S-ar putea să vă placă și
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutDe la EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutEvaluare: 5 din 5 stele5/5 (1)
- Amoebiasis: An Overview of Its Causes, Symptoms, Diagnosis and TreatmentDocument8 paginiAmoebiasis: An Overview of Its Causes, Symptoms, Diagnosis and TreatmentCheska ت HortelanoÎncă nu există evaluări
- Arthropod Written DocumentDocument7 paginiArthropod Written DocumentAngelo Recomo100% (1)
- Walking Pneumonia, (Mycoplasma Pneumonia) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandWalking Pneumonia, (Mycoplasma Pneumonia) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Morpholofy of MoDocument44 paginiMorpholofy of MoPathumavathy RamanathanÎncă nu există evaluări
- Introduction in Medical Microbiology June 2020 Online ClassDocument9 paginiIntroduction in Medical Microbiology June 2020 Online Classjames rukenyaÎncă nu există evaluări
- Sexually Transmitted InfectionsDocument34 paginiSexually Transmitted InfectionsMariana Creciun100% (1)
- Pathology, Vector Studies, and CultureDe la EverandPathology, Vector Studies, and CultureJulius P. KreierEvaluare: 5 din 5 stele5/5 (1)
- Chapter 13 Diagnosing Infectious DiseasesDocument47 paginiChapter 13 Diagnosing Infectious DiseasesSherinne Jane CariazoÎncă nu există evaluări
- Beronio, Gracel Caye M. - Module 2 - AntepartumDocument12 paginiBeronio, Gracel Caye M. - Module 2 - AntepartumGracel Caye Maon BeronioÎncă nu există evaluări
- Amoebiasis in Wild Mammals: Ayesha Ahmed M Phil. Parasitology 1 Semester 2013-Ag-2712Document25 paginiAmoebiasis in Wild Mammals: Ayesha Ahmed M Phil. Parasitology 1 Semester 2013-Ag-2712Abdullah AzeemÎncă nu există evaluări
- Anaerobic Infections in HumansDe la EverandAnaerobic Infections in HumansSydney FinegoldEvaluare: 5 din 5 stele5/5 (1)
- Pathogenesis, Treatment and Prevention of LeishmaniasisDe la EverandPathogenesis, Treatment and Prevention of LeishmaniasisMukesh SamantÎncă nu există evaluări
- Man Meets Microbes: An Introduction to Medical MicrobiologyDe la EverandMan Meets Microbes: An Introduction to Medical MicrobiologyÎncă nu există evaluări
- In The Name of Allah, The Most Beneficent and MercifulDocument35 paginiIn The Name of Allah, The Most Beneficent and MercifulAhmedMenshawyÎncă nu există evaluări
- Clinical Case 04 2019Document12 paginiClinical Case 04 2019Erica Veluz LuyunÎncă nu există evaluări
- Blood and Tissue NematodesDocument37 paginiBlood and Tissue NematodesjelenaÎncă nu există evaluări
- ZIKA VIRUS INFECTION Emerging Public Health ConcernDocument36 paginiZIKA VIRUS INFECTION Emerging Public Health Concerntummalapalli venkateswara rao100% (1)
- Hypophosphatemia, (Low Phosphate) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandHypophosphatemia, (Low Phosphate) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Vaccination or ImmunizationDocument4 paginiVaccination or ImmunizationPrincessÎncă nu există evaluări
- HI Classmates!!!Document36 paginiHI Classmates!!!Alex SilvanoÎncă nu există evaluări
- Measles: PGI Nicole Jenne C. TanDocument40 paginiMeasles: PGI Nicole Jenne C. TanNicole Jenne TanÎncă nu există evaluări
- Entamoeba HistolyticaDocument18 paginiEntamoeba HistolyticaMayuri VohraÎncă nu există evaluări
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- HEPA B and PIDDocument40 paginiHEPA B and PIDNica PinedaÎncă nu există evaluări
- Community Health One LinersDocument30 paginiCommunity Health One LinersRatan YadavÎncă nu există evaluări
- Individual PediaDocument37 paginiIndividual PediaLianna M. MilitanteÎncă nu există evaluări
