S-ar putea să vă placă și
- Sustainability 10 00415Document21 paginiSustainability 10 00415jorgemauriciocuartasÎncă nu există evaluări
- El Líder y La Fortaleza de La CooperaciónDocument2 paginiEl Líder y La Fortaleza de La CooperaciónjorgemauriciocuartasÎncă nu există evaluări
- Neurotheology PDFDocument4 paginiNeurotheology PDFjorgemauriciocuartasÎncă nu există evaluări
- The Neurobiology of PleasureDocument17 paginiThe Neurobiology of PleasurejorgemauriciocuartasÎncă nu există evaluări
- Geno SpiritualityDocument18 paginiGeno SpiritualityjorgemauriciocuartasÎncă nu există evaluări
- Neurotheology PDFDocument4 paginiNeurotheology PDFjorgemauriciocuartasÎncă nu există evaluări
- Rewireyourbrain 120203041805 Phpapp02Document28 paginiRewireyourbrain 120203041805 Phpapp02jorgemauriciocuartas100% (2)
- Psychotherapy in The Age of The ComputerDocument6 paginiPsychotherapy in The Age of The ComputerjorgemauriciocuartasÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Ogranizational Behavior Course OutlineDocument9 paginiOgranizational Behavior Course Outlineqirat nadeemÎncă nu există evaluări
- Chapter - 1: Theoretical Background of The Study: 1.7 IntroductionDocument28 paginiChapter - 1: Theoretical Background of The Study: 1.7 IntroductionSalman RazaÎncă nu există evaluări
- Behavior As CommunicationDocument2 paginiBehavior As Communicationapi-435371492Încă nu există evaluări
- Rishikesh Seminar Content - SSSOHADocument13 paginiRishikesh Seminar Content - SSSOHARabindra DhitalÎncă nu există evaluări
- 100 Ways To Achieve Success in Any FieldsDocument3 pagini100 Ways To Achieve Success in Any FieldsVnAy Vn100% (1)
- Depression PDFDocument16 paginiDepression PDFMakmur SejatiÎncă nu există evaluări
- Joseph T. Gwin, Klaus Gramann, Scott Makeig and Daniel P. FerrisDocument10 paginiJoseph T. Gwin, Klaus Gramann, Scott Makeig and Daniel P. FerrisFrontiersÎncă nu există evaluări
- Case StudyDocument4 paginiCase StudyYdynn Parejas GavinaÎncă nu există evaluări
- Emotion and Cognition in Political CommunicationDocument15 paginiEmotion and Cognition in Political CommunicationKhaled Aryan ArmanÎncă nu există evaluări
- Referral Counseling - List For WebsiteDocument3 paginiReferral Counseling - List For Websiteapi-425649572Încă nu există evaluări
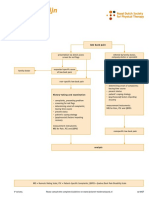
- Dutch LBP Physiotherapy FlowchartDocument2 paginiDutch LBP Physiotherapy FlowchartyohanÎncă nu există evaluări
- Hooked Workbook PDFDocument22 paginiHooked Workbook PDFalexaugusto100% (1)
- NFT PPT1 w21Document352 paginiNFT PPT1 w21Jc Manjunath ReddyÎncă nu există evaluări
- Neurodydaktyka WorkshopsDocument33 paginiNeurodydaktyka WorkshopsKinga Gąsowska-SzatałowiczÎncă nu există evaluări
- The Hierarchical Model of Approach-Avoidance MotivationDocument6 paginiThe Hierarchical Model of Approach-Avoidance MotivationRhix RheeÎncă nu există evaluări
- The Effects of Psychotherapy.. An Evaluation - Eysenck, H.J. (1952)Document6 paginiThe Effects of Psychotherapy.. An Evaluation - Eysenck, H.J. (1952)Javier SánchezÎncă nu există evaluări
- Mind Over Mass Media - Praising Effects of Tech On BrainDocument3 paginiMind Over Mass Media - Praising Effects of Tech On BrainFranco OliveraÎncă nu există evaluări
- Hearing Impairment T.brenDocument36 paginiHearing Impairment T.brenStarLord JedaxÎncă nu există evaluări
- Class 4 - LeadingDocument37 paginiClass 4 - LeadingMignionDavisÎncă nu există evaluări
- Adv Expert Progress Test2Document8 paginiAdv Expert Progress Test2Guilhermme Spiller AlonsoÎncă nu există evaluări
- Questionnaire On Compulsive BuyingDocument5 paginiQuestionnaire On Compulsive Buyingsiddhi jainÎncă nu există evaluări
- G4 Chapter 1Document12 paginiG4 Chapter 1Jovel Daniel ProtacioÎncă nu există evaluări
- Biz Ethics & NeuroscienceDocument50 paginiBiz Ethics & NeuroscienceAshchrisÎncă nu există evaluări
- Concept of PainDocument36 paginiConcept of PainSaqlain M.Încă nu există evaluări
- Fields of Specialization in PsychologyDocument1 paginăFields of Specialization in PsychologyAdrian BulusanÎncă nu există evaluări
- Cognitive Psychology Thought DisorderDocument6 paginiCognitive Psychology Thought DisorderTrisha SabaÎncă nu există evaluări
- Artificial VisionDocument7 paginiArtificial Visionmahi07404Încă nu există evaluări
- Chapter IiDocument2 paginiChapter IiRizka HartatiÎncă nu există evaluări
- Scale (Rubric) For The Diagnostic Evaluation of A Student With Down SyndromeDocument6 paginiScale (Rubric) For The Diagnostic Evaluation of A Student With Down SyndromeScribdTranslationsÎncă nu există evaluări
- LSP1501 Assessment 13Document15 paginiLSP1501 Assessment 13Annemarie RossouwÎncă nu există evaluări