S-ar putea să vă placă și
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- MEDICAL TERMINOLOGY PRAKTIKUM.2020docxDocument17 paginiMEDICAL TERMINOLOGY PRAKTIKUM.2020docxmawarÎncă nu există evaluări
- Health and Medical Certificate 3Document1 paginăHealth and Medical Certificate 3Danilo P. PancitoÎncă nu există evaluări
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionDe la EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionÎncă nu există evaluări
- Pre-Employment Medical FormDocument2 paginiPre-Employment Medical FormSourin NandiÎncă nu există evaluări
- Step 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionDe la EverandStep 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionÎncă nu există evaluări
- Test Bank For Equipment Theory For Respiratory Care 5th Edition by WhiteDocument11 paginiTest Bank For Equipment Theory For Respiratory Care 5th Edition by Whiteharoldbrownorcnxeijgd100% (29)
- Post Test AtlsDocument6 paginiPost Test Atlsnurul huda85% (62)
- Hearing ImpairmentDocument20 paginiHearing ImpairmentAlexandra Villaflor HernandezÎncă nu există evaluări
- D F-Elevated Blood Pressure DDocument2 paginiD F-Elevated Blood Pressure DMenly SusadaÎncă nu există evaluări
- Medical Form For Grade 7 12Document3 paginiMedical Form For Grade 7 12Deonna Angeline100% (1)
- Asessment and Evaluation FormsDocument11 paginiAsessment and Evaluation FormsJU DYÎncă nu există evaluări
- Newborn Physical AssessmentDocument7 paginiNewborn Physical AssessmentBinal JoshiÎncă nu există evaluări
- Amc Recall 2Document18 paginiAmc Recall 2vivekmoÎncă nu există evaluări
- FormDocument2 paginiFormBhargav VekariaÎncă nu există evaluări
- Medical Examination FormDocument3 paginiMedical Examination Formchumbefred20% (5)
- 7th Semester Log BookDocument57 pagini7th Semester Log BookaskmovieflixÎncă nu există evaluări
- Medical Form For All ApplicantsDocument2 paginiMedical Form For All ApplicantsHaason TzÎncă nu există evaluări
- P.A. Tool (Case Pres FINAL.)Document23 paginiP.A. Tool (Case Pres FINAL.)Crystal Ann TadiamonÎncă nu există evaluări
- Nursing Administration AssessmentDocument6 paginiNursing Administration Assessmentkatnebrija89Încă nu există evaluări
- PCS - Physician's Clinical Statement Form 2019 EtiqaDocument2 paginiPCS - Physician's Clinical Statement Form 2019 EtiqaRowena CallosÎncă nu există evaluări
- Anamnesis Form: Name Dose Regularity How Long Have You Been Taking ItDocument3 paginiAnamnesis Form: Name Dose Regularity How Long Have You Been Taking ItĐeŋýzař Đ ZòįđýckÎncă nu există evaluări
- 9 Thorax LungsDocument2 pagini9 Thorax LungsmendozakaceeyÎncă nu există evaluări
- Physical Therapy Evaluation FormDocument6 paginiPhysical Therapy Evaluation FormRobin MathewÎncă nu există evaluări
- OB Patho Assessment Tool EditedDocument6 paginiOB Patho Assessment Tool EditedDarren RobertoÎncă nu există evaluări
- Date: - : (Last) (First) (Middle)Document5 paginiDate: - : (Last) (First) (Middle)KatieÎncă nu există evaluări
- Prenatal Check Up InterviewDocument7 paginiPrenatal Check Up InterviewSHIELOU LOMODÎncă nu există evaluări
- Obstetric CRQsDocument4 paginiObstetric CRQsKomella PrakasamÎncă nu există evaluări
- Cardiovascular Module2Document27 paginiCardiovascular Module2Gracia MayaÎncă nu există evaluări
- NCP MaternalDocument21 paginiNCP MaternalDorothee GumisadÎncă nu există evaluări
- Assigned CasesDocument8 paginiAssigned CasessadiaÎncă nu există evaluări
- Physical Exam FormDocument1 paginăPhysical Exam FormEthan AtchleyÎncă nu există evaluări
- Borang Silat DoktorDocument2 paginiBorang Silat DoktorhafizÎncă nu există evaluări
- SDL3Document2 paginiSDL3Margaux BaynosaÎncă nu există evaluări
