S-ar putea să vă placă și
- Legal and Policy Perspectives on HIV and Human Rights in the CaribbeanDe la EverandLegal and Policy Perspectives on HIV and Human Rights in the CaribbeanÎncă nu există evaluări
- JC2750 SocialProtection enDocument32 paginiJC2750 SocialProtection enEneyew BirhanÎncă nu există evaluări
- Time Has Come For ABC Lancet2004Document3 paginiTime Has Come For ABC Lancet2004Constantino SantosÎncă nu există evaluări
- 4058 99135 MakurdiDocument111 pagini4058 99135 MakurdiSunkanmi FadojuÎncă nu există evaluări
- House of Pos InternationalDocument5 paginiHouse of Pos InternationalKENEDY FLORESÎncă nu există evaluări
- GESI - From NACO - CleanDocument35 paginiGESI - From NACO - CleanMatin Ahmad KhanÎncă nu există evaluări
- AIDS NB 2009 Annual ReportDocument12 paginiAIDS NB 2009 Annual ReportAIDSNBÎncă nu există evaluări
- Social Work Manifesto On HIV and AIDSDocument4 paginiSocial Work Manifesto On HIV and AIDSIonuț SîrbuÎncă nu există evaluări
- ICASO Annual Report 2000Document9 paginiICASO Annual Report 2000Kataisee RichardsonÎncă nu există evaluări
- Primary Care Guidance For Persons With Human Immunodeficiency Virus 2020 Update by The HIV Medicine Association of The Infectious Diseases Society of AmericaDocument33 paginiPrimary Care Guidance For Persons With Human Immunodeficiency Virus 2020 Update by The HIV Medicine Association of The Infectious Diseases Society of AmericaDiosvel José SarmientoÎncă nu există evaluări
- Preparedness, Prevention and Control of Coronavirus Disease (COVID-19) For Refugees and Migrants in Non-Camp SettingsDocument6 paginiPreparedness, Prevention and Control of Coronavirus Disease (COVID-19) For Refugees and Migrants in Non-Camp SettingsoscarÎncă nu există evaluări
- HIV This Week:: What Scientific Journals SaidDocument17 paginiHIV This Week:: What Scientific Journals SaidRizka AlnandaÎncă nu există evaluări
- India: National Youth Shadow ReportDocument24 paginiIndia: National Youth Shadow ReportBala KumaranÎncă nu există evaluări
- Civil Society and Communities Declaration To End HIV: Human Rights Must Come FirstDocument7 paginiCivil Society and Communities Declaration To End HIV: Human Rights Must Come FirsthousingworksÎncă nu există evaluări
- Civil Society's COVID-19 Calls To Action: PreambleDocument2 paginiCivil Society's COVID-19 Calls To Action: PreambleSyamsul PutraÎncă nu există evaluări
- PEPFAR SG Application 2017final3Document17 paginiPEPFAR SG Application 2017final3miadjafar463Încă nu există evaluări
- Nigeria: National Policy On HIV/AIDSDocument65 paginiNigeria: National Policy On HIV/AIDSState House NigeriaÎncă nu există evaluări
- Indigenous Peoples & The Covid-19 Pandemic: Considerations: Across International BordersDocument3 paginiIndigenous Peoples & The Covid-19 Pandemic: Considerations: Across International BordersRadhesh 2.OÎncă nu există evaluări
- 2015 InglésDocument124 pagini2015 InglésJuan Felipe RunzaÎncă nu există evaluări
- S.L. Aids PolicyDocument7 paginiS.L. Aids PolicyUmu NabieuÎncă nu există evaluări
- PPT1 HealthDocument52 paginiPPT1 HealthMa Angelica LocsinÎncă nu există evaluări
- Primary Health CareDocument5 paginiPrimary Health CareYashoda AmarasekeraÎncă nu există evaluări
- 2020 Community-Innovations enDocument32 pagini2020 Community-Innovations enpenaonparasÎncă nu există evaluări
- SCORA Manual PDFDocument8 paginiSCORA Manual PDFAmy WilsonÎncă nu există evaluări
