S-ar putea să vă placă și
- Cefoperazone and SulbactumDocument3 paginiCefoperazone and Sulbactumiloveit52252Încă nu există evaluări
- The Essential Guide to Ciprofloxacin: Usage, Precautions, Interactions and Side Effects.De la EverandThe Essential Guide to Ciprofloxacin: Usage, Precautions, Interactions and Side Effects.Încă nu există evaluări
- Magnamycin InjectionDocument8 paginiMagnamycin InjectionHitesh VermaÎncă nu există evaluări
- Cefoperazone Sodium + Sulbactam SodiumDocument17 paginiCefoperazone Sodium + Sulbactam SodiumMuhammad Isnaini ZuhriÎncă nu există evaluări
- Ceftriaxone + TazobactumDocument10 paginiCeftriaxone + Tazobactumnikoseamit7460100% (1)
- CARBAPENEMSDocument87 paginiCARBAPENEMSvijayabhavani.sÎncă nu există evaluări
- OFRAMAX 250 (Injection) OFRAMAX 1 G (Injection)Document4 paginiOFRAMAX 250 (Injection) OFRAMAX 1 G (Injection)mahgadÎncă nu există evaluări
- CefaclorsandozcapDocument9 paginiCefaclorsandozcapseagull70Încă nu există evaluări
- Claforan (Cefotaxime) PDFDocument18 paginiClaforan (Cefotaxime) PDFdinniÎncă nu există evaluări
- Cephalosporins, Flouroquinolones and SulfonamidesDocument7 paginiCephalosporins, Flouroquinolones and SulfonamidesErum JanÎncă nu există evaluări
- Cefprozil Final ProductDocument18 paginiCefprozil Final ProductRathnaganpathi ThulasikumarÎncă nu există evaluări
- Zentel PI - CleanDocument8 paginiZentel PI - CleanMuhammad Abubaker SaleemÎncă nu există evaluări
- Cefotaxime: Cefotaxime (Cefotaxime For Injection) For Injection USP and Dextrose InjectionDocument21 paginiCefotaxime: Cefotaxime (Cefotaxime For Injection) For Injection USP and Dextrose InjectionYaleswari Hayu PertiwiÎncă nu există evaluări
- Aus Pi TargocidDocument5 paginiAus Pi TargocidAsto Ata InteristiÎncă nu există evaluări
- Management of Uncomplicated Urinary Tract InfectionDocument38 paginiManagement of Uncomplicated Urinary Tract Infectionhuddy101Încă nu există evaluări
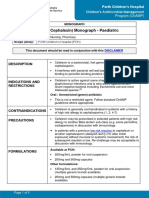
- Cefalexin (Cephalexin) Monograph - Paediatric: DescriptionDocument5 paginiCefalexin (Cephalexin) Monograph - Paediatric: Descriptioneinas omerÎncă nu există evaluări
- New Zealand Data Sheet: 1. Product NameDocument15 paginiNew Zealand Data Sheet: 1. Product NameMhd IjlalÎncă nu există evaluări
- Adult: IV Nosocomial Pneumonia Empiric Therapy For Febrile Neutropenic Patients 4.5Document3 paginiAdult: IV Nosocomial Pneumonia Empiric Therapy For Febrile Neutropenic Patients 4.5Chris Denver BancaleÎncă nu există evaluări
- CeftazidimeDocument16 paginiCeftazidimeNakorn BaisriÎncă nu există evaluări
- Cephalosporins and FriendsDocument4 paginiCephalosporins and FriendsErika De JesusÎncă nu există evaluări
- CephalosporinsDocument52 paginiCephalosporinsapi-306036754Încă nu există evaluări
- Prodoxime 200 1. Composition: - 2. Indications:: Upper Respiratory Tract InfectionDocument8 paginiProdoxime 200 1. Composition: - 2. Indications:: Upper Respiratory Tract InfectionNilisha PradhanÎncă nu există evaluări
- FluconazoleDocument5 paginiFluconazoleGreats HalomoanÎncă nu există evaluări
- Ceftriaxoneinj DEVADocument11 paginiCeftriaxoneinj DEVAMuhammad AwaisÎncă nu există evaluări
- Drug Name: Cefuroxime Generic Name: Axetil PharmacodynamicsDocument3 paginiDrug Name: Cefuroxime Generic Name: Axetil Pharmacodynamicswenz madridÎncă nu există evaluări
- Alclor: Water Used For Reconstitution Should Be Boiled and CooledDocument1 paginăAlclor: Water Used For Reconstitution Should Be Boiled and CooledRubel sheikhÎncă nu există evaluări