- Medical InformationDocument1 paginăMedical InformationfaithchurchyouthÎncă nu există evaluări
- SDL3 Self Directed LearningDocument2 paginiSDL3 Self Directed LearningKaila Marie BillonesÎncă nu există evaluări
- Sedation Record: Patient Selection Criteria DateDocument2 paginiSedation Record: Patient Selection Criteria Datenona aryanÎncă nu există evaluări
- Medical Form 2020 - 0Document3 paginiMedical Form 2020 - 0Light King ChaudharyÎncă nu există evaluări
- Pediatrics Workbook 2020Document11 paginiPediatrics Workbook 202019212024 AzizahÎncă nu există evaluări
- Cuidados Posoperatorio CirugiaDocument1 paginăCuidados Posoperatorio CirugiaAna CristernaÎncă nu există evaluări
- Medical Incident ReportDocument5 paginiMedical Incident Reportpetersen772339Încă nu există evaluări
- Procedural Sedation RecordDocument2 paginiProcedural Sedation RecordRosanne AguilarÎncă nu există evaluări
- Peace Corps Asthma Evaluation Form PC-262-2 (Initial Approval 08/2012)Document4 paginiPeace Corps Asthma Evaluation Form PC-262-2 (Initial Approval 08/2012)Accessible Journal Media: Peace Corps DocumentsÎncă nu există evaluări
- Health Form OaDocument1 paginăHealth Form OaWarren Castonguay JrÎncă nu există evaluări
- TB Chemoprophylaxis Monitor Modified 1Document2 paginiTB Chemoprophylaxis Monitor Modified 1Ferry DimyatiÎncă nu există evaluări
- Birla Institute of Technology & Science, Pilani (Rajasthan)Document1 paginăBirla Institute of Technology & Science, Pilani (Rajasthan)saminafirojÎncă nu există evaluări
- NHH TemplateDocument6 paginiNHH TemplateCaryl EteÎncă nu există evaluări
- Initial and Annual Health RecordDocument2 paginiInitial and Annual Health Recordmariegold mortola fabelaÎncă nu există evaluări
- Health History Assessment ToolDocument3 paginiHealth History Assessment ToolDaniela Suarez NimÎncă nu există evaluări
- Medical CertDocument1 paginăMedical CertLily SC ReyesÎncă nu există evaluări
- CLTCMEDICALCERtificationDocument1 paginăCLTCMEDICALCERtificationLily SC ReyesÎncă nu există evaluări
- Fitness Aziz AlhaidariDocument2 paginiFitness Aziz Alhaidariabdulaziz saif ali mansoorÎncă nu există evaluări
- Personal Medical History: Doctor Visit ChecklistDocument11 paginiPersonal Medical History: Doctor Visit ChecklistValentina VillarrealÎncă nu există evaluări
- Application Form Health Examination Form Parents Consent Form Camper'SDocument1 paginăApplication Form Health Examination Form Parents Consent Form Camper'SJeff BalladÎncă nu există evaluări
- Nursing Seminar 1 SAS Session 2Document9 paginiNursing Seminar 1 SAS Session 2ZiaÎncă nu există evaluări
- (HSO) Medical Examination FormDocument1 pagină(HSO) Medical Examination FormKrizel LagundiÎncă nu există evaluări
- ANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientDocument5 paginiANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientjackydoodsonÎncă nu există evaluări
- 8 AbdomenDocument3 pagini8 AbdomenSophia MarieÎncă nu există evaluări
- Gordon S Functional Health Pattern Assessment ToolDocument10 paginiGordon S Functional Health Pattern Assessment ToolMiguel VicenteÎncă nu există evaluări
- WM 03092011Document15 paginiWM 03092011Sbc GradÎncă nu există evaluări
- Gordon's FormDocument6 paginiGordon's FormHarry AglugobÎncă nu există evaluări
- Please SpecifyDocument1 paginăPlease SpecifyleonÎncă nu există evaluări
- Headaches Residual Functional Capacity QuestionnaireDocument3 paginiHeadaches Residual Functional Capacity QuestionnaireDellComputer99Încă nu există evaluări
- Enrolment FormDocument2 paginiEnrolment FormHiy GisingÎncă nu există evaluări
- Chnursing NotesDocument21 paginiChnursing Notesjimmy boy canlas jrÎncă nu există evaluări
