S-ar putea să vă placă și
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDe la EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesEvaluare: 4 din 5 stele4/5 (2)
- Hypoglycemic Encephalopathy A Case Series and Literature Review On Outcome DeterminationDocument7 paginiHypoglycemic Encephalopathy A Case Series and Literature Review On Outcome Determinationc5qdk8jnÎncă nu există evaluări
- Complementary and Alternative Medical Lab Testing Part 12: NeurologyDe la EverandComplementary and Alternative Medical Lab Testing Part 12: NeurologyÎncă nu există evaluări
- Poststroke Hyperglycemia: Natural History and Immediate ManagementDocument5 paginiPoststroke Hyperglycemia: Natural History and Immediate ManagementEsteban Martin Chiotti KaneshimaÎncă nu există evaluări
- Emergencies in Diabetes: Diagnosis, Management and PreventionDe la EverandEmergencies in Diabetes: Diagnosis, Management and PreventionÎncă nu există evaluări
- Assessment and Treatment of Hyperglycemia in Critically IllDocument6 paginiAssessment and Treatment of Hyperglycemia in Critically IllYousif ElmasryÎncă nu există evaluări
- Clinical Presentation and Diagnostic Approach To Hypoglycemia inDocument9 paginiClinical Presentation and Diagnostic Approach To Hypoglycemia inRichard Loor RomeroÎncă nu există evaluări
- 7 UJP 15468 (RV)Document6 pagini7 UJP 15468 (RV)sohailsuÎncă nu există evaluări
- Suspected Postprandial Hypoglycemia Is Associated With ,&adrenergic Hypersensitivity and Emotional DistressDocument6 paginiSuspected Postprandial Hypoglycemia Is Associated With ,&adrenergic Hypersensitivity and Emotional Distresslasith123Încă nu există evaluări
- HipoglikemiaDocument7 paginiHipoglikemiakarisaÎncă nu există evaluări
- Case Study Seizure ControlDocument16 paginiCase Study Seizure ControlCitra KristiÎncă nu există evaluări
- Er 2018-00226Document21 paginiEr 2018-00226Aldo Amed Montaño SalinasÎncă nu există evaluări
- Desantis 2006Document15 paginiDesantis 2006Hoàng ThôngÎncă nu există evaluări
- Content ServerDocument9 paginiContent ServerNourma Kusuma WinawanÎncă nu există evaluări
- Hypoglycemia in Critically Ill Children: J Diabetes Sci TechnolDocument21 paginiHypoglycemia in Critically Ill Children: J Diabetes Sci TechnolSuryadi Soekiman RazakÎncă nu există evaluări
- Hypoglycemia in Adults Without Diabetes Mellitus - Clinical Manifestations, Causes, and DiagnosisDocument25 paginiHypoglycemia in Adults Without Diabetes Mellitus - Clinical Manifestations, Causes, and Diagnosismayteveronica1000Încă nu există evaluări
- Stress Response in Critical Illness: Laura Santos, MDDocument9 paginiStress Response in Critical Illness: Laura Santos, MDPutri Wulan SukmawatiÎncă nu există evaluări
- Jcem 0709Document20 paginiJcem 0709Rao Rizwan ShakoorÎncă nu există evaluări
- Hypo Glice MiaDocument14 paginiHypo Glice MiaCarlos SandovalÎncă nu există evaluări
- Congenital Hyperinsulinism Current Trends in Diagnosis and TheraphyDocument14 paginiCongenital Hyperinsulinism Current Trends in Diagnosis and TheraphyJaka KurniawanÎncă nu există evaluări
- Journal Pone 0059672Document8 paginiJournal Pone 0059672mcgilicuttyÎncă nu există evaluări
- Case StudyDocument3 paginiCase StudyAnnie Laiza BacayÎncă nu există evaluări
- Tight GlycemicDocument10 paginiTight GlycemicIsmail Mohammed AbdelgawadÎncă nu există evaluări
- HypoglicemicDocument20 paginiHypoglicemicAndreea CreangaÎncă nu există evaluări
- Symptoms of HypoglycemiaDocument20 paginiSymptoms of Hypoglycemiakenny StefÎncă nu există evaluări
