S-ar putea să vă placă și
- Toy Cutting Fruits Velcro Playset KitchenDocument1 paginăToy Cutting Fruits Velcro Playset KitchenWely Tiffani YpÎncă nu există evaluări
- AntihipertensiDocument1 paginăAntihipertensiWely Tiffani YpÎncă nu există evaluări
- Pre EklampsiaDocument10 paginiPre EklampsiaWely Tiffani YpÎncă nu există evaluări
- PMK No. 7 TH 2018 TTG Perubahan Penggolongan NarkotikaDocument24 paginiPMK No. 7 TH 2018 TTG Perubahan Penggolongan NarkotikayuliyujeÎncă nu există evaluări
- Correlation Between Folic Acid and Homocysteine Plasma in Severe Pre-Eclampsia and Normal PregnancyDocument18 paginiCorrelation Between Folic Acid and Homocysteine Plasma in Severe Pre-Eclampsia and Normal PregnancyWely Tiffani YpÎncă nu există evaluări
- Correlation Between Folic Acid and Homocysteine Plasma in Severe Pre-Eclampsia and Normal PregnancyDocument18 paginiCorrelation Between Folic Acid and Homocysteine Plasma in Severe Pre-Eclampsia and Normal PregnancyWely Tiffani YpÎncă nu există evaluări
- Triple Antiretroviral Therapy Effectively Eliminates HIV Transmission From Mother To ChildDocument4 paginiTriple Antiretroviral Therapy Effectively Eliminates HIV Transmission From Mother To ChildWely Tiffani YpÎncă nu există evaluări
- Triple Antiretroviral Therapy Effectively Eliminates HIV Transmission From Mother To ChildDocument4 paginiTriple Antiretroviral Therapy Effectively Eliminates HIV Transmission From Mother To ChildWely Tiffani YpÎncă nu există evaluări
- Preeclampsia With HELLP SyndromeDocument8 paginiPreeclampsia With HELLP SyndromeWely Tiffani YpÎncă nu există evaluări
- Preeclampsia With HELLP SyndromeDocument8 paginiPreeclampsia With HELLP SyndromeWely Tiffani YpÎncă nu există evaluări
- BiomolekulerDocument137 paginiBiomolekulerNicylaÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Chemotherapy ToxicityDocument37 paginiChemotherapy ToxicityCarlos Eduardo Cadu100% (1)
- Seminar Obgyn Chemotheraphy in GynaecologyDocument38 paginiSeminar Obgyn Chemotheraphy in GynaecologyRoshandiep GillÎncă nu există evaluări
- Oncology High Alert Medications ListDocument3 paginiOncology High Alert Medications ListAbdur RachmanÎncă nu există evaluări
- Anticancer DrugsDocument67 paginiAnticancer Drugsoh hello thereÎncă nu există evaluări
- Medical Abbreviations With Multiple Meanings: A Prescription For DisasterDocument4 paginiMedical Abbreviations With Multiple Meanings: A Prescription For DisasterNani ReedÎncă nu există evaluări
- Synergistic Activation of Doxorubicin Against Cancer: A ReviewDocument6 paginiSynergistic Activation of Doxorubicin Against Cancer: A ReviewArya GuganÎncă nu există evaluări
- Anti Cancer DrugsDocument4 paginiAnti Cancer Drugsnerdo1999Încă nu există evaluări
- Antimetabolite, alkylating agent & antibiotic antitumor drugs MOA & useDocument11 paginiAntimetabolite, alkylating agent & antibiotic antitumor drugs MOA & useAmina AmiarÎncă nu există evaluări
- Anti Cancer DrugsDocument56 paginiAnti Cancer DrugsTimothy David50% (2)
- (Recent Advances in Phytochemistry 33) Gordon M. Cragg - Michael R. Boyd (Auth.) - John T. Romeo (Eds.) - Phytochemicals in Human Health Protection - Nutrition - and Plant Defense-Springer US (1999)Document436 pagini(Recent Advances in Phytochemistry 33) Gordon M. Cragg - Michael R. Boyd (Auth.) - John T. Romeo (Eds.) - Phytochemicals in Human Health Protection - Nutrition - and Plant Defense-Springer US (1999)hakimcabÎncă nu există evaluări
- Oncotarget 09 9114Document23 paginiOncotarget 09 9114Kerezsiné Kovács Erika RozáliaÎncă nu există evaluări
- Fasting and Fasting-Mimicking Diets For ChemotherapyDocument16 paginiFasting and Fasting-Mimicking Diets For ChemotherapyHuman ResourcesÎncă nu există evaluări
- Linfoma de HodgkinDocument44 paginiLinfoma de Hodgkindochas666Încă nu există evaluări
- ALL - Interim Guideline v3Document59 paginiALL - Interim Guideline v3Awais Ul Hassan67% (3)
- GUI - Final - Referencing - Approved - Oct 2020Document18 paginiGUI - Final - Referencing - Approved - Oct 2020Proschool HyderabadÎncă nu există evaluări
- Review Questions On Antiviral and AntibioticDocument63 paginiReview Questions On Antiviral and AntibioticusedforfunplocÎncă nu există evaluări
- Hyper CvadDocument5 paginiHyper CvadAmr MuhammedÎncă nu există evaluări
- Immunology & Oncology Review 2Document99 paginiImmunology & Oncology Review 2Melchor Felipe SalvosaÎncă nu există evaluări
- Advanced Drug Delivery Reviews: Vladimir TorchilinDocument5 paginiAdvanced Drug Delivery Reviews: Vladimir Torchilinvishal makadiaÎncă nu există evaluări
- Finding Opportunity in Uncertainty-Introductory Chapter PDFDocument21 paginiFinding Opportunity in Uncertainty-Introductory Chapter PDFHimanshu SaxenaÎncă nu există evaluări
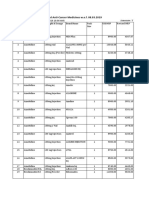
- Revised MRP of Non-Scheduled Anti-Cancer MedicinesDocument23 paginiRevised MRP of Non-Scheduled Anti-Cancer Medicinessampath seshadri100% (1)
- JCO.2011.39.9436.Full - JCO Executive Summary PDFDocument10 paginiJCO.2011.39.9436.Full - JCO Executive Summary PDFMónica Tallón GÎncă nu există evaluări
- Gao 2016Document15 paginiGao 2016kevin gelaudeÎncă nu există evaluări
- AntimetaboliteDocument53 paginiAntimetaboliteRahul LokhandeÎncă nu există evaluări
- Product Information: Adriamycin Solution For InjectionDocument18 paginiProduct Information: Adriamycin Solution For InjectionArya GuganÎncă nu există evaluări
- Engineered Nanoparticles For Drug Delivery in CancerDocument46 paginiEngineered Nanoparticles For Drug Delivery in CancerBrunaÎncă nu există evaluări
- Antibiotic (Bacteriostatic) DrugsDocument15 paginiAntibiotic (Bacteriostatic) DrugsVictor LeeÎncă nu există evaluări
- Antibiotics For Cancer Treatment: A Double-Edged SwordDocument15 paginiAntibiotics For Cancer Treatment: A Double-Edged SwordRushikesh G ParitÎncă nu există evaluări
- BREAST CANCER CLINICAL PHARMACY PRESENTATIONDocument21 paginiBREAST CANCER CLINICAL PHARMACY PRESENTATIONfrankÎncă nu există evaluări
- ATI Prototype DrugsDocument11 paginiATI Prototype Drugsjinnyduong100% (1)