S-ar putea să vă placă și
- Badianus Manuscript An Aztec HerbalDocument12 paginiBadianus Manuscript An Aztec HerbalIgnacio Pamplona100% (1)
- Imhotep Books PDFDocument108 paginiImhotep Books PDFAndrew AdamsÎncă nu există evaluări
- Without Grain 100 Delicious Recipes For Eating A Grain-Free - Gluten-Free - Wheat-Free Diet PDFDocument211 paginiWithout Grain 100 Delicious Recipes For Eating A Grain-Free - Gluten-Free - Wheat-Free Diet PDFChuôngGió100% (1)
- Oral Physiology ReviewerDocument20 paginiOral Physiology ReviewerCamille Baybay100% (1)
- Department of Education: Republic of The PhilippinesDocument1 paginăDepartment of Education: Republic of The PhilippinesMary Grace R VillanuevaÎncă nu există evaluări
- Flag Ceremony (Mondays Only) /management of Learning (TWTHF)Document5 paginiFlag Ceremony (Mondays Only) /management of Learning (TWTHF)Jessa Mae Lig-angÎncă nu există evaluări
- Esp Inset Proposal 2023Document6 paginiEsp Inset Proposal 2023Renz PolicarpioÎncă nu există evaluări
- Restraint CompetencyDocument6 paginiRestraint CompetencyFrederick RyanÎncă nu există evaluări
- DLL Mapeh-6 Whole-YearDocument154 paginiDLL Mapeh-6 Whole-YearKristine Ann DadoleÎncă nu există evaluări
- Operator Manual AXIOM Artis: ListsDocument606 paginiOperator Manual AXIOM Artis: ListsHelen Cid Acevedo100% (2)
- RPMSDocument14 paginiRPMSMichael Louie IglesiasÎncă nu există evaluări
- Breastfeeding Policies: Martin Marasigan District HospitalDocument2 paginiBreastfeeding Policies: Martin Marasigan District Hospitalgrace dimangondayaoÎncă nu există evaluări
- FBS DLLDocument2 paginiFBS DLLDino PangilinanÎncă nu există evaluări
- ACTIVITY COMPLETION REPORT IN TLE June29-30Document11 paginiACTIVITY COMPLETION REPORT IN TLE June29-30Gil Bryan BalotÎncă nu există evaluări
- INDIVIDUAL DAILY LOG AND ACCOMPLISHMENT REPORT - MarielDocument3 paginiINDIVIDUAL DAILY LOG AND ACCOMPLISHMENT REPORT - MarielM3xobÎncă nu există evaluări
- P1 1-4Document1 paginăP1 1-4Bhem BoyÎncă nu există evaluări
- SBFP Accomplishment Sy2021-2022 Batch 2Document28 paginiSBFP Accomplishment Sy2021-2022 Batch 2viviane abrigo100% (1)
- Department of Education: Republic of The PhilippinesDocument18 paginiDepartment of Education: Republic of The PhilippinesAaron David SubaÎncă nu există evaluări
- Consolidated Nutritional Status2019Document1 paginăConsolidated Nutritional Status2019ZailiYaunÎncă nu există evaluări
- DLL TemplateDocument2 paginiDLL TemplateAlvin CaloraÎncă nu există evaluări
- Col. Patrocinio Artuz National High School: Division of Capiz Brgy. Taft, Tapaz, CapizDocument5 paginiCol. Patrocinio Artuz National High School: Division of Capiz Brgy. Taft, Tapaz, CapizPaul Senen DiduloÎncă nu există evaluări
- San Isidro Schoolcanteen-Report-Sy-2022-2023Document9 paginiSan Isidro Schoolcanteen-Report-Sy-2022-2023Leila R. RecanaÎncă nu există evaluări
- SBFP 2018-2019Document3 paginiSBFP 2018-2019Lea CardinezÎncă nu există evaluări
- Action PlanDocument1 paginăAction PlanMilagrosa Fiel D. IncisoÎncă nu există evaluări