- HOMA-IR Values Are Associated With Glycemic Control in Japanese Subjects Without Diabetes or Obesity: The KOBE StudyDocument8 paginiHOMA-IR Values Are Associated With Glycemic Control in Japanese Subjects Without Diabetes or Obesity: The KOBE StudyNur Ahmad HabibiÎncă nu există evaluări
- Hypoglycemia in Patients With Insulin Treated Diabetes: Review ArticleDocument9 paginiHypoglycemia in Patients With Insulin Treated Diabetes: Review ArticleEmanuel BaltigÎncă nu există evaluări
- Association Between Early Glycemic Control and Improvements In. 2014Document6 paginiAssociation Between Early Glycemic Control and Improvements In. 2014ARELHI ROSARIO GARCIA MONROYÎncă nu există evaluări
- Hypoglycemia in Critically Ill ChildrenDocument10 paginiHypoglycemia in Critically Ill ChildrenCiendy ShintyaÎncă nu există evaluări
- Hamsini SreeramDocument33 paginiHamsini SreeramkalyanpavuralaÎncă nu există evaluări
- Journal of The Neurological SciencesDocument3 paginiJournal of The Neurological SciencesAdrian KhomanÎncă nu există evaluări
- Edwards AbstractDocument3 paginiEdwards Abstracteen265Încă nu există evaluări
- Jurnal Hipoglikemik NeonatusDocument25 paginiJurnal Hipoglikemik NeonatusJosephine Ria PitasariÎncă nu există evaluări
- Minimizing Hypoglycemia in Diabetes: International Hypoglycaemia Study GroupDocument9 paginiMinimizing Hypoglycemia in Diabetes: International Hypoglycaemia Study GroupNovianDwiRoessantiÎncă nu există evaluări
- Jurnal KDMDocument8 paginiJurnal KDMFhietry Idrus ScaftweeÎncă nu există evaluări
- Persistent HypoglycemiaDocument47 paginiPersistent Hypoglycemiapriyanshu mathurÎncă nu există evaluări
- Jurnal Hipoglikemia PDFDocument8 paginiJurnal Hipoglikemia PDFAyu Aprilita BastariÎncă nu există evaluări
- Danilo F. Baldemor, MD, MS, DPCP: Internist - DiabetetologistDocument93 paginiDanilo F. Baldemor, MD, MS, DPCP: Internist - DiabetetologistButch AmbataliÎncă nu există evaluări
- Morales2014 PDFDocument8 paginiMorales2014 PDFIneke IntaniaÎncă nu există evaluări
- Referat 8Document6 paginiReferat 8Sultan Rahmat SeptianÎncă nu există evaluări
- Mahajan 2017Document25 paginiMahajan 2017Farin MauliaÎncă nu există evaluări
- Hyperglycemia and Neurological Outcome in Patients With Head InjuryDocument7 paginiHyperglycemia and Neurological Outcome in Patients With Head InjuryOsQ_drÎncă nu există evaluări
- Hypoglycaemia Unawareness: JP Vignesh, V MohanDocument6 paginiHypoglycaemia Unawareness: JP Vignesh, V MohanFaizudin HafifiÎncă nu există evaluări
- A Nutraceutical Combination Improves Insulin Sensitivity in Patients With Metabolic SyndromeDocument7 paginiA Nutraceutical Combination Improves Insulin Sensitivity in Patients With Metabolic SyndromegiannidietÎncă nu există evaluări
- Jurnal HipoglikemiaDocument5 paginiJurnal HipoglikemiaIndra Budi PutraÎncă nu există evaluări
- Hyperglycemia After Cardiac Surgery - Hebson2013Document6 paginiHyperglycemia After Cardiac Surgery - Hebson2013Dr XÎncă nu există evaluări
- Acromegalie Cu GH Aparent in NormaDocument6 paginiAcromegalie Cu GH Aparent in NormaOlesea DorogonceanÎncă nu există evaluări
- Diabetes Case StudyDocument6 paginiDiabetes Case StudyDavid DeegbeÎncă nu există evaluări
- Vlasselaers 2009Document10 paginiVlasselaers 2009Dr XÎncă nu există evaluări
- Management of Neonatal HypoglycemiaDocument14 paginiManagement of Neonatal Hypoglycemiaece142Încă nu există evaluări