- Chloramphenicol: Ayen University - Al College of PharmacyDocument7 paginiChloramphenicol: Ayen University - Al College of Pharmacyمحمد حميد عطيةÎncă nu există evaluări
- Streptogramins (Quinupristin/ Dalfopristin) : Tejal Khade KGRDCP & RiDocument16 paginiStreptogramins (Quinupristin/ Dalfopristin) : Tejal Khade KGRDCP & RiAkshada bhangreÎncă nu există evaluări
- Targocid PI - NewDocument4 paginiTargocid PI - NewDR JAMAL WARISÎncă nu există evaluări
- NETSPAN Injection (Netilmicin Sulfate) : CompositionDocument9 paginiNETSPAN Injection (Netilmicin Sulfate) : CompositionIntan Rizqi RahmawatiÎncă nu există evaluări
- FluconazoleDocument14 paginiFluconazoleasdwasdÎncă nu există evaluări
- AmbrolexDocument4 paginiAmbrolexWeiki Opan FirdausÎncă nu există evaluări
- RotacefDocument2 paginiRotacefBobeico TatianaÎncă nu există evaluări
- Ceftaroline Teflaro CefotaximeDocument3 paginiCeftaroline Teflaro CefotaximeKristi WrayÎncă nu există evaluări
- En Web Insert Cefaz NLDocument3 paginiEn Web Insert Cefaz NLAbdul AzizÎncă nu există evaluări
- Zinex VialDocument5 paginiZinex Vialelcapitano vegetaÎncă nu există evaluări
- Profort VialDocument8 paginiProfort Vialelcapitano vegetaÎncă nu există evaluări
- CefaclorDocument3 paginiCefaclorAyah PaasaÎncă nu există evaluări
- Primaxin IVDocument26 paginiPrimaxin IVkingdom5000Încă nu există evaluări
- Taxim-O Dry Syrup: Cefixime Oral Suspension IPDocument7 paginiTaxim-O Dry Syrup: Cefixime Oral Suspension IPJudy AncyÎncă nu există evaluări
- Gentamicin: Gentamicin 80mg/2mL Injection As Gentamicin SulphateDocument7 paginiGentamicin: Gentamicin 80mg/2mL Injection As Gentamicin SulphateGraciano Aristides MaturbongsÎncă nu există evaluări
- CeftriaxoneaftinjDocument18 paginiCeftriaxoneaftinjbarbawurakÎncă nu există evaluări
- AmoxcillinDocument7 paginiAmoxcillinRoni Sanchez MalanaÎncă nu există evaluări
- Ceftriaxone Monograph - PaediatricDocument6 paginiCeftriaxone Monograph - PaediatricGheorghe Stefan-SorinÎncă nu există evaluări
- TobramycinDocument3 paginiTobramycinAj MillanÎncă nu există evaluări
- Paracetamol Poisoning: G. Rajapandi 521625111 Final MbbsDocument18 paginiParacetamol Poisoning: G. Rajapandi 521625111 Final MbbsAntony PrakashÎncă nu există evaluări
- Unasyn PIDocument8 paginiUnasyn PIfsdfÎncă nu există evaluări
- Unasyn OralDocument10 paginiUnasyn OralAodh OwainÎncă nu există evaluări
- 31Document4 pagini31Noman AliÎncă nu există evaluări
- Gastro Graf in Oral Rectal SuspDocument11 paginiGastro Graf in Oral Rectal SuspPervez Ahmad AhmadÎncă nu există evaluări
- CephalosporinDocument34 paginiCephalosporinliamhenry9449Încă nu există evaluări
- Piperacillin+Tazobactam - TAZOCIN 4.5 G - Leaflet - PfizerDocument12 paginiPiperacillin+Tazobactam - TAZOCIN 4.5 G - Leaflet - PfizerTiaraÎncă nu există evaluări
- Zednad Tablet LeafletDocument2 paginiZednad Tablet LeafletAli KhÎncă nu există evaluări
- Data Sheet: VesicareDocument10 paginiData Sheet: VesicareumarÎncă nu există evaluări
- Cephalosporins: Rama Raju A.V.S PT/2010/04Document20 paginiCephalosporins: Rama Raju A.V.S PT/2010/04Hasitha Shilpa AnantharajuÎncă nu există evaluări
- Stromectol PiDocument7 paginiStromectol PiZainul AnwarÎncă nu există evaluări
- Pharmacology of Antiparasit DrugsDocument40 paginiPharmacology of Antiparasit Drugsakun scribÎncă nu există evaluări
- Gentamycin: Classification of Antihypertensive DrugsDocument3 paginiGentamycin: Classification of Antihypertensive DrugsMargo Milad Fahim SaadÎncă nu există evaluări
- EPIGENTDocument3 paginiEPIGENTmahgad100% (1)
- Oxazolo Activit PDFDocument24 paginiOxazolo Activit PDFImen MiminaÎncă nu există evaluări