- Iv. Management of Resources: Fortunato F. Halili National Agricultural School Magasawang-Sapa AnnexDocument19 paginiIv. Management of Resources: Fortunato F. Halili National Agricultural School Magasawang-Sapa AnnexJerome Manabat100% (1)
- LE Cookery 9 Q4W7Document4 paginiLE Cookery 9 Q4W7Jenny Rose Mojica Betsayda100% (1)
- RPMS Tool For Master Teachers I-IV (Highly Proficient Teachers) in The Time of COVID-19 S.Y. 2020-2021Document19 paginiRPMS Tool For Master Teachers I-IV (Highly Proficient Teachers) in The Time of COVID-19 S.Y. 2020-2021AMADO JR BANAWAÎncă nu există evaluări
- TLE Department Action Plan 2016 2017Document8 paginiTLE Department Action Plan 2016 2017Shiela Marie Galo Sanico-DespoyÎncă nu există evaluări
- Training Proposal - Revised (AutoRecovered)Document5 paginiTraining Proposal - Revised (AutoRecovered)Emil OcierÎncă nu există evaluări
- Challenges Met On SBM ImplementationDocument3 paginiChallenges Met On SBM ImplementationStephen John Palomaria100% (1)
- Tip Course 3 Answer Key - Compress PDFDocument18 paginiTip Course 3 Answer Key - Compress PDFGil B. MillendezÎncă nu există evaluări
- Re-Entry Action Plan (REAP)Document3 paginiRe-Entry Action Plan (REAP)Ricardo TambogonÎncă nu există evaluări
- Request-for-Correction-Forms-Released - (RF13) SMNHSDocument30 paginiRequest-for-Correction-Forms-Released - (RF13) SMNHSJapeth PurisimaÎncă nu există evaluări
- 2022-2023 Action PlanDocument6 pagini2022-2023 Action PlanMay-ann Ramos Galliguez ValdezÎncă nu există evaluări
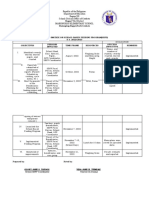
- Projects/ Programs Targets Strategies Time Frame Funding Sources Persons Involve Expected OutcomesDocument3 paginiProjects/ Programs Targets Strategies Time Frame Funding Sources Persons Involve Expected OutcomesFlorame OñateÎncă nu există evaluări
- Appendix B2: Screening Test Class Reading Record (STCRR)Document1 paginăAppendix B2: Screening Test Class Reading Record (STCRR)Janine ArmamentoÎncă nu există evaluări
- DLL - Cooperative Learning ApproachDocument5 paginiDLL - Cooperative Learning ApproachAndrea Dapiton OrillanedaÎncă nu există evaluări
- Project Design 555 FinalDocument6 paginiProject Design 555 FinalHaydee BELGICAÎncă nu există evaluări
- Tle 9 March 8 - 13, 2020Document5 paginiTle 9 March 8 - 13, 2020Charmain J. DequitoÎncă nu există evaluări
- Action Plan For School Year 2018-2019 Expected Outcomes Time Frame Success Indicator Quantity Quality A. Pupil DevelopmentDocument3 paginiAction Plan For School Year 2018-2019 Expected Outcomes Time Frame Success Indicator Quantity Quality A. Pupil DevelopmentMylene P Tiburcio-SantiagoÎncă nu există evaluări
- 2017 Project Activity Design & Report FormDocument3 pagini2017 Project Activity Design & Report FormClerica Realingo100% (1)
- Module-4 Lesson2 Activity1Document2 paginiModule-4 Lesson2 Activity1Norvel BucaoÎncă nu există evaluări
- Department of Education: Republic of The PhilippinesDocument2 paginiDepartment of Education: Republic of The PhilippinesMedalla MocorroÎncă nu există evaluări
- Literacy Numeracy Quarter Monitoring ToolDocument1 paginăLiteracy Numeracy Quarter Monitoring ToolJennifer Albarado100% (1)
