S-ar putea să vă placă și
- A Child With An Epileptic Status With Growth FalteringDocument25 paginiA Child With An Epileptic Status With Growth FalteringHasan HusienÎncă nu există evaluări
- First Seizure-RCEMDocument2 paginiFirst Seizure-RCEMalsadiqbr5Încă nu există evaluări
- Neurological DisordersDocument6 paginiNeurological DisordersSoojung Nam100% (3)
- Febrile SeizuresDocument1 paginăFebrile SeizuresDiana AlexandraÎncă nu există evaluări
- Pediatric Neurology Referral Guidelines: Table of ContentsDocument10 paginiPediatric Neurology Referral Guidelines: Table of ContentsEvannelson WardhanaÎncă nu există evaluări
- Ihm - Febril SeizureDocument1 paginăIhm - Febril SeizureEmmy 1432Încă nu există evaluări
- Truspected Stroke AlgorithmDocument4 paginiTruspected Stroke Algorithmtri wahyunoÎncă nu există evaluări
- Seizure Disorders: Nursing ManagementDocument3 paginiSeizure Disorders: Nursing ManagementDarren Mae MosadaÎncă nu există evaluări
- Evangelista Pagola Case StudyDocument21 paginiEvangelista Pagola Case StudyMikes CastroÎncă nu există evaluări
- Febrile Seizures 12 - 1 - 2019 3Document12 paginiFebrile Seizures 12 - 1 - 2019 3ninta karinaÎncă nu există evaluări
- Febrile Seizures PathwayDocument10 paginiFebrile Seizures PathwayFerry Abu Irsyad AtthaillahÎncă nu există evaluări
- Ver Tigo A ND Dizziness in The Emergenc y Depar TmentDocument12 paginiVer Tigo A ND Dizziness in The Emergenc y Depar TmentEko SaputraÎncă nu există evaluări
- Hayats ResponsesDocument18 paginiHayats Responsesyacineone01Încă nu există evaluări
- EpilepsiaDocument37 paginiEpilepsiaGrigore AlexandraÎncă nu există evaluări
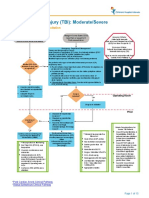
- Traumatic Brain Injury Moderate Severe Clinical PathwayDocument15 paginiTraumatic Brain Injury Moderate Severe Clinical PathwayDobrila SimonovicÎncă nu există evaluări
- High Risk Mild Head InjuryDocument1 paginăHigh Risk Mild Head InjuryMay JPÎncă nu există evaluări
- Seizure New Onset Clinical PathwayDocument17 paginiSeizure New Onset Clinical PathwayKim Shyen BontuyanÎncă nu există evaluări
- Citicoline Drug StudyDocument2 paginiCiticoline Drug StudyJC LumayaÎncă nu există evaluări
- ED Adult NICE Final 1107Document2 paginiED Adult NICE Final 1107Guillermo Calderaro0% (1)
- Febrile Seizures, Febrile Seizure Plus, First Unprovoked Seizure WebinarDocument45 paginiFebrile Seizures, Febrile Seizure Plus, First Unprovoked Seizure WebinarTun Paksi Sareharto100% (1)
- Benign Febrile Seizure: PediatricsDocument2 paginiBenign Febrile Seizure: PediatricsKrista P. AguinaldoÎncă nu există evaluări
- Bacterial MeningitisDocument2 paginiBacterial Meningitisjennielunay00Încă nu există evaluări
- F Seizures AssessDocument1 paginăF Seizures Assessmahmudajannatul.7Încă nu există evaluări
- COP Week 4Document32 paginiCOP Week 4hasti.khaledyanÎncă nu există evaluări
- BCCA AB in Febrile Neutropenia GuidelinesDocument2 paginiBCCA AB in Febrile Neutropenia GuidelinesAlvy SyukrieÎncă nu există evaluări
- 3B2 Preceptorial Nov 18 SFSeizuresDocument79 pagini3B2 Preceptorial Nov 18 SFSeizuresAbigail PaasaÎncă nu există evaluări