- Excipient Performance - General Chapter USP 38Document19 paginiExcipient Performance - General Chapter USP 38Anonymous SDUIPeqXÎncă nu există evaluări
- Rabbit Eye Expt.Document3 paginiRabbit Eye Expt.Padmanabha Gowda100% (1)
- Most Common Food-Drug InteractionsDocument17 paginiMost Common Food-Drug InteractionsNazi AwanÎncă nu există evaluări
- Presentation Musa NserekoDocument53 paginiPresentation Musa NserekogeekindiaÎncă nu există evaluări
- Central Bank Moves On Rates: Birth Control Pulled From Shelves On Police OrdersDocument54 paginiCentral Bank Moves On Rates: Birth Control Pulled From Shelves On Police OrdersThe Myanmar TimesÎncă nu există evaluări
- Regulatory Toxicology (I - Semester) : Principles and Methods in ToxicologyDocument15 paginiRegulatory Toxicology (I - Semester) : Principles and Methods in ToxicologyHARI HARA RAO GUJJARÎncă nu există evaluări
- Otc Template Pi BromhexineDocument2 paginiOtc Template Pi BromhexineHadzrie HamdanÎncă nu există evaluări
- Pharmaceutics and CosmetologyDocument8 paginiPharmaceutics and Cosmetologytirupati_rasalaÎncă nu există evaluări
- General Pharmacology) 343 (Document28 paginiGeneral Pharmacology) 343 (ALNAKI100% (1)
- IV Infusion NumericalsDocument2 paginiIV Infusion NumericalsYarfa KhurramÎncă nu există evaluări
- Ijpab 2015 3 1 224 235 PDFDocument12 paginiIjpab 2015 3 1 224 235 PDFDrAmit VermaÎncă nu există evaluări
- Comprehensive Drug Study KetoanalogueDocument2 paginiComprehensive Drug Study KetoanalogueDolly Benitez100% (9)
- Travco Products v. Wedgewood Village PharmacyDocument5 paginiTravco Products v. Wedgewood Village PharmacyPriorSmartÎncă nu există evaluări
- 1 - DS SATK Form - Initial Application of LTO 1.1Document4 pagini1 - DS SATK Form - Initial Application of LTO 1.1Rudejane TanÎncă nu există evaluări
- Consideraciones Practicas en La Administracion y Dosis de Cannabis MedicinalDocument8 paginiConsideraciones Practicas en La Administracion y Dosis de Cannabis MedicinalGerardo QGÎncă nu există evaluări
- The 10 Most Addictive Pain MedicationsDocument17 paginiThe 10 Most Addictive Pain MedicationslabendetÎncă nu există evaluări
- Write - Up - Adhoc Data SourcesDocument12 paginiWrite - Up - Adhoc Data SourcesRaju BaiÎncă nu există evaluări
- IV Drug CompDocument5 paginiIV Drug CompWil Lester100% (1)
- 3D Database SearchingDocument24 pagini3D Database SearchingSrigiriraju VedavyasÎncă nu există evaluări
- 050c2d93fc8616 - PMP Catalouge-Jan-2013 PDFDocument52 pagini050c2d93fc8616 - PMP Catalouge-Jan-2013 PDFUmaima faizÎncă nu există evaluări
- Module No. 2 Drug Dosage and CalculatioonsDocument7 paginiModule No. 2 Drug Dosage and CalculatioonsJellie An TalattagÎncă nu există evaluări
- MPharm Course Structure and Syllabus 11-8-2014Document101 paginiMPharm Course Structure and Syllabus 11-8-2014DongreSanjayÎncă nu există evaluări
- 10 Herbal Medicine-DohDocument5 pagini10 Herbal Medicine-DohJuna RoallosÎncă nu există evaluări
- The Structured Oral Examination in AnaesthesiaDocument287 paginiThe Structured Oral Examination in AnaesthesiaGerman Yakushkin100% (8)
- Patient Counseling-General Considerations, Important Steps & Procedures InvolvedDocument13 paginiPatient Counseling-General Considerations, Important Steps & Procedures InvolvedMD REFATÎncă nu există evaluări
- Extraction of Nutraceuticals From Plants - 14Document20 paginiExtraction of Nutraceuticals From Plants - 14Nikhil ChipadeÎncă nu există evaluări
- Phytochemistry and Pharmacological Activities of Clitoria TernateaDocument11 paginiPhytochemistry and Pharmacological Activities of Clitoria TernateaPaul Adrienne U. LaoÎncă nu există evaluări