- Application Form Health Examination Form Parents Consent FormDocument1 paginăApplication Form Health Examination Form Parents Consent Formapril rose catainaÎncă nu există evaluări
- YukonDocument28 paginiYukonBhargav VekariaÎncă nu există evaluări
- Line Plan XcracerDocument1 paginăLine Plan XcracerBhargav VekariaÎncă nu există evaluări
- OfferTermsCondition2019 11 25 - 063147592 PDFDocument1 paginăOfferTermsCondition2019 11 25 - 063147592 PDFBhargav VekariaÎncă nu există evaluări
- Post Office Monthly Income Scheme (POMIS) - Calculator: Interest Rate 7.70% Amount Invested (RS.) 100,000Document3 paginiPost Office Monthly Income Scheme (POMIS) - Calculator: Interest Rate 7.70% Amount Invested (RS.) 100,000Bhargav VekariaÎncă nu există evaluări
- Post Office Monthly Income Scheme (POMIS) - Calculator: Interest Rate 7.70% Amount Invested (RS.) 100,000Document3 paginiPost Office Monthly Income Scheme (POMIS) - Calculator: Interest Rate 7.70% Amount Invested (RS.) 100,000Bhargav VekariaÎncă nu există evaluări
- Measurement Report: Report Number: Sample Name: Manufacturer: S/NDocument1 paginăMeasurement Report: Report Number: Sample Name: Manufacturer: S/NtermicasÎncă nu există evaluări
- YukonDocument28 paginiYukonBhargav VekariaÎncă nu există evaluări
- Candidateapplicationform PDFDocument2 paginiCandidateapplicationform PDFBhargav VekariaÎncă nu există evaluări
- District-Wise Covid-19 Cases in India - April 6Document8 paginiDistrict-Wise Covid-19 Cases in India - April 6Express WebÎncă nu există evaluări
- Nehru Institute of Mountaineering Uttarkashi, Uttarakhand (India) - 249193Document2 paginiNehru Institute of Mountaineering Uttarkashi, Uttarakhand (India) - 249193Bhargav VekariaÎncă nu există evaluări
- National Rock Climbing Camp National Rock Climbing CampDocument2 paginiNational Rock Climbing Camp National Rock Climbing CampBhargav VekariaÎncă nu există evaluări
- Kessler 2-3may17 Workshop SSDocument31 paginiKessler 2-3may17 Workshop SSBhargav VekariaÎncă nu există evaluări
- Gautam BuddhaDocument64 paginiGautam BuddhasharathVEMÎncă nu există evaluări
- DownloadDocument138 paginiDownloaddehammoÎncă nu există evaluări
- CoronaDocument7 paginiCoronaSaurabh ShandilyaÎncă nu există evaluări
- Book Indian Birds TextDocument444 paginiBook Indian Birds TextMani KandanÎncă nu există evaluări
- Course Schedule For Year 2017-2018: Swami Vivekanand Institute of MountaineeringDocument2 paginiCourse Schedule For Year 2017-2018: Swami Vivekanand Institute of MountaineeringBhargav VekariaÎncă nu există evaluări
- Course Prog 2017-18Document5 paginiCourse Prog 2017-18Bhargav VekariaÎncă nu există evaluări
- Your Role As A Frontline Worker Is Two-Fold:: What Is COVID-19? How Does COVID-19 Spread?Document4 paginiYour Role As A Frontline Worker Is Two-Fold:: What Is COVID-19? How Does COVID-19 Spread?Debapriya SamalÎncă nu există evaluări
- JIO Exchange Make-ModelsDocument709 paginiJIO Exchange Make-ModelsChandan Kumar Satyanarayana0% (1)
- Sociology of Sport: Pamela SerraDocument39 paginiSociology of Sport: Pamela SerraBhargav VekariaÎncă nu există evaluări
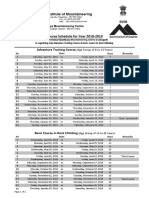
- Course Schedule For Year 2018-2019: Swami Vivekanand Institute of MountaineeringDocument2 paginiCourse Schedule For Year 2018-2019: Swami Vivekanand Institute of MountaineeringBhargav VekariaÎncă nu există evaluări
- Communication in Difficult Times - Final PDFDocument21 paginiCommunication in Difficult Times - Final PDFBhargav VekariaÎncă nu există evaluări
- SHIVALIKLAKEVIEW-II PriceList 2922020161712948 PDFDocument2 paginiSHIVALIKLAKEVIEW-II PriceList 2922020161712948 PDFBhargav VekariaÎncă nu există evaluări
- Amc Ssi PDFDocument308 paginiAmc Ssi PDFRinoy R BhagoraÎncă nu există evaluări