- Zoonotic Diseases: by Rita NkiroteDocument44 paginiZoonotic Diseases: by Rita NkiroteIsaac JumaÎncă nu există evaluări
- Veterinary Obstetrics IntroductionDocument27 paginiVeterinary Obstetrics IntroductionShakil MahmodÎncă nu există evaluări
- Psychiatric Nursing (Notes) : Alcohol AbuseDocument88 paginiPsychiatric Nursing (Notes) : Alcohol AbuseJulie Ann ParaÎncă nu există evaluări
- ####Bahan Kuliah ISK Blok 23 (Nov 2015)Document32 pagini####Bahan Kuliah ISK Blok 23 (Nov 2015)ajengdmrÎncă nu există evaluări
- Oral Fecal Route Diseases Oral Fecal Route Diseases: Afroz Lakhani RN, BSCNDocument74 paginiOral Fecal Route Diseases Oral Fecal Route Diseases: Afroz Lakhani RN, BSCNafrozlakhaniÎncă nu există evaluări
- VARICELLA PowerpointDocument28 paginiVARICELLA PowerpointMelina SagalaÎncă nu există evaluări
- Rabies - MicrobiologyDocument30 paginiRabies - MicrobiologyMohammed ShakeelÎncă nu există evaluări
- 1 IntroDocument5 pagini1 IntroJeanjayannseptoemanÎncă nu există evaluări
- Acute diarrheal disease caused by Vibrio choleraDocument24 paginiAcute diarrheal disease caused by Vibrio choleracipacipaaÎncă nu există evaluări
- CAD - EBM September 2020 EditionDocument17 paginiCAD - EBM September 2020 EditionNaga Venkatamanoj Kumar PakalapatiÎncă nu există evaluări
- Appendix A: National Unified Health Research Agenda A. DiagnosticsDocument10 paginiAppendix A: National Unified Health Research Agenda A. DiagnosticsKit ChampÎncă nu există evaluări
- Schistosomiasis JaponicaDocument17 paginiSchistosomiasis JaponicaKhairulAmranAn-naml100% (1)
- Protozoans Lecture AmoebaDocument42 paginiProtozoans Lecture Amoebablue_blooded23100% (1)
- Cavite State University: I. ObjectivesDocument7 paginiCavite State University: I. ObjectivesChamy CruzÎncă nu există evaluări
- Hearing Loss Causes: Otosclerosis ExplainedDocument5 paginiHearing Loss Causes: Otosclerosis ExplainedYoko Mae YanoÎncă nu există evaluări
- Microbiology and MycologyDocument76 paginiMicrobiology and MycologyAhmad Said AliÎncă nu există evaluări
- Zoonotic DiseasesDocument27 paginiZoonotic DiseasesGift Summer DinoÎncă nu există evaluări
- Modes of InfectionDocument19 paginiModes of InfectionLinguumÎncă nu există evaluări
- DengueDocument46 paginiDengueMuhammad Ayub KhanÎncă nu există evaluări
- STDs Guide: Gonorrhea to SyphilisDocument5 paginiSTDs Guide: Gonorrhea to Syphilisreghpineda28Încă nu există evaluări
- Epydemiologi AmebiasisDocument6 paginiEpydemiologi AmebiasisRizal FajriÎncă nu există evaluări
- CH 01 The Microbial WorldDocument21 paginiCH 01 The Microbial Worldsammy alan0% (1)
- 8. Care of Child With GI Dysfunction (1) ءءءءDocument44 pagini8. Care of Child With GI Dysfunction (1) ءءءءNuhaÎncă nu există evaluări
- Typhoid Fever: Presented by Sharlin MacalintalDocument18 paginiTyphoid Fever: Presented by Sharlin MacalintalPaul JacksonÎncă nu există evaluări
- H1N1 Diagnosis, Management and TreatmentDocument56 paginiH1N1 Diagnosis, Management and TreatmentNishanth BabuÎncă nu există evaluări
- Theories of Aging: An Overview of Biopsychosocial PerspectivesDocument14 paginiTheories of Aging: An Overview of Biopsychosocial PerspectivesElla Neiza AngelesÎncă nu există evaluări
- SchistosomiasisDocument27 paginiSchistosomiasisNarz Cupahan0% (1)
- A Review On Otitis Media (Karnapaka) : Ayurvedic Aspects and TreatmentDocument4 paginiA Review On Otitis Media (Karnapaka) : Ayurvedic Aspects and TreatmentEditor_IAIMÎncă nu există evaluări
- 3a 3c 4 Dopamine, A Neurotransmitter Located Primarily in TheDocument1 pagină3a 3c 4 Dopamine, A Neurotransmitter Located Primarily in The알파Încă nu există evaluări