- 2017 Stroke in Childhood - Pathway PosterDocument1 pagină2017 Stroke in Childhood - Pathway PosterDeomicah SolanoÎncă nu există evaluări
- Pediatric SeizuresDocument64 paginiPediatric SeizuresShobithaÎncă nu există evaluări
- Seizures and The Epilepsies in Infants, Children, and AdolescentsDocument8 paginiSeizures and The Epilepsies in Infants, Children, and AdolescentsCecille Ann CayetanoÎncă nu există evaluări
- When Should Brain Imaging Precede Lumbar Puncture in Cases of Suspected Bacterial MeningitisDocument3 paginiWhen Should Brain Imaging Precede Lumbar Puncture in Cases of Suspected Bacterial Meningitistsiko111Încă nu există evaluări
- Acute Stroke Management by Carlos L Chua PDFDocument61 paginiAcute Stroke Management by Carlos L Chua PDFHynne Jhea EchavezÎncă nu există evaluări
- 18.d SeizuresDocument6 pagini18.d SeizuresSamantha LuiÎncă nu există evaluări
- Febrile Convulsions Clinical Guideline V4.0 February 2020Document10 paginiFebrile Convulsions Clinical Guideline V4.0 February 2020AzmiÎncă nu există evaluări
- EpilepsyDocument38 paginiEpilepsyB AuÎncă nu există evaluări
- Principles of Seizure ManagementDocument119 paginiPrinciples of Seizure ManagementRenan Toledo SandaloÎncă nu există evaluări
- Endo 5Document1 paginăEndo 5Bea YmsnÎncă nu există evaluări
- Materi I DR HadryastutiDocument38 paginiMateri I DR HadryastutiyuliÎncă nu există evaluări
- Hydrocephalus Clinical Pathway: James L. PatigayonDocument6 paginiHydrocephalus Clinical Pathway: James L. PatigayonJayson OlileÎncă nu există evaluări
- Head Injury: Closed Head Injury EG: Falls, Motor Vehicle Crashes, Bicycle InjuriesDocument13 paginiHead Injury: Closed Head Injury EG: Falls, Motor Vehicle Crashes, Bicycle InjuriesJudy HandlyÎncă nu există evaluări
- Hypoxic Ischemic Encephalopathy (Hie) : AlgorithmDocument11 paginiHypoxic Ischemic Encephalopathy (Hie) : AlgorithmAndreiMunteanuÎncă nu există evaluări
- Farmakoterapi I: EpilepsiDocument83 paginiFarmakoterapi I: EpilepsisafiraÎncă nu există evaluări
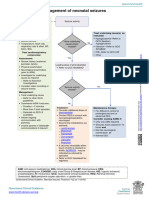
- Neonatal SeizuresDocument33 paginiNeonatal SeizuresNursulfia MaharaniÎncă nu există evaluări
- Battisti Nnconvulsions enDocument130 paginiBattisti Nnconvulsions enangelinaÎncă nu există evaluări
- Dr. I Gusti Ngurah Suwarba, Sp.A (K) Dr. Dewi Sutriani M, Sp.ADocument28 paginiDr. I Gusti Ngurah Suwarba, Sp.A (K) Dr. Dewi Sutriani M, Sp.ASheryl ElitaÎncă nu există evaluări
- Neo SeizureDocument27 paginiNeo SeizureAchyut KanungoÎncă nu există evaluări
- Guillian Barre Astra ZenecaDocument6 paginiGuillian Barre Astra ZenecaGerardo de Gyves AvilaÎncă nu există evaluări
- PREDICTALGORITHM v1 1 29.01.21Document2 paginiPREDICTALGORITHM v1 1 29.01.21selvi zhafirahÎncă nu există evaluări
- Concept Map Meningitis TheoryDocument3 paginiConcept Map Meningitis TheoryMia AuliaÎncă nu există evaluări
- Concept Map Meningitis TheoryDocument3 paginiConcept Map Meningitis TheoryMia AuliaÎncă nu există evaluări
- Hepatitis B VaccineDocument4 paginiHepatitis B VaccineShantal AbelloÎncă nu există evaluări
- Neonatal SeizuresDocument4 paginiNeonatal SeizuresSerag EdeenÎncă nu există evaluări