- Communication in Difficult Times - Final PDFDocument21 paginiCommunication in Difficult Times - Final PDFBhargav VekariaÎncă nu există evaluări
- Nihms 897616Document7 paginiNihms 897616Hafidz Ma'rufÎncă nu există evaluări
- Swiggy Order 43333379786Document2 paginiSwiggy Order 43333379786Bhargav VekariaÎncă nu există evaluări
- Biography of Alexander FlemingDocument3 paginiBiography of Alexander FlemingElizabeth Ramos SayritupacÎncă nu există evaluări
- QSE6034: Teknologi Dan Inovasi Dalam Sains SukanDocument3 paginiQSE6034: Teknologi Dan Inovasi Dalam Sains SukanMohamad Ramlan RamliÎncă nu există evaluări
- Fraser Health: Health Authority Redesign AccomplishmentsDocument13 paginiFraser Health: Health Authority Redesign AccomplishmentsStephen OlsonÎncă nu există evaluări
- Avortul Medicamentos Si ChirurgicalDocument72 paginiAvortul Medicamentos Si ChirurgicalNicu EnachiÎncă nu există evaluări
- Barium StudiesDocument89 paginiBarium StudiesManuel PoncianÎncă nu există evaluări
- FIGURE: Haemobartonella Felis in Blood From A Cat. Organisms Appear As Small Cocci, Rods, orDocument3 paginiFIGURE: Haemobartonella Felis in Blood From A Cat. Organisms Appear As Small Cocci, Rods, orabdulÎncă nu există evaluări
- Blood: Elaine N. MariebDocument42 paginiBlood: Elaine N. Mariebkhim catubayÎncă nu există evaluări
- For Demo in Teaching Strategies by Mike ReyesDocument10 paginiFor Demo in Teaching Strategies by Mike ReyesPaulo Sandino GaliciaÎncă nu există evaluări
- ISR NG Chun Ruh2Document1 paginăISR NG Chun Ruh2Yasmine SlhÎncă nu există evaluări
- PBLDocument6 paginiPBLzuhaldarwisÎncă nu există evaluări
- Acyclovir - Iarc Monographs 76-6Document25 paginiAcyclovir - Iarc Monographs 76-6NitinPrachiJainÎncă nu există evaluări
- Tara's Intro To Critical CareDocument6 paginiTara's Intro To Critical CareTara McNeillÎncă nu există evaluări
- Surgical Complication of Typhoid FeverDocument10 paginiSurgical Complication of Typhoid FeverHelsa Eldatarina JÎncă nu există evaluări
- JAT - CHT 13Document68 paginiJAT - CHT 13j_smith24Încă nu există evaluări
- In An Incisional Model of Wound Healing Genistein Aglycone Enhances Skin Recovery A Comparison With Raloxifene and Estradiol in Ovariectomized Rats Is PresentedDocument10 paginiIn An Incisional Model of Wound Healing Genistein Aglycone Enhances Skin Recovery A Comparison With Raloxifene and Estradiol in Ovariectomized Rats Is PresentedAthenaeum Scientific PublishersÎncă nu există evaluări
- Propofol 1 2 BrochureDocument4 paginiPropofol 1 2 BrochureDr. Hafiz Shahid HameedÎncă nu există evaluări
- Perspective: New England Journal MedicineDocument4 paginiPerspective: New England Journal MedicineGary MaoÎncă nu există evaluări
- An Evidence-Based Approach To Pediatric MelanonychiaDocument13 paginiAn Evidence-Based Approach To Pediatric MelanonychiaMarice QCÎncă nu există evaluări
- AFP Tumor Markers: The TestDocument20 paginiAFP Tumor Markers: The TestMuhammad Umar SaleemÎncă nu există evaluări
- World Journal of Radiology PDFDocument8 paginiWorld Journal of Radiology PDFniluhÎncă nu există evaluări
- Sickle Cell - RahafDocument39 paginiSickle Cell - RahafgalalÎncă nu există evaluări
- Common Poison in ChildrenDocument31 paginiCommon Poison in ChildrenNimi BatuboÎncă nu există evaluări
- Care Plan TemplateDocument8 paginiCare Plan TemplateXosweetbebeÎncă nu există evaluări
- Effectiveness of Psychotherapy On Suicidal Risk - A Systematic Review of Observational Studies (MENDEZ, Et Al, 2019)Document10 paginiEffectiveness of Psychotherapy On Suicidal Risk - A Systematic Review of Observational Studies (MENDEZ, Et Al, 2019)JAVIERA CONSTANZA MUÑOZ VERGARAÎncă nu există evaluări
- U1L7 Student Guide (1) - 1Document4 paginiU1L7 Student Guide (1) - 1jonahÎncă nu există evaluări