S-ar putea să vă placă și
- Helicobacter Pylori InfectionDocument18 paginiHelicobacter Pylori InfectionPMÎncă nu există evaluări
- Narrative Report in ReadingDocument8 paginiNarrative Report in ReadingSarahMostolesBambalanÎncă nu există evaluări
- Phil IRI Pretest Oral Reading Passage in English 2 7 LearnersDocument7 paginiPhil IRI Pretest Oral Reading Passage in English 2 7 LearnersSer Dodong100% (1)
- Grade6 Eng Reading - Catch Up FridayDocument7 paginiGrade6 Eng Reading - Catch Up FridayJohn Lloyd Kuizon100% (1)
- Set Achievable and Appropriate Learning Outcomes That Aligned With Learning CompetenciesDocument4 paginiSet Achievable and Appropriate Learning Outcomes That Aligned With Learning Competenciesmhlq14100% (1)
- Department of Education: Republic of The PhilippinesDocument33 paginiDepartment of Education: Republic of The PhilippinesSaluibTanMel100% (1)
- Knopp2017 Article OnceACheaterAlwaysACheaterSeriDocument11 paginiKnopp2017 Article OnceACheaterAlwaysACheaterSeriAnda F. CotoarăÎncă nu există evaluări
- Cs Form 86 - Health Examination RecordDocument2 paginiCs Form 86 - Health Examination RecordEdmon-Ivy Lynn Sosing-Giray Tan85% (20)
- NATG6 Stratified Sampling TemplateDocument148 paginiNATG6 Stratified Sampling Templatericlane apoleÎncă nu există evaluări
- (Appendix C-03) COT-RPMS Rating Sheet For T I-III For SY 2023-2024Document1 pagină(Appendix C-03) COT-RPMS Rating Sheet For T I-III For SY 2023-2024mariahvanessa.soto100% (4)
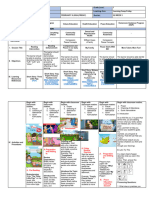
- DLL Catch Up Friday Week 3Document6 paginiDLL Catch Up Friday Week 3Maryanne Labaso86% (7)
- Catch Up Fridays Orientation PresentationDocument21 paginiCatch Up Fridays Orientation PresentationJOSEVIE CABISAYÎncă nu există evaluări
- 2mw Biomass Gasification Gas Power Plant ProposalDocument9 pagini2mw Biomass Gasification Gas Power Plant ProposalsabrahimaÎncă nu există evaluări
- English-LESSON PLAN - SELECTION 2Document1 paginăEnglish-LESSON PLAN - SELECTION 2Isabel R Ortega50% (2)
- 2023 KRA's and ObjectivesDocument8 pagini2023 KRA's and ObjectivesJay Ar Jones TrompetaÎncă nu există evaluări
- Deped Standard Certificate TemplatesDocument2 paginiDeped Standard Certificate TemplatesLicca Argallon100% (1)
- Teaching Guide Catchup Template Health Grade4Document4 paginiTeaching Guide Catchup Template Health Grade4NEIL CARLO ARCEGAÎncă nu există evaluări
- School Form 2 (SF2) Daily Attendance Report of LearnersDocument25 paginiSchool Form 2 (SF2) Daily Attendance Report of LearnersMelinda Rafael100% (1)
- COT RPMS TI III Inter Observer Agreement FormDocument1 paginăCOT RPMS TI III Inter Observer Agreement FormDenelleJamoloMorancil50% (2)
- Nursing Care Plan For Readiness For Enhanced Sleep NCPDocument4 paginiNursing Care Plan For Readiness For Enhanced Sleep NCPderic100% (2)
- MTMASDocument2 paginiMTMASUlquiorra Garcia100% (1)
- RPMS Design 5Document24 paginiRPMS Design 5Ann GaniaÎncă nu există evaluări
- INSET TOS and Test ConstructionDocument47 paginiINSET TOS and Test ConstructionRiza Garganza100% (1)
- New DLL Blank FormDocument5 paginiNew DLL Blank FormAlcazar Renz Justine60% (5)