- Summary For FABC VCC Task Force Workshop - PrintDocument6 paginiSummary For FABC VCC Task Force Workshop - PrintInes Oleaga CastelletÎncă nu există evaluări
- Declaration 2010Document2 paginiDeclaration 2010lanceinnesÎncă nu există evaluări
- Bns 209 Module 6 Prevention in Hiv and AidsDocument12 paginiBns 209 Module 6 Prevention in Hiv and AidslebogangÎncă nu există evaluări
- Llamado de Accin de MaliDocument2 paginiLlamado de Accin de MaliVictor Eduardo OchoaÎncă nu există evaluări
- Unaids: Saving Lives, Leaving No One BehindDocument4 paginiUnaids: Saving Lives, Leaving No One BehindTee Kok KeongÎncă nu există evaluări
- Position Paper IDocument1 paginăPosition Paper IIorgus-Serghei CicalaÎncă nu există evaluări
- A G P, P I P K P B F: Ssessment of Aps in Olicies Olicy Mplementation and Rograms For EY Opulations in Urkina ASODocument224 paginiA G P, P I P K P B F: Ssessment of Aps in Olicies Olicy Mplementation and Rograms For EY Opulations in Urkina ASOFuturesGroup1Încă nu există evaluări
- HIVAIDS Socio-Cultural PerspectiveDocument20 paginiHIVAIDS Socio-Cultural PerspectiveruffinanoellaanyangoÎncă nu există evaluări
- Demand Generation of COVID-19 VaccineDocument53 paginiDemand Generation of COVID-19 VaccineDesta DeressaÎncă nu există evaluări
- Community Health NursingDocument12 paginiCommunity Health NursingArra Mae EstabilloÎncă nu există evaluări
- The Paris Aids Declaration - enDocument3 paginiThe Paris Aids Declaration - enrauf_ayganÎncă nu există evaluări
- Abuja DeclarationDocument8 paginiAbuja DeclarationChikezie OnwukweÎncă nu există evaluări
- IqraDocument71 paginiIqraShenaya singhÎncă nu există evaluări
- DSWD Hiv Referral Book (1) Final and PublishedDocument98 paginiDSWD Hiv Referral Book (1) Final and PublishedRonz RoganÎncă nu există evaluări
- Batt Exam CHNDocument62 paginiBatt Exam CHNJoana Grace CortezÎncă nu există evaluări
- Part 1 (2291)Document20 paginiPart 1 (2291)Brian AdiemaÎncă nu există evaluări
- Role of NGOs in AIDS Control Programme DR Joseph P CarelDocument115 paginiRole of NGOs in AIDS Control Programme DR Joseph P CarelCarel Joseph0% (1)
- Aged Care Issues Raised by LGBTIQ and HIV+ People in The ACT (Screen Version)Document36 paginiAged Care Issues Raised by LGBTIQ and HIV+ People in The ACT (Screen Version)Harley DennettÎncă nu există evaluări
- HLST 354: Class 4 - Global HealthDocument29 paginiHLST 354: Class 4 - Global HealthLenard GpÎncă nu există evaluări
- Empathy, Dignity, and Respect: Creating Cultural Safety For Aboriginal People in Urban Health CareDocument78 paginiEmpathy, Dignity, and Respect: Creating Cultural Safety For Aboriginal People in Urban Health CareHealthCouncilCanadaÎncă nu există evaluări
- Summary of The President of The General Assembly On The Informal Interactive Civil Society HearingDocument9 paginiSummary of The President of The General Assembly On The Informal Interactive Civil Society HearingKataisee RichardsonÎncă nu există evaluări
- UNAIDS With Your Help enDocument16 paginiUNAIDS With Your Help enTee Kok KeongÎncă nu există evaluări
- BG Orientation 2022Document38 paginiBG Orientation 2022Kelvin ZhouÎncă nu există evaluări
- Pakistan: National Youth Shadow ReportDocument13 paginiPakistan: National Youth Shadow ReportjamshaidjiÎncă nu există evaluări
- Prepared By: Jessica D. Bentayen RN-MANDocument24 paginiPrepared By: Jessica D. Bentayen RN-MANNathaniel PulidoÎncă nu există evaluări