- Pathophysiology of FractureDocument2 paginiPathophysiology of Fracturemyer pasandalanÎncă nu există evaluări
- Analogy Test With Answers PDFDocument13 paginiAnalogy Test With Answers PDFsaiÎncă nu există evaluări
- Health AssessmentDocument25 paginiHealth AssessmentGovindaraju Subramani100% (1)
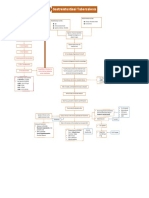
- Gastrointestinal Tuberculosis: PathogenesisDocument1 paginăGastrointestinal Tuberculosis: Pathogenesis알파Încă nu există evaluări
- CUES CholeDocument9 paginiCUES Chole알파Încă nu există evaluări
- Analogy Test With Answers PDFDocument13 paginiAnalogy Test With Answers PDFsaiÎncă nu există evaluări
- Gastrointestinal Tuberculosis: PathogenesisDocument1 paginăGastrointestinal Tuberculosis: Pathogenesis알파Încă nu există evaluări
- Analogy Test With Answers PDFDocument13 paginiAnalogy Test With Answers PDFsaiÎncă nu există evaluări
- Solving Radical Equations Step-by-StepDocument3 paginiSolving Radical Equations Step-by-StepJewel PottÎncă nu există evaluări
- Measuring MatterDocument3 paginiMeasuring Matter알파Încă nu există evaluări
- Gordon's 11 Functional Health PatternsDocument1 paginăGordon's 11 Functional Health PatternsTracy100% (37)
- Oxygen Therapy in Suspected Acute Myocardial InfarctionDocument10 paginiOxygen Therapy in Suspected Acute Myocardial InfarctionPutri YunandaÎncă nu există evaluări
- The Impact of The Tax System On Health Insurance CoverageDocument2 paginiThe Impact of The Tax System On Health Insurance Coverage알파Încă nu există evaluări
- Docslide - Us - Drug Study FormatDocument2 paginiDocslide - Us - Drug Study Format알파Încă nu există evaluări
- Oncology Nursing Management for Cancer Cell GrowthDocument3 paginiOncology Nursing Management for Cancer Cell Growth알파Încă nu există evaluări
- BP TakingDocument4 paginiBP Taking알파Încă nu există evaluări
- Nursing Care for Oncology PatientsDocument35 paginiNursing Care for Oncology Patients알파Încă nu există evaluări
- Nursing Care for Oncology PatientsDocument35 paginiNursing Care for Oncology Patients알파Încă nu există evaluări
- PPP BCCDocument1 paginăPPP BCC알파Încă nu există evaluări
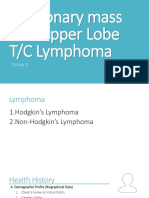
- Pulmonary Mass Left Upper LobeDocument8 paginiPulmonary Mass Left Upper Lobe알파Încă nu există evaluări
- Approaching Disaster Management Through Social Learning 2010Document14 paginiApproaching Disaster Management Through Social Learning 2010알파Încă nu există evaluări
- LMV 014Document5 paginiLMV 014알파Încă nu există evaluări
- Disaster Risk Reduction and Management in The PhilippinesDocument32 paginiDisaster Risk Reduction and Management in The PhilippinesErnan BaldomeroÎncă nu există evaluări
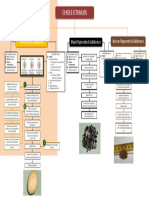
- PPP - CholelithiasisDocument1 paginăPPP - Cholelithiasis알파Încă nu există evaluări
- Triage in Emergency DepartmentDocument25 paginiTriage in Emergency Departmenthatem alsrour91% (11)
- Fluids and Electrolytes: Maintenance of Patent AirwayDocument13 paginiFluids and Electrolytes: Maintenance of Patent Airway알파Încă nu există evaluări
- Gastrointestinal Tuberculosis: PathogenesisDocument1 paginăGastrointestinal Tuberculosis: Pathogenesis알파Încă nu există evaluări
- Immunization Coverage and Adverse Events Following Vaccination A RetrospectiveDocument8 paginiImmunization Coverage and Adverse Events Following Vaccination A RetrospectiveOchechi JosephÎncă nu există evaluări
- Truechemie: Widal (Antigen Agglutination) Test KitDocument1 paginăTruechemie: Widal (Antigen Agglutination) Test Kitfitriadin damayantiÎncă nu există evaluări
- Intervention GuidebookDocument56 paginiIntervention GuidebookSomeonelse47Încă nu există evaluări