- Dr. Loida N. Nidea, Ceso V: V.Bagasina Sr. Memorial High SchoolDocument3 paginiDr. Loida N. Nidea, Ceso V: V.Bagasina Sr. Memorial High SchoolJanet VasquezÎncă nu există evaluări
- Pulverizers: By: G. RamachandranDocument140 paginiPulverizers: By: G. Ramachandranshivshankar prajapatiÎncă nu există evaluări
- Heat Shrink CoatingDocument5 paginiHeat Shrink CoatingMekhmanÎncă nu există evaluări
- Understanding RPMS PPST Targets and Features of Practice Final 1Document58 paginiUnderstanding RPMS PPST Targets and Features of Practice Final 1HELEN CONARCO100% (2)
- DLL Reading Program Sy23 24Document2 paginiDLL Reading Program Sy23 24Mark BaniagaÎncă nu există evaluări
- LAC SG - Session 15 Figuring It Out - Drawing Conclusions and Generalizations of The Selections - ONLINE - EditedDocument8 paginiLAC SG - Session 15 Figuring It Out - Drawing Conclusions and Generalizations of The Selections - ONLINE - Editedangeli100% (5)
- Annex A2 RPMS Tool For Proficient Teachers SY 2023-2024Document20 paginiAnnex A2 RPMS Tool For Proficient Teachers SY 2023-2024Jackie Lyn Ramos100% (4)
- Catch Up PlanDocument5 paginiCatch Up PlanKateVeralloÎncă nu există evaluări
- Template 2 3 SCHOOL QUARTERLY TEST MPS REPORT OVERALL AND BY GRADE SECONDARY LEVEL FINALDocument22 paginiTemplate 2 3 SCHOOL QUARTERLY TEST MPS REPORT OVERALL AND BY GRADE SECONDARY LEVEL FINALmichelle manito100% (2)
- RPMS ChecklistDocument3 paginiRPMS ChecklistMarkus100% (2)
- Individual Oral Reading Observation Checklist: Walang Pagbabago Ang Tono)Document10 paginiIndividual Oral Reading Observation Checklist: Walang Pagbabago Ang Tono)Joanna Marie VillamarÎncă nu există evaluări
- Ipcrf Development Plan 2023 2024Document1 paginăIpcrf Development Plan 2023 2024ErnestoJarapaJr100% (1)
- FULLER APPROACH - Lesson 1 93Document22 paginiFULLER APPROACH - Lesson 1 93Jahyala KristalÎncă nu există evaluări
- HOMEROOM GUIDANCE LEARNER'S DEVELOPMENT ASSESSMENT (Grade 4-6) - DepedtambayanDocument2 paginiHOMEROOM GUIDANCE LEARNER'S DEVELOPMENT ASSESSMENT (Grade 4-6) - DepedtambayanMargie Rodriguez100% (2)
- Phil-IRI Group Screening Answer Sheet (ENGLISH) Grade 3Document5 paginiPhil-IRI Group Screening Answer Sheet (ENGLISH) Grade 3Darien Tayag AloroÎncă nu există evaluări
- Phil-Iri Answer Sheet (GST)Document2 paginiPhil-Iri Answer Sheet (GST)Abigail Fritz GoloÎncă nu există evaluări
- SESSION 2 Difficulty in Performing Adaptive Skills Deaf BlindnessDocument52 paginiSESSION 2 Difficulty in Performing Adaptive Skills Deaf BlindnessCharie Enrile-JaleÎncă nu există evaluări
- Medical Certificate: Department of EducationDocument1 paginăMedical Certificate: Department of EducationCamille Organis100% (2)
- Answers To LDM Module 1-5Document33 paginiAnswers To LDM Module 1-5Lielet MatutinoÎncă nu există evaluări
- Disbursement Voucher - DepEdDocument1 paginăDisbursement Voucher - DepEdJ LÎncă nu există evaluări
- CS FORM 41 Medical CertificateDocument2 paginiCS FORM 41 Medical Certificatedoña Aurora100% (2)