- CN Govt (1) .Document3 paginiCN Govt (1) .smurajasthan5038Încă nu există evaluări
- C Internationally, We Aim To Provide HIV Rapid Testing and Counseling To Rural Villagers inDocument5 paginiC Internationally, We Aim To Provide HIV Rapid Testing and Counseling To Rural Villagers inuaidinternationalÎncă nu există evaluări
- Concept of PHCDocument43 paginiConcept of PHCVantrigaru Veeresh Bangi93% (14)
- Breaking The BarriersDocument36 paginiBreaking The BarriersKaramchedu Vignani VijayagopalÎncă nu există evaluări
- Primary Health Care As An Approach To HealthDocument31 paginiPrimary Health Care As An Approach To HealthRea Andrea CuaresmaÎncă nu există evaluări
- Evaluation:: Basinang, Rica Kyrie T BSN 2 Community Health NursingDocument7 paginiEvaluation:: Basinang, Rica Kyrie T BSN 2 Community Health NursingloviÎncă nu există evaluări
- CASE STUDY A Scarcity of Life-Saving Resources During The COVID-19 PandemicDocument2 paginiCASE STUDY A Scarcity of Life-Saving Resources During The COVID-19 Pandemicmadiha fatimaÎncă nu există evaluări
- 1 - Q3 - Arts 10Document52 pagini1 - Q3 - Arts 10REGLOS, Marie Nhelle K.Încă nu există evaluări
- Hfa, PHC, MDG & SDGDocument13 paginiHfa, PHC, MDG & SDGUmme najiajahanÎncă nu există evaluări
- English Expository EssayDocument2 paginiEnglish Expository Essayjixie hwangÎncă nu există evaluări
- History of CBRDocument15 paginiHistory of CBRkim100% (3)
- Diabetexts Handout FlierDocument1 paginăDiabetexts Handout FlierMikhail MakÎncă nu există evaluări
- Open Education DiscDocument2 paginiOpen Education DiscMikhail MakÎncă nu există evaluări
- Two Spirit WomenDocument30 paginiTwo Spirit WomenMikhail Mak100% (1)
- OS in EducationDocument26 paginiOS in EducationMikhail MakÎncă nu există evaluări
- 2spirits Transgender Training ManualDocument32 pagini2spirits Transgender Training ManualMikhail MakÎncă nu există evaluări
- A History of Spirited PeopleDocument38 paginiA History of Spirited PeopleMikhail MakÎncă nu există evaluări
- First Nations Girls Health EducationDocument20 paginiFirst Nations Girls Health EducationMikhail MakÎncă nu există evaluări
- First Nations BoysDocument20 paginiFirst Nations BoysMikhail MakÎncă nu există evaluări
- The ELDER Project: Healthy Learning, Healthy LivingDocument18 paginiThe ELDER Project: Healthy Learning, Healthy LivingMikhail MakÎncă nu există evaluări
- Installing Edubuntu: ELDER ProjectDocument26 paginiInstalling Edubuntu: ELDER ProjectMikhail MakÎncă nu există evaluări
- Installing and Running QIMODocument27 paginiInstalling and Running QIMOMikhail MakÎncă nu există evaluări
- 8 Link Ers ContrastDocument2 pagini8 Link Ers ContrastGabitza GabyÎncă nu există evaluări
- Lesson PlanDocument5 paginiLesson PlanRedwan Siddik100% (2)
- COT RPMS Inter Observer Agreement Form For T I III For SY 2023 2024Document1 paginăCOT RPMS Inter Observer Agreement Form For T I III For SY 2023 2024alice mapanaoÎncă nu există evaluări
- Ferdinand LessonDocument2 paginiFerdinand Lessonapi-534190089Încă nu există evaluări
- 2ND Graduation Sppeech. Dean of Students. UmcDocument5 pagini2ND Graduation Sppeech. Dean of Students. Umcdereckstevens2015Încă nu există evaluări
- Study Material-INTRODUCTION TO FACILITATING LEARNER-CENTERED TEACHINGDocument2 paginiStudy Material-INTRODUCTION TO FACILITATING LEARNER-CENTERED TEACHINGJosette BonadorÎncă nu există evaluări
