Document13 paginiNejmoa 067423ArghaÎncă nu există evaluări
- Impact of Menopause On Quality of Life Among Indian WomenDocument16 paginiImpact of Menopause On Quality of Life Among Indian WomenGlobal Research and Development ServicesÎncă nu există evaluări
- Author Information Kafaei Atrian MDocument9 paginiAuthor Information Kafaei Atrian MabdullahÎncă nu există evaluări
- Author Information Kafaei Atrian MDocument9 paginiAuthor Information Kafaei Atrian MabdullahÎncă nu există evaluări
- Sexual Dysfunction Among Women With Diabetes in A Primary Health Care at Semarang, Central Java Province, IndonesiaDocument8 paginiSexual Dysfunction Among Women With Diabetes in A Primary Health Care at Semarang, Central Java Province, IndonesiaTantonio Tri PutraÎncă nu există evaluări
- Pelvic Floor Healing Milestones After Obstetric Anal Sphincter Injury: A Prospective Case Control Feasibility StudyDocument9 paginiPelvic Floor Healing Milestones After Obstetric Anal Sphincter Injury: A Prospective Case Control Feasibility Studywijana410Încă nu există evaluări
- Coitus Late in PregnancyDocument8 paginiCoitus Late in PregnancyabdullahÎncă nu există evaluări
- (PCOSQ) ImpDocument12 pagini(PCOSQ) Impamanysalama5976Încă nu există evaluări
- Aerts Et Al 2014Document8 paginiAerts Et Al 2014chatsashÎncă nu există evaluări
- Ekwo 1993Document10 paginiEkwo 1993Nurul ImaniarÎncă nu există evaluări
- Fink, Carson & DeVellis - Adult Circumcision Outcomes Study PDFDocument4 paginiFink, Carson & DeVellis - Adult Circumcision Outcomes Study PDFOmar MohammedÎncă nu există evaluări
- The Effect of Total Hysterectomy On Sexual Function and DepressionDocument6 paginiThe Effect of Total Hysterectomy On Sexual Function and DepressionJA BerzabalÎncă nu există evaluări
- Mode of Delivery On Sexual FunctionDocument9 paginiMode of Delivery On Sexual Functionoluchukwuobina92Încă nu există evaluări
- Vaginal Health in Menopausal Peruvian WomenDocument6 paginiVaginal Health in Menopausal Peruvian WomenManuel WongÎncă nu există evaluări
- Adverse Childhood Experiences and Repeat Induced Abortion: General GynecologyDocument6 paginiAdverse Childhood Experiences and Repeat Induced Abortion: General Gynecologychie_8866Încă nu există evaluări
- Genital Pain and Sexual Functioning: Effects On Sexual Experience, Psychological Health, and Quality of LifeDocument13 paginiGenital Pain and Sexual Functioning: Effects On Sexual Experience, Psychological Health, and Quality of LifeSexologia Del OesteÎncă nu există evaluări
- The Sexual Activity QuestionnaireDocument10 paginiThe Sexual Activity Questionnaireศุภชัย ศิลาวัชรพลÎncă nu există evaluări
- 05 N017 13590Document15 pagini05 N017 13590Rajmohan VijayanÎncă nu există evaluări
- Climacteric-Related Symptoms in Menopause Transition and Beyond: A Prospective 19-Year Follow-Up Study On Previously Hysterectomized WomenDocument7 paginiClimacteric-Related Symptoms in Menopause Transition and Beyond: A Prospective 19-Year Follow-Up Study On Previously Hysterectomized WomenRicardo MedinaÎncă nu există evaluări
- NIH Public Access: Author ManuscriptDocument19 paginiNIH Public Access: Author ManuscriptErna Jovem GluberryÎncă nu există evaluări
- Sex and AgingDocument3 paginiSex and AgingCristhian RamírezÎncă nu există evaluări
- Factors in Uencing Couples' Sexuality in The Puerperium: A Systematic ReviewDocument10 paginiFactors in Uencing Couples' Sexuality in The Puerperium: A Systematic ReviewIonela BogdanÎncă nu există evaluări
- Perception ChildbearingDocument18 paginiPerception ChildbearingnorjumawatonshahruddÎncă nu există evaluări
- Maternal Nursing Care - CHPT 6 Human Sexuality and FertilityDocument28 paginiMaternal Nursing Care - CHPT 6 Human Sexuality and Fertilitythubtendrolma100% (1)
- The Secrets You Should Know About Sexual Medicine; Part One; Obesity and Sexual DysfunctionDe la EverandThe Secrets You Should Know About Sexual Medicine; Part One; Obesity and Sexual DysfunctionÎncă nu există evaluări
- Routine Firsttrimester Ultrasound Screening Using A Standardized Anatomical ProtocolDocument15 paginiRoutine Firsttrimester Ultrasound Screening Using A Standardized Anatomical ProtocolYosep SutandarÎncă nu există evaluări