- Original Article: Endothelial Glycocalyx Damage Coincides With Microalbuminuria in Type 1 DiabetesDocument6 paginiOriginal Article: Endothelial Glycocalyx Damage Coincides With Microalbuminuria in Type 1 DiabetesPandji 'Utuh'Încă nu există evaluări
- A Prospective Evaluation of Microvascular ComplicaDocument5 paginiA Prospective Evaluation of Microvascular ComplicaBeatrizÎncă nu există evaluări
- HypoglycaemiaDocument3 paginiHypoglycaemiaAneejaa BidhaÎncă nu există evaluări
- Empagliflozin Monotherapy in Japanese Patients With Type 2 Diabetes Mellitus: A Randomized, 12-Week, Double-Blind, Placebo-Controlled, Phase II TrialDocument18 paginiEmpagliflozin Monotherapy in Japanese Patients With Type 2 Diabetes Mellitus: A Randomized, 12-Week, Double-Blind, Placebo-Controlled, Phase II TrialKeenan JaquesÎncă nu există evaluări
- Approach To Hypoglycemia in Infants and Children - UpToDateDocument31 paginiApproach To Hypoglycemia in Infants and Children - UpToDateyohanes gabriel dwirianto w.aÎncă nu există evaluări
- AACE Clinical Case ReportsDocument3 paginiAACE Clinical Case ReportsSameerÎncă nu există evaluări
- Frequency and Predictors of Hypoglycemia in Type 2.9Document7 paginiFrequency and Predictors of Hypoglycemia in Type 2.9Doménica JayaÎncă nu există evaluări
- Hyperglycemia Has A Stronger Relation With Outcome in Trauma Patients Than in Other Critically Ill PatientsDocument12 paginiHyperglycemia Has A Stronger Relation With Outcome in Trauma Patients Than in Other Critically Ill PatientsAfkar30Încă nu există evaluări
- Derosa 2010 InfDocument5 paginiDerosa 2010 InfJuan Carlos FloresÎncă nu există evaluări
- Hypoglycemia - The Neglected ComplicationDocument23 paginiHypoglycemia - The Neglected Complication4g5xwdvh9sÎncă nu există evaluări
- Singularity Point Part Two - Nebulae of HopesDocument35 paginiSingularity Point Part Two - Nebulae of HopesJennifer JaneÎncă nu există evaluări
- Rutherford Vascular Surgery 6th Edition Elsevier SDocument2 paginiRutherford Vascular Surgery 6th Edition Elsevier SJennifer Jane0% (1)
- Trombocitopenia PDFDocument11 paginiTrombocitopenia PDFbrigde_xÎncă nu există evaluări
- 2 PBDocument5 pagini2 PBvita famia sariÎncă nu există evaluări
- Counting Sheep: A Rational Approach To Managing Insomnia (TH305)Document1 paginăCounting Sheep: A Rational Approach To Managing Insomnia (TH305)Jennifer JaneÎncă nu există evaluări
- 4Document5 pagini4Razwa MaghviraÎncă nu există evaluări
- Rasburicase (Elitek) : A Novel Agent For Tumor Lysis SyndromeDocument5 paginiRasburicase (Elitek) : A Novel Agent For Tumor Lysis SyndromeJennifer JaneÎncă nu există evaluări
- Approach To The Adult Patient With Fever of Unknown OriginDocument6 paginiApproach To The Adult Patient With Fever of Unknown Origini can always make u smile :D100% (1)
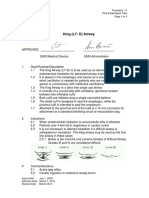
- Ems Proc 17 King Airway 3-29-2012Document4 paginiEms Proc 17 King Airway 3-29-2012Jennifer JaneÎncă nu există evaluări
- Coronavirus Infections-More Than Just The Common ColdDocument2 paginiCoronavirus Infections-More Than Just The Common ColdLuis Miguel Ruiz VÎncă nu există evaluări
- The Effects of Corticosteroids and Nonsteroidal Anti-Inflammatory Drugs, Including Aspirin, On CoagulationDocument3 paginiThe Effects of Corticosteroids and Nonsteroidal Anti-Inflammatory Drugs, Including Aspirin, On CoagulationmelvinÎncă nu există evaluări
- Focus Group AnalysisDocument1 paginăFocus Group AnalysisFarasila RashofaÎncă nu există evaluări