- Etable 1. Encephalitis Diagnostic Criteria From Selected Published StudiesDocument4 paginiEtable 1. Encephalitis Diagnostic Criteria From Selected Published StudiesNadine N'dilimabakaÎncă nu există evaluări
- Finals - MCN RLEDocument6 paginiFinals - MCN RLEKorean GirlÎncă nu există evaluări
- Convulsive Disorders: Presenters: Kabwe Chanda EliasDocument30 paginiConvulsive Disorders: Presenters: Kabwe Chanda EliasHomeground entertainmentÎncă nu există evaluări
- Pediatric EpilepsyDocument1 paginăPediatric EpilepsyRangel AngelÎncă nu există evaluări
- 1538 Exam 5 IntracranialDocument31 pagini1538 Exam 5 IntracranialJade EdanoÎncă nu există evaluări
- MIni CaseSTUDY pediaWARDDocument10 paginiMIni CaseSTUDY pediaWARDDANIELLA MALARANG MELÎncă nu există evaluări
- NRN 202 Concept Map Patho-Altered Mental StatusDocument1 paginăNRN 202 Concept Map Patho-Altered Mental StatusWendy Gilbert50% (2)
- AAN2023 PedsNCC Case1 Compositeslides 4.13Document14 paginiAAN2023 PedsNCC Case1 Compositeslides 4.13Evelina ȘabanovÎncă nu există evaluări
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicDe la EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicEvaluare: 5 din 5 stele5/5 (1)
- The Effects of Dehydration On Brain Volume - Preliminary ResultsDocument6 paginiThe Effects of Dehydration On Brain Volume - Preliminary ResultsCharina Geofhany DeboraÎncă nu există evaluări
- Comparison of The Effects of Clobazam and Diazepam in Prevention of Recurrent Febrile Seizures PDFDocument5 paginiComparison of The Effects of Clobazam and Diazepam in Prevention of Recurrent Febrile Seizures PDFCharina Geofhany DeboraÎncă nu există evaluări
- 922 FullDocument7 pagini922 FullCharina Geofhany DeboraÎncă nu există evaluări
- Acute Surgical Abdomen: An Unusual Presentation of Pulmonary EmbolusDocument4 paginiAcute Surgical Abdomen: An Unusual Presentation of Pulmonary EmbolusCharina Geofhany DeboraÎncă nu există evaluări
- Acute Cerebral Infarction Masked by A Brain Tumor: Kwo-Whei Lee Chung-Ping LoDocument6 paginiAcute Cerebral Infarction Masked by A Brain Tumor: Kwo-Whei Lee Chung-Ping LoCharina Geofhany DeboraÎncă nu există evaluări
- Operating Room: Ns. Heri Kristianto. Skep., Mkep Department of Medical Surgical NursingDocument21 paginiOperating Room: Ns. Heri Kristianto. Skep., Mkep Department of Medical Surgical NursingNizZa TakaricoÎncă nu există evaluări
- Articulo AcromegaliaDocument10 paginiArticulo AcromegaliaLaura AbrilÎncă nu există evaluări
- Cervical and Vaginal Cytology - Interpretation of Results (Pap Test Report) - UpToDateDocument36 paginiCervical and Vaginal Cytology - Interpretation of Results (Pap Test Report) - UpToDateRoberto López MataÎncă nu există evaluări
- East Meets West Reaction PaperDocument2 paginiEast Meets West Reaction PaperErika Corinne SisonÎncă nu există evaluări
- MdsDocument356 paginiMdsARJUN SreenivasÎncă nu există evaluări
- Kidney AdimeDocument2 paginiKidney Adimeapi-287591907Încă nu există evaluări
- International Journal of Scientific Research and ReviewsDocument11 paginiInternational Journal of Scientific Research and ReviewsHanif ZakariÎncă nu există evaluări