- PIIS000293781502102XDocument1 paginăPIIS000293781502102XYosep SutandarÎncă nu există evaluări
- Physiology of Amniotic Fluid Volume RegulationDocument8 paginiPhysiology of Amniotic Fluid Volume RegulationYosep SutandarÎncă nu există evaluări
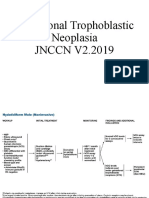
- Gestational Trophoblastic NeoplasiaDocument14 paginiGestational Trophoblastic NeoplasiaYosep SutandarÎncă nu există evaluări
- Ferra RettiDocument51 paginiFerra RettiYosep SutandarÎncă nu există evaluări
- Acog Committee Opinion: Dysmenorrhea and Endometriosis in The AdolescentDocument10 paginiAcog Committee Opinion: Dysmenorrhea and Endometriosis in The AdolescentYosep SutandarÎncă nu există evaluări
- Mao2014 Article ImagingOfPelvicLymphNodesDocument13 paginiMao2014 Article ImagingOfPelvicLymphNodesYosep SutandarÎncă nu există evaluări
- Practice Bullet In: Emergency ContraceptionDocument11 paginiPractice Bullet In: Emergency ContraceptionYosep SutandarÎncă nu există evaluări
- Ovarian Reserve Testing: A User's Guide: Expert ReviewsDocument12 paginiOvarian Reserve Testing: A User's Guide: Expert ReviewsYosep SutandarÎncă nu există evaluări
- Eng - PDF JsessionidDocument34 paginiEng - PDF JsessionidYosep SutandarÎncă nu există evaluări
- Pi Is 0884217517304100Document3 paginiPi Is 0884217517304100Yosep SutandarÎncă nu există evaluări
- Clue CellsDocument10 paginiClue CellsYosep SutandarÎncă nu există evaluări
- STD Prevention Question SheetDocument1 paginăSTD Prevention Question Sheetapi-282682274Încă nu există evaluări
- Bpo Application Form: Republic of The Philippines Province of Pangasinan Municipality of Bautista Barangay SinabaanDocument1 paginăBpo Application Form: Republic of The Philippines Province of Pangasinan Municipality of Bautista Barangay SinabaanOmar Dizon II50% (2)
- Lesson 17Document26 paginiLesson 17LANIE JANE BRUCALÎncă nu există evaluări
- Assignment: Beltei Internationa UniversityDocument13 paginiAssignment: Beltei Internationa UniversityEN ChomrongÎncă nu există evaluări
- Reworking The Term SlutDocument14 paginiReworking The Term Slutapi-237706595Încă nu există evaluări
- Ss1 Family Planning EssayDocument1 paginăSs1 Family Planning EssayIrish BarcelonÎncă nu există evaluări
- 1 Applications: Matching/mating Yusen SungDocument4 pagini1 Applications: Matching/mating Yusen Sung1030966ckjanananwnnÎncă nu există evaluări
- Change in Cultural Perception Related To Sex in IndiaDocument20 paginiChange in Cultural Perception Related To Sex in IndiaprachiÎncă nu există evaluări
- Working Towards A More Progressive and IDocument11 paginiWorking Towards A More Progressive and INicole Andrei RiveraÎncă nu există evaluări
- 8 Sexuality As An Important Component of One's PersonalityDocument14 pagini8 Sexuality As An Important Component of One's PersonalityJeneva Rose PerezÎncă nu există evaluări
- Teen Talk Vol 3Document2 paginiTeen Talk Vol 3api-309082881Încă nu există evaluări
- MateriDocument10 paginiMateriDevi Claudia PalupiÎncă nu există evaluări
- Childhood Sexual Abuse, Relationship Satisfaction, and Sexual Risk Taking in A Community Sample of WomenDocument9 paginiChildhood Sexual Abuse, Relationship Satisfaction, and Sexual Risk Taking in A Community Sample of WomenScott PymÎncă nu există evaluări
- The Sexual SelfDocument83 paginiThe Sexual Self-------Încă nu există evaluări
- Contraceptive Use and Unplanned Pregnancy Among Female Sex Workers in ZambiaDocument7 paginiContraceptive Use and Unplanned Pregnancy Among Female Sex Workers in ZambiaNiki Rizqi rachmawatiÎncă nu există evaluări
- Sex Education and Adolescent Sexual Risk-Taking Behavior: A Correlational StudyDocument10 paginiSex Education and Adolescent Sexual Risk-Taking Behavior: A Correlational StudyMelvin TamayoÎncă nu există evaluări
- Why Pornography Should Be Available For All AgesDocument3 paginiWhy Pornography Should Be Available For All Agesdarker_polar2Încă nu există evaluări
- Division of Eastern Samar: Giporlos National Trade SchoolDocument5 paginiDivision of Eastern Samar: Giporlos National Trade Schooljhun ecleoÎncă nu există evaluări
- Gender 4Document9 paginiGender 4api-438533699Încă nu există evaluări