S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5782)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Upt SMP Negeri 5 Pasarkemis: Dinas PendidikanDocument2 paginiUpt SMP Negeri 5 Pasarkemis: Dinas Pendidikanara ibagaztaÎncă nu există evaluări
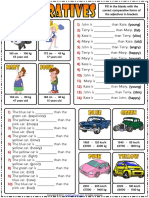
- Comparative Forms of Adjectives Esl Grammar Gap Fill Exercises WorksheetDocument2 paginiComparative Forms of Adjectives Esl Grammar Gap Fill Exercises WorksheetAnonymous LELyuBoÎncă nu există evaluări
- Katie Zodiac PDFDocument27 paginiKatie Zodiac PDFKatie LaytonÎncă nu există evaluări
- Guide To Indian ManuscriptsDocument86 paginiGuide To Indian Manuscriptsshahrad87Încă nu există evaluări
- Dungeon Vault M. - Issue No. 1Document36 paginiDungeon Vault M. - Issue No. 1Devon EaccountÎncă nu există evaluări
- GAPS Guidelines: Maintenance Program ElementsDocument17 paginiGAPS Guidelines: Maintenance Program ElementsAsad KhanÎncă nu există evaluări
- 20 Medals of PNPDocument12 pagini20 Medals of PNPJohn Paul BoclotÎncă nu există evaluări
- RRL in ThesisDocument2 paginiRRL in Thesismark_torreon100% (1)
- 20dce007 Practical1,2Document63 pagini20dce007 Practical1,2Anand BapodaraÎncă nu există evaluări
- A. Subanen Elders' Interest in The Restoration of Subanen Language 2023Document12 paginiA. Subanen Elders' Interest in The Restoration of Subanen Language 2023MEDELYN INTONGÎncă nu există evaluări
- Dashboards in Dynamics CRM 2011Document14 paginiDashboards in Dynamics CRM 2011ZhiWen TanÎncă nu există evaluări
- Ceremony - Baby Dedication PDFDocument5 paginiCeremony - Baby Dedication PDFrafaelgsccÎncă nu există evaluări
- Health Benefits of Vitamin CDocument5 paginiHealth Benefits of Vitamin CZackÎncă nu există evaluări
- Parts of a Ship ExplainedDocument9 paginiParts of a Ship ExplainedCazy DuabanÎncă nu există evaluări
- Cat 94Document255 paginiCat 94Fakerooooooooooooooooo100% (1)
- Presentation Slides: Contemporary Strategy Analysis: Concepts, Techniques, ApplicationsDocument11 paginiPresentation Slides: Contemporary Strategy Analysis: Concepts, Techniques, ApplicationsMonika SharmaÎncă nu există evaluări
- VatDocument5 paginiVatninaryzaÎncă nu există evaluări
- Biological Basis of BehaviourDocument6 paginiBiological Basis of BehaviourRichard ManuelÎncă nu există evaluări
- Fridleifsson BenefitDocument9 paginiFridleifsson BenefitWanambwa SilagiÎncă nu există evaluări
- How to knit top down sleeves flat (less than 40 charsDocument3 paginiHow to knit top down sleeves flat (less than 40 charsRadu AnghelÎncă nu există evaluări
- Tumbler Test For CokeDocument3 paginiTumbler Test For CokeDavid CazorlaÎncă nu există evaluări
- MSc XX Assignment Submission InstructionsDocument1 paginăMSc XX Assignment Submission Instructionslynnlynn23Încă nu există evaluări
- Wc4Sks: Booking DetailsDocument4 paginiWc4Sks: Booking DetailsLizaÎncă nu există evaluări
- Effect of Human Overpopulation On EnvironmentDocument2 paginiEffect of Human Overpopulation On Environmentarshad13Încă nu există evaluări
- Resume 1Document1 paginăResume 1api-661712165Încă nu există evaluări
- RA 7942 Plus CasesDocument53 paginiRA 7942 Plus CasesJessielleÎncă nu există evaluări
- Hen FruitDocument8 paginiHen FruitPuneet Singh DhaniÎncă nu există evaluări
- Mapping and Analysis of Efforts To Counter Information Pollution PDFDocument48 paginiMapping and Analysis of Efforts To Counter Information Pollution PDFAhmad Ridzalman JamalÎncă nu există evaluări
- Internal Control and Risk ManagementDocument26 paginiInternal Control and Risk ManagementPrasad LadÎncă nu există evaluări
- Nayna PorediDocument7 paginiNayna PorediMukesh ShettyÎncă nu există evaluări