- (Full-Time Teacher-Broadcasters) (Full-Time Teacher-Broadcasters) (Full-Time Teacher-Broadcasters)Document1 pagină(Full-Time Teacher-Broadcasters) (Full-Time Teacher-Broadcasters) (Full-Time Teacher-Broadcasters)Gypsie Ann PaconÎncă nu există evaluări
- Cot - LP 2Document7 paginiCot - LP 2Sheila Abbu ComonsadÎncă nu există evaluări
- Activity Completion Report: Accomplished Enhanced School Improvement Plan (ESIP) S.Y 2019-2020Document15 paginiActivity Completion Report: Accomplished Enhanced School Improvement Plan (ESIP) S.Y 2019-2020Cristina SarmientoÎncă nu există evaluări
- S.Y. 2017-2018 Bocaue District Project An Pretest ResultsDocument18 paginiS.Y. 2017-2018 Bocaue District Project An Pretest Resultsvincevillamora2k11Încă nu există evaluări
- WLAS Activity Plan and Accomplishment ReportDocument2 paginiWLAS Activity Plan and Accomplishment Reportmaricel sulapasÎncă nu există evaluări
- Project Title Pagkain Mo, Sagot Ko para Sa Tuloy-Tuloy Na Pag-Unlad Mo Program Problem StatementDocument4 paginiProject Title Pagkain Mo, Sagot Ko para Sa Tuloy-Tuloy Na Pag-Unlad Mo Program Problem StatementGe LoÎncă nu există evaluări
- SF-10b-comDocument7 paginiSF-10b-comRoSs Adrales ArelegÎncă nu există evaluări
- Localized Module in Promoting Philippine-Hilot in Teaching Wellness Massage and The Student's Performance in Tle 10: Input To New Delivery Modes of InstructionDocument12 paginiLocalized Module in Promoting Philippine-Hilot in Teaching Wellness Massage and The Student's Performance in Tle 10: Input To New Delivery Modes of InstructionIOER International Multidisciplinary Research Journal ( IIMRJ)Încă nu există evaluări
- PAR Form 2019 and OnDocument1 paginăPAR Form 2019 and OnRiza Garganza100% (5)
- Feeding MatrixDocument2 paginiFeeding MatrixJane TapgosÎncă nu există evaluări
- Grade 6 ExemplarDocument8 paginiGrade 6 ExemplarLulu Belle B. PadriqueÎncă nu există evaluări
- Home Visitation Form 2022 2023Document1 paginăHome Visitation Form 2022 2023JaneÎncă nu există evaluări
- Libre Bulad Action Plan 2019 2020Document5 paginiLibre Bulad Action Plan 2019 2020Jeffreynald Francisco100% (1)
- Lesson Plan in TLE (Process Based Learning) FinalDocument4 paginiLesson Plan in TLE (Process Based Learning) Finalapril impsÎncă nu există evaluări
- Q2 - (LAS) O.M WK 6Document6 paginiQ2 - (LAS) O.M WK 6Jazer LeuterioÎncă nu există evaluări
- PART-IV DP - FinalDocument1 paginăPART-IV DP - FinalAlz Bakino LptÎncă nu există evaluări
- PARENT Teacher Conference ToolDocument3 paginiPARENT Teacher Conference ToolJHODIE LYNNE OLAERÎncă nu există evaluări
- Deworming TemplateDocument2 paginiDeworming TemplateHaidee Huerta-SalubreÎncă nu există evaluări
- School Monitoring Evaluation and Adjustment: Calendar Year 2021 Quarter 1Document39 paginiSchool Monitoring Evaluation and Adjustment: Calendar Year 2021 Quarter 1Reynalyn SuangcoÎncă nu există evaluări
- SUGGESTED ARTIFACTS SBMDocument28 paginiSUGGESTED ARTIFACTS SBMDoc BesterÎncă nu există evaluări
- Malapad Na Parang Es-Deworming-Form - 2021Document5 paginiMalapad Na Parang Es-Deworming-Form - 2021Bernice OrtegaÎncă nu există evaluări
