S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Star Health Medi Premier BrochureDocument2 paginiStar Health Medi Premier BrochureBhaktha SinghÎncă nu există evaluări
- Cardiac Case StudyDocument3 paginiCardiac Case StudyJessi ParsonsÎncă nu există evaluări
- Dynamic Psychotherapy PDFDocument603 paginiDynamic Psychotherapy PDFfllorinv775% (4)
- Join Pakistan Army in Armed Forces Nursing Service (AFNS) ENTRY 2019/2020Document2 paginiJoin Pakistan Army in Armed Forces Nursing Service (AFNS) ENTRY 2019/2020Arslan BashirÎncă nu există evaluări
- Problem-Based Research PaperDocument8 paginiProblem-Based Research Paperapi-457674200Încă nu există evaluări
- Plastic Surgery SummaryDocument30 paginiPlastic Surgery SummaryLailaAliÎncă nu există evaluări
- Evaluating A Case Study Using Bloom's Taxonomy of Education: ASE TudyDocument10 paginiEvaluating A Case Study Using Bloom's Taxonomy of Education: ASE TudyAli RaufÎncă nu există evaluări
- MST Nursing HandoutDocument3 paginiMST Nursing Handoutapi-261265221Încă nu există evaluări
- Lanao Chung Hua School Pala-O, Iligan City: General InstructionsDocument7 paginiLanao Chung Hua School Pala-O, Iligan City: General InstructionsDawn FernandezÎncă nu există evaluări
- Finish Application Selection CriteriaDocument2 paginiFinish Application Selection Criteriaapi-322710565Încă nu există evaluări
- HughLaurie ST James InfirmaryDocument7 paginiHughLaurie ST James InfirmaryjoeÎncă nu există evaluări
- Jeanne Kenney DepositionDocument225 paginiJeanne Kenney DepositionMarkingsonCaseÎncă nu există evaluări
- Nursing Assessment and Physical ExaminationDocument5 paginiNursing Assessment and Physical ExaminationTaufik Rohman0% (1)
- 2013 Scope of Appointment Form - CORBINDocument2 pagini2013 Scope of Appointment Form - CORBINCorbin LindseyÎncă nu există evaluări
- Annexure A6-8 A4Document15 paginiAnnexure A6-8 A4bathinsreenivasÎncă nu există evaluări
- Complete Medical Surgical 2nd Year Course PlanDocument9 paginiComplete Medical Surgical 2nd Year Course Planvipin sharmaÎncă nu există evaluări
- Post-Seclusion And/or Restraint Review in Psychiatry: A Scoping Review Article OutlineDocument27 paginiPost-Seclusion And/or Restraint Review in Psychiatry: A Scoping Review Article OutlineStudentnurseMjÎncă nu există evaluări
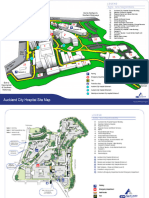
- ACH Site MapTWTDocument2 paginiACH Site MapTWTyashacnzÎncă nu există evaluări
- Documentation of Nutrition CareDocument51 paginiDocumentation of Nutrition CareBrix ValdrizÎncă nu există evaluări
- 4-8-1-989 Format For SynopsisDocument7 pagini4-8-1-989 Format For SynopsisYashoda SatputeÎncă nu există evaluări
- Palliative Care Practice and Associated Factors Among Nurses Working in Jimma University Medical Center South-West Ethiopia, 2017Document8 paginiPalliative Care Practice and Associated Factors Among Nurses Working in Jimma University Medical Center South-West Ethiopia, 2017Diani Rista SariÎncă nu există evaluări
- Ward ManagementDocument5 paginiWard ManagementVeeresh TopalakattiÎncă nu există evaluări
- Bus Writing Linc5Document50 paginiBus Writing Linc5manuÎncă nu există evaluări
- Outpatient Teaching Lecture NotesDocument1 paginăOutpatient Teaching Lecture NotesdnaritaÎncă nu există evaluări
- May 2013 Notices Ohio Board of NursingDocument703 paginiMay 2013 Notices Ohio Board of NursingJames LindonÎncă nu există evaluări
- Emergency Response Team (Ert) and Fire Safety Training: By: Mr. Antonio Zacarias JRDocument44 paginiEmergency Response Team (Ert) and Fire Safety Training: By: Mr. Antonio Zacarias JRShah Newaz KabirÎncă nu există evaluări
- Hospital Management System: Presented by GroupDocument29 paginiHospital Management System: Presented by GroupsamdhathriÎncă nu există evaluări
- SONGS OF WILLOW FROST by Jamie FordDocument24 paginiSONGS OF WILLOW FROST by Jamie FordRandom House Publishing Group100% (1)
- Ap Chief Minister'S Relief FundDocument6 paginiAp Chief Minister'S Relief Fundiqbal1439988100% (1)
- Hospital Application Guide SchneiderDocument51 paginiHospital Application Guide SchneiderSundaresan SabanayagamÎncă nu există evaluări