- Advantages Disadvantages: Sedative Premedication Guidelines at RCHDocument3 paginiAdvantages Disadvantages: Sedative Premedication Guidelines at RCHdwÎncă nu există evaluări
- EntresToDocument17 paginiEntresToMorgan faresÎncă nu există evaluări
- ICH Quality Guidelines: An Implementation GuideDe la EverandICH Quality Guidelines: An Implementation GuideAndrew TeasdaleÎncă nu există evaluări
- Chemistry for Breakfast: The Amazing Science of Everyday LifeDe la EverandChemistry for Breakfast: The Amazing Science of Everyday LifeEvaluare: 4.5 din 5 stele4.5/5 (14)
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincDe la EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincEvaluare: 3.5 din 5 stele3.5/5 (137)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactDe la EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactEvaluare: 5 din 5 stele5/5 (5)
- Monkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeDe la EverandMonkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeEvaluare: 4 din 5 stele4/5 (1)
- The Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsDe la EverandThe Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsEvaluare: 5 din 5 stele5/5 (3)
- AP® Chemistry Crash Course, For the 2020 Exam, Book + Online: Get a Higher Score in Less TimeDe la EverandAP® Chemistry Crash Course, For the 2020 Exam, Book + Online: Get a Higher Score in Less TimeEvaluare: 5 din 5 stele5/5 (1)
- It's Elemental: The Hidden Chemistry in EverythingDe la EverandIt's Elemental: The Hidden Chemistry in EverythingEvaluare: 4 din 5 stele4/5 (10)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactDe la EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactEvaluare: 5 din 5 stele5/5 (1)
- Taste: Surprising Stories and Science About Why Food Tastes GoodDe la EverandTaste: Surprising Stories and Science About Why Food Tastes GoodEvaluare: 3 din 5 stele3/5 (20)
- AP Chemistry Flashcards, Fourth Edition: Up-to-Date Review and PracticeDe la EverandAP Chemistry Flashcards, Fourth Edition: Up-to-Date Review and PracticeÎncă nu există evaluări
- Handbook of Formulating Dermal Applications: A Definitive Practical GuideDe la EverandHandbook of Formulating Dermal Applications: A Definitive Practical GuideÎncă nu există evaluări
- Guidelines for Defining Process Safety Competency RequirementsDe la EverandGuidelines for Defining Process Safety Competency RequirementsEvaluare: 3 din 5 stele3/5 (1)
- The Periodic Table: A Very Short IntroductionDe la EverandThe Periodic Table: A Very Short IntroductionEvaluare: 4.5 din 5 stele4.5/5 (3)
- Chemistry for Breakfast: The Amazing Science of Everyday LifeDe la EverandChemistry for Breakfast: The Amazing Science of Everyday LifeEvaluare: 4.5 din 5 stele4.5/5 (90)
- The Production of Volatile Oils and Perfumery Plants in the United StatesDe la EverandThe Production of Volatile Oils and Perfumery Plants in the United StatesÎncă nu există evaluări
- Formulating, Packaging, and Marketing of Natural Cosmetic ProductsDe la EverandFormulating, Packaging, and Marketing of Natural Cosmetic ProductsÎncă nu există evaluări
- The Billion-Dollar Molecule: The Quest for the Perfect DrugDe la EverandThe Billion-Dollar Molecule: The Quest for the Perfect DrugEvaluare: 5 din 5 stele5/5 (2)
- Essential Chemistry for Formulators of Semisolid and Liquid DosagesDe la EverandEssential Chemistry for Formulators of Semisolid and Liquid DosagesEvaluare: 5 din 5 stele5/5 (2)
- Chemistry: a QuickStudy Laminated Reference GuideDe la EverandChemistry: a QuickStudy Laminated Reference GuideEvaluare: 5 din 5 stele5/5 (1)