- Sexually Transmitted Infections/Diseases or Venereal DiseasesDocument4 paginiSexually Transmitted Infections/Diseases or Venereal DiseasesChristian Pardilla BuenaÎncă nu există evaluări
- The Poisoned Needle by Eleanor McBean (1957) + VACCINATION-A MEDICAL DELUSION by Rex U. LloydDocument186 paginiThe Poisoned Needle by Eleanor McBean (1957) + VACCINATION-A MEDICAL DELUSION by Rex U. Lloydsilent_weeper100% (6)
- Dermatology QuizDocument7 paginiDermatology QuizFaddy OrahaÎncă nu există evaluări
- Drug Inspector 1Document16 paginiDrug Inspector 1dshari100% (1)
- Advances en Pediatrics 2013Document395 paginiAdvances en Pediatrics 2013Gris C. RicoÎncă nu există evaluări
- Ebola: The Natural and Human History of A Deadly Virus (Norton, October 2014), by David QuammenDocument4 paginiEbola: The Natural and Human History of A Deadly Virus (Norton, October 2014), by David QuammenThe World50% (4)
- Haemophilus Species: Characteristics, Pathogenicity and Laboratory DiagnosisDocument26 paginiHaemophilus Species: Characteristics, Pathogenicity and Laboratory DiagnosisCătălina ProcopieÎncă nu există evaluări
- Leaked New Zealand Health Data Had The Government Told The Truth About Vaccine Harms Lives Would HaveDocument8 paginiLeaked New Zealand Health Data Had The Government Told The Truth About Vaccine Harms Lives Would HavemikeÎncă nu există evaluări
- PDF 2342120702Document1 paginăPDF 2342120702Razzak CoolÎncă nu există evaluări
- Mapeh 8 Q3Document5 paginiMapeh 8 Q3Sarah Jane PescadorÎncă nu există evaluări
- Referat Anestesi - Sepsis & Septic ShockDocument36 paginiReferat Anestesi - Sepsis & Septic ShockDimas Arsana PrayogaÎncă nu există evaluări
- VaccinDocument30 paginiVaccinBestari PenyelarasÎncă nu există evaluări
- Exercise 5 InternDocument5 paginiExercise 5 InternJ-Mi AlejanoÎncă nu există evaluări
- Modeling Uganda's Immunization System DynamicsDocument21 paginiModeling Uganda's Immunization System DynamicsTazkiyatun NufusÎncă nu există evaluări
- Grama PriyaDocument5 paginiGrama PriyaRajesh RaiÎncă nu există evaluări
- Guide To OSHA RecordabilityDocument1 paginăGuide To OSHA RecordabilityMuhammadZahirKhanÎncă nu există evaluări
- Euribrid PreviewDocument5 paginiEuribrid PreviewrockfakeyÎncă nu există evaluări
- CertificateDocument1 paginăCertificateajayreddy19103Încă nu există evaluări
- Australia Provides Unequivocal Proof The Covid-19 Vaccines Dont Work and Just Make You WorseDocument8 paginiAustralia Provides Unequivocal Proof The Covid-19 Vaccines Dont Work and Just Make You Worseleon jelcicÎncă nu există evaluări
- Pediatric Residency Training Authors and ContributorsDocument681 paginiPediatric Residency Training Authors and ContributorsVictoria SandersÎncă nu există evaluări
- The Microbiology of Wounds: Neal R. Chamberlain, PH.D., Department of Microbiology/Immunology KcomDocument31 paginiThe Microbiology of Wounds: Neal R. Chamberlain, PH.D., Department of Microbiology/Immunology KcomFhaliesha Zakur100% (1)
- Baby Vaccination ProgramDocument1 paginăBaby Vaccination Programplainspeak100% (1)
- Herpetic Gingivostomatitis in Young ChildrenDocument8 paginiHerpetic Gingivostomatitis in Young ChildrenEunike NabasaÎncă nu există evaluări
- Fake Vaccines in June 2016Document1 paginăFake Vaccines in June 2016Herlinda SoefiyantiÎncă nu există evaluări
- Acusource (Michael Hamilton)Document90 paginiAcusource (Michael Hamilton)Tim Schlank100% (5)
- Barangay Mambog 4 Population and Measles SpreadDocument15 paginiBarangay Mambog 4 Population and Measles SpreadEzerÎncă nu există evaluări
- Chicken-Pox Concept MapDocument4 paginiChicken-Pox Concept MapElle0% (1)