- Prepscholar Head To ToeDocument2 paginiPrepscholar Head To ToeJennifer JaneÎncă nu există evaluări
- Free Crochet Pattern "Little Monkey": Hi There! I Invite You To Crochet Little Monkeys Like This One With MeDocument7 paginiFree Crochet Pattern "Little Monkey": Hi There! I Invite You To Crochet Little Monkeys Like This One With MeJennifer JaneÎncă nu există evaluări
- Meletis Editoril Supl 12015Document6 paginiMeletis Editoril Supl 12015Jennifer JaneÎncă nu există evaluări
- 2 PBDocument5 pagini2 PBvita famia sariÎncă nu există evaluări
- Coronavirus Infections-More Than Just The Common ColdDocument2 paginiCoronavirus Infections-More Than Just The Common ColdLuis Miguel Ruiz VÎncă nu există evaluări
- Burns Management PDFDocument7 paginiBurns Management PDFRoh Bungaria N Garingging100% (1)
- Corynebacterium Minutissimum: Bacteremia in An Immunocompetent Host With CellulitisDocument3 paginiCorynebacterium Minutissimum: Bacteremia in An Immunocompetent Host With CellulitisJennifer JaneÎncă nu există evaluări
- Dexmedetomidine Use in General Anaesthesia: A. Arcangeli, C. D'Alò and R. GaspariDocument9 paginiDexmedetomidine Use in General Anaesthesia: A. Arcangeli, C. D'Alò and R. GaspariJennifer JaneÎncă nu există evaluări
- Clinical Picture: Secondary Hemorrhage in Traumatic HyphemaDocument1 paginăClinical Picture: Secondary Hemorrhage in Traumatic HyphemaJennifer JaneÎncă nu există evaluări
- Mask Strap Ear Saver PatternDocument3 paginiMask Strap Ear Saver PatternJennifer JaneÎncă nu există evaluări
- Traumatic Hyphema in Benin City, Nigeria: Original ArticleDocument4 paginiTraumatic Hyphema in Benin City, Nigeria: Original ArticleJennifer JaneÎncă nu există evaluări
- The Prevalence of Interdigital Erythrasma in Southern Region of TurkeyDocument5 paginiThe Prevalence of Interdigital Erythrasma in Southern Region of TurkeyJennifer JaneÎncă nu există evaluări
- 12512-Article Text-43579-1-10-20150503 PDFDocument4 pagini12512-Article Text-43579-1-10-20150503 PDFJennifer JaneÎncă nu există evaluări
- Prog Lin2018Document4 paginiProg Lin2018Jennifer JaneÎncă nu există evaluări
- ModuleIV RespiratoryEmergencies CHF COPD AsthmaDocument96 paginiModuleIV RespiratoryEmergencies CHF COPD AsthmaSaiKiranÎncă nu există evaluări
- ModuleIV RespiratoryEmergencies CHF COPD AsthmaDocument96 paginiModuleIV RespiratoryEmergencies CHF COPD AsthmaSaiKiranÎncă nu există evaluări
- 2015 Article 1418 PDFDocument5 pagini2015 Article 1418 PDFJennifer JaneÎncă nu există evaluări
- Guideline: Dumonceau Jean-Marc Et Al. Indications, Results, and EndosDocument22 paginiGuideline: Dumonceau Jean-Marc Et Al. Indications, Results, and EndosJennifer JaneÎncă nu există evaluări
- Ludwig Heinrich Bojanus (1776-1827) On Gall's Craniognomic System, Zoology - UnlockedDocument20 paginiLudwig Heinrich Bojanus (1776-1827) On Gall's Craniognomic System, Zoology - UnlockedJaime JaimexÎncă nu există evaluări
- Meisi Arisandi - Resume Jurnal Internasional Dan Nasional Keperawatan JiwaDocument6 paginiMeisi Arisandi - Resume Jurnal Internasional Dan Nasional Keperawatan JiwawendihiÎncă nu există evaluări
- Orbino, Frances Anne N. 4th Rot FdarDocument2 paginiOrbino, Frances Anne N. 4th Rot FdarFrances OrbinoÎncă nu există evaluări
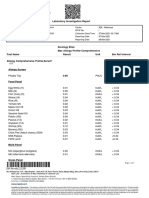
- Laboratory Investigation ReportDocument7 paginiLaboratory Investigation ReportAmarjeetÎncă nu există evaluări
