S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Skin and MSK EverythingDocument31 paginiSkin and MSK EverythingBernard HernandezÎncă nu există evaluări
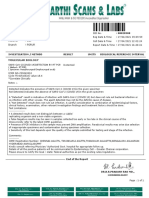
- Gopu.R:::: Patient Age / Sex 30 Y / Male BranchDocument1 paginăGopu.R:::: Patient Age / Sex 30 Y / Male BranchGopu RÎncă nu există evaluări
- Nosocomial InfectionDocument31 paginiNosocomial InfectionDr. Ashish Jawarkar0% (1)
- Prevalence of Intestinal Parasitic Infection Among Food Vendors in Purok 1, Barangay Matina Gravahan, Davao CityDocument25 paginiPrevalence of Intestinal Parasitic Infection Among Food Vendors in Purok 1, Barangay Matina Gravahan, Davao CityInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Daftar PustakaDocument7 paginiDaftar Pustakarey whiteÎncă nu există evaluări
- Talaromycosis: Click To Edit Master Title StyleDocument6 paginiTalaromycosis: Click To Edit Master Title StyleAlleah AkmadÎncă nu există evaluări
- Ghulam YaseenDocument1 paginăGhulam Yaseenuzi malikÎncă nu există evaluări
- PRO TEENS ResearchDocument24 paginiPRO TEENS ResearchWee-Weh HamjaÎncă nu există evaluări
- (23003235 - Bulletin of The Veterinary Institute in Pulawy) Microbiological Quality of Compound Feed Used in PolandDocument6 pagini(23003235 - Bulletin of The Veterinary Institute in Pulawy) Microbiological Quality of Compound Feed Used in PolandfirewÎncă nu există evaluări
- Quanti-Cult Plus ENG Dos PasesDocument4 paginiQuanti-Cult Plus ENG Dos Pasessagor sagorÎncă nu există evaluări
- Fistul Entero Kutan (FEK)Document4 paginiFistul Entero Kutan (FEK)dewiswahyuÎncă nu există evaluări
- Uv DoseDocument6 paginiUv DoseRajesh DeshmukhÎncă nu există evaluări
- Infeksi Pada Pasien KankerDocument18 paginiInfeksi Pada Pasien KankerSuci Fitriani SammuliaÎncă nu există evaluări
- Cell Phone Germs Article WORDDocument2 paginiCell Phone Germs Article WORDJack LangstonÎncă nu există evaluări
- The Main Themes of MicrobiologyDocument31 paginiThe Main Themes of MicrobiologyJhon VincentÎncă nu există evaluări
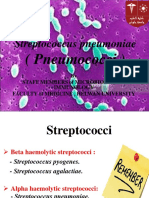
- Pneumococci MIcro LabDocument52 paginiPneumococci MIcro LabSandy AtefÎncă nu există evaluări
- Evolutionary Virology at 40: PerspectivesDocument12 paginiEvolutionary Virology at 40: PerspectivesAlejandra BarbosaÎncă nu există evaluări
- MM 010Document6 paginiMM 010worksheetbookÎncă nu există evaluări
- SpirochaetesDocument17 paginiSpirochaetesDayana PrasanthÎncă nu există evaluări
- HYPHOZYMA - Antonie Van LeeuwenhoekDocument6 paginiHYPHOZYMA - Antonie Van LeeuwenhoekcharlesÎncă nu există evaluări
- The Journal of Veterinary Medical Science: Advance PublicationDocument10 paginiThe Journal of Veterinary Medical Science: Advance PublicationTuyen TruongÎncă nu există evaluări
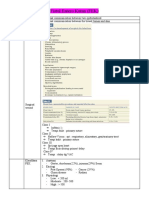
- CROUPDocument26 paginiCROUPRahul MehtaÎncă nu există evaluări
- Covid-19 RT PCR Test Sample Type: Method UsedDocument1 paginăCovid-19 RT PCR Test Sample Type: Method Usedyour mdrahamanÎncă nu există evaluări
- Growth and Physiology of BactDocument3 paginiGrowth and Physiology of Bactyam pdÎncă nu există evaluări
- In Vitro Antimicrobial Potential of Extracts and PDocument14 paginiIn Vitro Antimicrobial Potential of Extracts and PWilliam VolmerÎncă nu există evaluări
- General Principles of Microbial Pathogenesis: MicrobiologyDocument5 paginiGeneral Principles of Microbial Pathogenesis: MicrobiologyAbi SulitÎncă nu există evaluări
- Adam Abubakar Abdullahi TECHNICAL REPORTDocument40 paginiAdam Abubakar Abdullahi TECHNICAL REPORTAdam AbubakarÎncă nu există evaluări
- BioLumix NutraCBioLumix RMM Platform Featured in Latest Edition of NutraCos Journalos-Revise FINALDocument3 paginiBioLumix NutraCBioLumix RMM Platform Featured in Latest Edition of NutraCos Journalos-Revise FINALAnnabel ElizabethÎncă nu există evaluări
- Mandell Douglas and Bennetts Principles and Practice of Infectious Diseases 9Th Edition John E Bennett Raphael Dolin Martin J Blaser Full ChapterDocument68 paginiMandell Douglas and Bennetts Principles and Practice of Infectious Diseases 9Th Edition John E Bennett Raphael Dolin Martin J Blaser Full Chaptergerald.burris720100% (7)
- Group B Strep Fact SheetDocument2 paginiGroup B Strep Fact SheetDrashua AshuaÎncă nu există evaluări