- Consolidated Report On Individual Learning Monitoring PlanDocument2 paginiConsolidated Report On Individual Learning Monitoring PlanJomajFalcatanDelaCruzÎncă nu există evaluări
- Department of Education Division of Zamboanga Del Sur: Ramon Magsaysay DistrictDocument2 paginiDepartment of Education Division of Zamboanga Del Sur: Ramon Magsaysay DistrictReia Dagohoy100% (1)
- Oral Reading Verification PassagesDocument1 paginăOral Reading Verification PassagesMarichele Liwag Pagaragan100% (2)
- Paghahawan NG BalakidDocument21 paginiPaghahawan NG BalakidKATRINE JOYCE CRISTOBALÎncă nu există evaluări
- Department of Education: - Elementary School Learner'S Information SheetDocument2 paginiDepartment of Education: - Elementary School Learner'S Information SheetRouselle Umagat RaraÎncă nu există evaluări
- Weekly Accomplishment ReportDocument10 paginiWeekly Accomplishment ReportMa. Victoria LlameraÎncă nu există evaluări
- SPED-Tagging Tutorial GuideDocument4 paginiSPED-Tagging Tutorial GuideBong Bandola100% (2)
- Activity Design 1 - Differentiated InstructionDocument2 paginiActivity Design 1 - Differentiated InstructionLuz Marie CorveraÎncă nu există evaluări
- Appendix C 02 COT RPMS Rating Sheet For T I III For SY 2022 2023Document4 paginiAppendix C 02 COT RPMS Rating Sheet For T I III For SY 2022 2023Revie Joy Bugsangit Bentillo-OliverosÎncă nu există evaluări
- Appendix C 02 COT RPMS Rating Sheet For T I III For SY 2022 2023Document1 paginăAppendix C 02 COT RPMS Rating Sheet For T I III For SY 2022 2023Klaudette AsuncionÎncă nu există evaluări
- How To Encode Pds For Hris Step by Step InstructionsDocument11 paginiHow To Encode Pds For Hris Step by Step Instructionsjean nazarenoÎncă nu există evaluări
- (Appendix C-03) COT-RPMS Rating Sheet For T I-III For SY 2023-2024Document1 pagină(Appendix C-03) COT-RPMS Rating Sheet For T I-III For SY 2023-2024Rommel Duatin100% (2)
- Teacher's Program 2021 - 2022Document2 paginiTeacher's Program 2021 - 2022John Darryl Caysido100% (1)
- Summative Test No. 2 Tle 6Document2 paginiSummative Test No. 2 Tle 6windy mirandaÎncă nu există evaluări
- VI-2 Phil-Iri-Filipino-Automated - 2019-2020Document48 paginiVI-2 Phil-Iri-Filipino-Automated - 2019-2020baldo yellow4Încă nu există evaluări
- Accomplishment - Project Dear-Sy2019-2020Document8 paginiAccomplishment - Project Dear-Sy2019-2020Sheena Claire dela Pe?Încă nu există evaluări
- Department of Education: Individual Daily Log and Accomplishment ReportDocument2 paginiDepartment of Education: Individual Daily Log and Accomplishment ReportJoelmarMondonedoÎncă nu există evaluări
- DLL - English 2 - Q1 - W2Document3 paginiDLL - English 2 - Q1 - W2Glene M CarbonelÎncă nu există evaluări
- Department of Education: Republic of The PhilippinesDocument3 paginiDepartment of Education: Republic of The PhilippinesARVID REE LOMERAÎncă nu există evaluări
- Health Examination Form: Instruction For FilingDocument3 paginiHealth Examination Form: Instruction For FilingJonathanÎncă nu există evaluări
- Form No. 86 Health Examination FormDocument1 paginăForm No. 86 Health Examination FormJielyn Macorol NorioÎncă nu există evaluări