- Magnesium ReplacementDocument4 paginiMagnesium ReplacementArvenaa SubramaniamÎncă nu există evaluări
- Grass Jelly On Glycemic ControlDocument11 paginiGrass Jelly On Glycemic ControlAnanta ArioÎncă nu există evaluări
- Open Bite: A Review of Etiology and Management: Peter Ngan, DMD Henry W. Fields, DDS, MS, MSDDocument8 paginiOpen Bite: A Review of Etiology and Management: Peter Ngan, DMD Henry W. Fields, DDS, MS, MSDAzi Pertiwi HussainÎncă nu există evaluări
- BLUE Protocol 2Document1 paginăBLUE Protocol 2Syed Shahrul Naz SyedÎncă nu există evaluări
- NUR1213L May2013 FinalDocument23 paginiNUR1213L May2013 FinalOzzy Viadnes MalanaÎncă nu există evaluări
- A Know LodgementDocument1 paginăA Know LodgementMahmmoud EltaweelÎncă nu există evaluări
- NIH Public Access: The Pathogenesis of Systemic Lupus Erythematosus - An UpdateDocument12 paginiNIH Public Access: The Pathogenesis of Systemic Lupus Erythematosus - An UpdateYessicaMariñosKirosÎncă nu există evaluări
- Q 7Document21 paginiQ 7Buii AhÎncă nu există evaluări
- Bai Tap Ve Chia Thi Tieng Anh Nang CaoDocument3 paginiBai Tap Ve Chia Thi Tieng Anh Nang CaoTai NguyễnÎncă nu există evaluări
- NHIS Variable SummaryDocument4 paginiNHIS Variable SummaryJin SiclonÎncă nu există evaluări
- Aditya MotwaneDocument3 paginiAditya Motwaneapi-257938623Încă nu există evaluări
- Scapular Dyskinesis Increases The Risk of Future Shoulder Pain by 43% in Asymptomatic Athletes A Systematic Reviwer Nad Meta AnalysisDocument11 paginiScapular Dyskinesis Increases The Risk of Future Shoulder Pain by 43% in Asymptomatic Athletes A Systematic Reviwer Nad Meta AnalysisCesar C SÎncă nu există evaluări
- High Risk PregnanciesDocument27 paginiHigh Risk PregnanciesMochammad Adam EldiÎncă nu există evaluări
- Costeo Basado en ActividadesDocument11 paginiCosteo Basado en Actividadesfrank richard lopez salinasÎncă nu există evaluări
- SAQ123 NursesUserGuide V6Document30 paginiSAQ123 NursesUserGuide V6LisaBrook100% (1)
- Ich GCP: HistoryDocument57 paginiIch GCP: HistoryChandrashekhar Singh100% (1)
- Merger Value CreationDocument11 paginiMerger Value CreationAziz BouignaneÎncă nu există evaluări
- Intensive Revision Course in Paediatrics (Poster)Document2 paginiIntensive Revision Course in Paediatrics (Poster)Chris Jardine LiÎncă nu există evaluări
- Homeo MedicinesDocument31 paginiHomeo MedicinesSaleem RazaÎncă nu există evaluări
- 6 DOH Sample FormsDocument136 pagini6 DOH Sample FormsSir Cris CapiliÎncă nu există evaluări
- Vietnam Vets and Delayed Expression PTSD - WorddocDocument5 paginiVietnam Vets and Delayed Expression PTSD - Worddocjim912Încă nu există evaluări
- The Platyhelminthes (Flatworms) : Flukes: - Trematodes Are Parasites of Vertebrates. They HaveDocument29 paginiThe Platyhelminthes (Flatworms) : Flukes: - Trematodes Are Parasites of Vertebrates. They HaveRiya KayarkarÎncă nu există evaluări
- Biosecurity Challenges of The Global Expansion of High-Containment Biological LaboratoriesDocument217 paginiBiosecurity Challenges of The Global Expansion of High-Containment Biological LaboratoriesIhor KuzinÎncă nu există evaluări