- Statement of PurposeDocument2 paginiStatement of PurposeMehedi HasanÎncă nu există evaluări
- Dayanand Sagar College of Engineering Bangalore - DSCE - MBADocument11 paginiDayanand Sagar College of Engineering Bangalore - DSCE - MBARakeshKumar1987Încă nu există evaluări
- Iis University JaipurDocument2 paginiIis University JaipurashleysharmaÎncă nu există evaluări
- Classroom Observation AssignmentDocument2 paginiClassroom Observation Assignmentapi-302422262Încă nu există evaluări
- Elc2012 PDFDocument2 paginiElc2012 PDFcÎncă nu există evaluări
- MINI MBA Brochure MIBDocument20 paginiMINI MBA Brochure MIBPranoj P FrancisÎncă nu există evaluări
- Instructional Design in Outcome Based EducationDocument44 paginiInstructional Design in Outcome Based EducationTherirose AnneÎncă nu există evaluări
- Lesson Plan Nimu Co 1 - 2021Document5 paginiLesson Plan Nimu Co 1 - 2021Jelly Marie Baya FloresÎncă nu există evaluări
- SaviasachiDocument1 paginăSaviasachiP.chandra Sekhar RajuÎncă nu există evaluări
- Mini Research - Esp Course Design - Group DDocument33 paginiMini Research - Esp Course Design - Group DPutri IlsaÎncă nu există evaluări
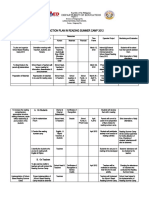
- An Action Plan in Reading Summer Camp 2012: Department of EducationDocument3 paginiAn Action Plan in Reading Summer Camp 2012: Department of EducationJESSICA MOSCARDON100% (1)
- SBE Assessment 3 2023 - 24-2 - 1715466357Document3 paginiSBE Assessment 3 2023 - 24-2 - 1715466357muhammad1970maqsoodÎncă nu există evaluări
- Grade 7 Daily Lesson Log School Grade Level 7 Teacher Learning Area MATHEMATICS Teaching Dates and Time Quarter FIRSTDocument2 paginiGrade 7 Daily Lesson Log School Grade Level 7 Teacher Learning Area MATHEMATICS Teaching Dates and Time Quarter FIRSTGerson Acosta100% (2)
- Norshamsiah Binti Harun: About MeDocument4 paginiNorshamsiah Binti Harun: About MeSYAFIQ BADANGÎncă nu există evaluări
- LCFDocument5 paginiLCFVashish RamrechaÎncă nu există evaluări
- The Muscular System Manual - E-Book: The Skeletal Muscles of The Human Body - Joseph E. MuscolinoDocument5 paginiThe Muscular System Manual - E-Book: The Skeletal Muscles of The Human Body - Joseph E. MuscolinonamurameÎncă nu există evaluări
- Leap 2025 Grade 6 Ela Practice Test Answer KeyDocument18 paginiLeap 2025 Grade 6 Ela Practice Test Answer KeyエゼイインムハンマドÎncă nu există evaluări
- E-Portfolio For Field Study 2Document9 paginiE-Portfolio For Field Study 2Darwin ValdezÎncă nu există evaluări
- Antony Partee Curriculum VitaeDocument5 paginiAntony Partee Curriculum Vitaeapi-290586785Încă nu există evaluări
- Thesis Topics Multimedia ArtsDocument5 paginiThesis Topics Multimedia Artsheatherricedesmoines100% (1)
- Theory Guide Simple Present Tense: NEGATIVE FORM:Subject + Auxiliary + Not + Verb (Base Form) +Document102 paginiTheory Guide Simple Present Tense: NEGATIVE FORM:Subject + Auxiliary + Not + Verb (Base Form) +Sheyla Castillo León100% (11)
- LS - Calendar 0809Document15 paginiLS - Calendar 0809sheenturtleÎncă nu există evaluări
- (360301354) OBE in Polytechnic EducationDocument39 pagini(360301354) OBE in Polytechnic EducationNoel KlÎncă nu există evaluări
- Semi-Detailed Lesson Plan in Mathematics 10 I. Learning Competency (MELC) With CodeDocument3 paginiSemi-Detailed Lesson Plan in Mathematics 10 I. Learning Competency (MELC) With Codecorrzz owthreeÎncă nu există evaluări