- Remote Control RC902V1 ManualDocument3 paginiRemote Control RC902V1 ManualdezdoÎncă nu există evaluări
- Ball Bearing Units Stainless SeriesDocument5 paginiBall Bearing Units Stainless SeriesRicardo KharisÎncă nu există evaluări
- 50-Article Text-116-1-10-20191113Document6 pagini50-Article Text-116-1-10-20191113Annisa FauziahÎncă nu există evaluări
- Teri MicorisaDocument7 paginiTeri MicorisabiodieselnetÎncă nu există evaluări
- การทดสอบแรงต้านแรงเฉือนแบบแรงเฉือนโดยตรง Direct Shear Test: Table 1 Sample DataDocument5 paginiการทดสอบแรงต้านแรงเฉือนแบบแรงเฉือนโดยตรง Direct Shear Test: Table 1 Sample DataTomorrowÎncă nu există evaluări
- The Effect of Gas Metal Arc Welding (GMAW) Processes On Different Welding Parameters - DoneDocument5 paginiThe Effect of Gas Metal Arc Welding (GMAW) Processes On Different Welding Parameters - DoneAsim AliÎncă nu există evaluări
- Future Proofing Cities Toolkit by Craig Applegath 2012-03-01sm PDFDocument20 paginiFuture Proofing Cities Toolkit by Craig Applegath 2012-03-01sm PDFJorge Fernández BaluarteÎncă nu există evaluări
- ErostorysDocument19 paginiErostorysMayLiuÎncă nu există evaluări
- Form Apr 22 2022Document4 paginiForm Apr 22 2022api-589628245Încă nu există evaluări
- Perdev - Module 9Document9 paginiPerdev - Module 9April Rose CortesÎncă nu există evaluări
- NSF 型錄2Document2 paginiNSF 型錄2Nermeen ElmelegaeÎncă nu există evaluări
- 2457-Article Text-14907-2-10-20120724Document6 pagini2457-Article Text-14907-2-10-20120724desi meleniaÎncă nu există evaluări
- Types of Shops Shopping: 1. Chemist's 2. Grocer's 3. Butcher's 4. Baker'sDocument1 paginăTypes of Shops Shopping: 1. Chemist's 2. Grocer's 3. Butcher's 4. Baker'sMonik IonelaÎncă nu există evaluări
- JEE Mains 2024 Question Paper Shift 2 27 JanDocument4 paginiJEE Mains 2024 Question Paper Shift 2 27 JanAnjali SahooÎncă nu există evaluări
- Corporate Security Policy TemplateDocument4 paginiCorporate Security Policy TemplateCoronaÎncă nu există evaluări
- Genomics and Crop ImprovementDocument56 paginiGenomics and Crop Improvementsenguvelan100% (6)
- 2006 SM600Document2 pagini2006 SM600Ioryogi KunÎncă nu există evaluări
- User's Manual Eco Friendly Park BenchDocument35 paginiUser's Manual Eco Friendly Park BenchAmirulHanif AlyahyaÎncă nu există evaluări
- Cen-Tech 63759Document8 paginiCen-Tech 63759GregÎncă nu există evaluări
- Job Vacancy Kabil - Batam April 2017 RECARE PDFDocument2 paginiJob Vacancy Kabil - Batam April 2017 RECARE PDFIlham AdeÎncă nu există evaluări
- Comparative Study of Financial Statements of Company, Oil and Gas.Document105 paginiComparative Study of Financial Statements of Company, Oil and Gas.Ray Brijesh AjayÎncă nu există evaluări
- Narrative Report On Conduct of Classes-October 2021Document1 paginăNarrative Report On Conduct of Classes-October 2021Jansen Roy D. JaraboÎncă nu există evaluări
- Publication PDFDocument152 paginiPublication PDFAlicia Mary PicconeÎncă nu există evaluări
- Crew Resource Management Phil O'DonnellDocument39 paginiCrew Resource Management Phil O'DonnellMostafaÎncă nu există evaluări