- Ozone Based Waste Water TreatmentDocument10 paginiOzone Based Waste Water TreatmentZafar BukhariÎncă nu există evaluări
- Asthma: MA, Mucus Accumulation MP, Mucus Plug HALV, Hyperinflation of AlveoliDocument34 paginiAsthma: MA, Mucus Accumulation MP, Mucus Plug HALV, Hyperinflation of Alveolidentist40Încă nu există evaluări
- Perawatan Saluran Akar Pada Sisa Akar Gigi Dengan Restorasi DirekDocument7 paginiPerawatan Saluran Akar Pada Sisa Akar Gigi Dengan Restorasi DirekNindya TamayaÎncă nu există evaluări
- HeparinDocument2 paginiHeparinNinoska Garcia-Ortiz100% (4)
- Cholera Guidelines PresentationDocument17 paginiCholera Guidelines PresentationhumphrangoÎncă nu există evaluări
- Non-Surgical Periodontal Therapy Part 1 PDFDocument106 paginiNon-Surgical Periodontal Therapy Part 1 PDFnsr_sweetyÎncă nu există evaluări
- Knotless Bankart Repair Using The Labral SwiveLock® and FiberStick™Document6 paginiKnotless Bankart Repair Using The Labral SwiveLock® and FiberStick™savvoÎncă nu există evaluări
- Daftar Pustaka MeytaDocument3 paginiDaftar Pustaka MeytaAbraham TheodoreÎncă nu există evaluări
- Sharma - Scoring Systems in ConstipationDocument3 paginiSharma - Scoring Systems in ConstipationdocbinÎncă nu există evaluări
- Ayurveda Konyvtar KonyveiDocument23 paginiAyurveda Konyvtar KonyveiPeter Kova'csÎncă nu există evaluări
- Coagulant & AnticoagulantDocument40 paginiCoagulant & AnticoagulantDr Nilesh PatelÎncă nu există evaluări
- Asepsis and InfectionDocument6 paginiAsepsis and InfectionMabes100% (1)
- Quiz 3 Study QuestionsDocument20 paginiQuiz 3 Study QuestionsJessie AllisonÎncă nu există evaluări
- Nutritionist-Dietitian Association of The Philipiines 59th ConventionDocument36 paginiNutritionist-Dietitian Association of The Philipiines 59th ConventionOlive FactorizaÎncă nu există evaluări
- Nota Bene For My ReviewersDocument4 paginiNota Bene For My ReviewersYomadoÎncă nu există evaluări
- 8a - Final Reflection Practicum Alfa RDocument4 pagini8a - Final Reflection Practicum Alfa Rapi-355974373Încă nu există evaluări
- Macro PneumohemoDocument28 paginiMacro PneumohemoSiti AishahÎncă nu există evaluări
- Urinary Tract Infection PIAG 84Document3 paginiUrinary Tract Infection PIAG 84madimadi11Încă nu există evaluări
- Sem4 Preceptor - Rinechia Mcintosh HRH Semester 4 Mary Mcgory K4y 1Document17 paginiSem4 Preceptor - Rinechia Mcintosh HRH Semester 4 Mary Mcgory K4y 1api-314325486Încă nu există evaluări
- Program 2Document152 paginiProgram 2jonathanmr2Încă nu există evaluări
- Antenatal Principles of Antenatal Care 2017Document60 paginiAntenatal Principles of Antenatal Care 2017JanielWright100% (3)
- "My Neck Feels Stiff and There's Pain Coming From It. Every Time I Move It, It Only Gets Worse." As Stated by TheDocument4 pagini"My Neck Feels Stiff and There's Pain Coming From It. Every Time I Move It, It Only Gets Worse." As Stated by TheCassey CuregÎncă nu există evaluări
- A Story of Triumph Over Manic DepressionDocument4 paginiA Story of Triumph Over Manic DepressionclaroblancoÎncă nu există evaluări