- CONJUNCTIVITIS or Pink Eye, Emotional and Spiritual MeaningDocument1 paginăCONJUNCTIVITIS or Pink Eye, Emotional and Spiritual MeaningSarah g.Încă nu există evaluări
- Virology DatabaseDocument56 paginiVirology DatabaseAhraÎncă nu există evaluări
- Module 10Document5 paginiModule 10Yuki Xairah TunayÎncă nu există evaluări
- Prosthetic Case PresentationsDocument19 paginiProsthetic Case PresentationsptannenbaumÎncă nu există evaluări
- Fulmer SPICES: An Overall Assessment Tool For Older AdultsDocument2 paginiFulmer SPICES: An Overall Assessment Tool For Older AdultsSteve GarrettÎncă nu există evaluări
- 307-Article Text-578-1-10-20210309 PDFDocument13 pagini307-Article Text-578-1-10-20210309 PDFPUTRI LISTIANIÎncă nu există evaluări
- Physics With Illustrative Examples From Medicine and BiologyDocument1 paginăPhysics With Illustrative Examples From Medicine and BiologySivaranjaniÎncă nu există evaluări
- Optic Nerve Glioma: Case Series With Review of Clinical, Radiologic, Molecular, and Histopathologic CharacteristicsDocument5 paginiOptic Nerve Glioma: Case Series With Review of Clinical, Radiologic, Molecular, and Histopathologic CharacteristicsUtama Hadiputra SurbaktiÎncă nu există evaluări
- Stylohyoid LigamentDocument4 paginiStylohyoid LigamentArindom ChangmaiÎncă nu există evaluări
- Hospitalization and Its Effect For Patient - UNTAD 2011 PDFDocument26 paginiHospitalization and Its Effect For Patient - UNTAD 2011 PDFRiris SutrisnoÎncă nu există evaluări
- Health Checklist: NG:) Lumunok)Document2 paginiHealth Checklist: NG:) Lumunok)Rose Duron GumaÎncă nu există evaluări
- 1st Floor No 105 Above Raymonds Opp Medical College Koti: SHARMA Bpo SupportDocument4 pagini1st Floor No 105 Above Raymonds Opp Medical College Koti: SHARMA Bpo SupportMK Musthafa GudalurÎncă nu există evaluări
- A Detailed Lesson Plan in Living ThingsDocument23 paginiA Detailed Lesson Plan in Living ThingsclarisseÎncă nu există evaluări
- All India Hospital ListDocument303 paginiAll India Hospital ListwittyadityaÎncă nu există evaluări
- Bisphosphonate Treatment Break Guidance June 2017Document2 paginiBisphosphonate Treatment Break Guidance June 2017Usman Zafar QaziÎncă nu există evaluări
- Sedation Under JCI StandardDocument36 paginiSedation Under JCI Standardกิ๊กกิ๊ก ค่าาาาÎncă nu există evaluări
- Piis1036731421001144 PDFDocument7 paginiPiis1036731421001144 PDFvaloranthakam10Încă nu există evaluări
- European University of Lefke: Eczacılık Fakültesi / Faculty of PharmacyDocument3 paginiEuropean University of Lefke: Eczacılık Fakültesi / Faculty of PharmacyMariem Ben HediaÎncă nu există evaluări
- Neri, Angela - Act. 1,2,3Document5 paginiNeri, Angela - Act. 1,2,3Angela NeriÎncă nu există evaluări
- Question 1Document87 paginiQuestion 1hemihemaÎncă nu există evaluări
- Down Screen Proposal For Health Screen at Thyrocare AmitDocument19 paginiDown Screen Proposal For Health Screen at Thyrocare AmitSwatiSuranaÎncă nu există evaluări
- Mixed Lymphocyte Culture / Reaction (MLC / MLR)Document2 paginiMixed Lymphocyte Culture / Reaction (MLC / MLR)Muthi KhairunnisaÎncă nu există evaluări
- Epidemiology of Infectious DiseasesDocument69 paginiEpidemiology of Infectious Diseasesmus zaharaÎncă nu există evaluări
- Special Round Seats For MD - MS - Diploma & DNB SeatsDocument23 paginiSpecial Round Seats For MD - MS - Diploma & DNB SeatsManoj KashyapÎncă nu există evaluări
- LewisDocument12 paginiLewisLewis Nimsy Tunde100% (1)
- The Andrea Bocelli ConcertDocument2 paginiThe Andrea Bocelli Concertgastoast5Încă nu există evaluări