S-ar putea să vă placă și
- NICU Journal: A Parent's JourneyDe la EverandNICU Journal: A Parent's JourneyÎncă nu există evaluări
- Postnatal Care of Mother and Newborn: WHO Guidelines OnDocument14 paginiPostnatal Care of Mother and Newborn: WHO Guidelines OnSuman GuptaÎncă nu există evaluări
- Maternal Child Nursing Trends and StatisticsDocument21 paginiMaternal Child Nursing Trends and StatisticsbrunoÎncă nu există evaluări
- Assessment and Management of High Risk NewbornsDocument45 paginiAssessment and Management of High Risk NewbornsShiva KarthikeyanÎncă nu există evaluări
- Palliative Ca Re For Children With Ca Ncer - : A Guide For Pa RentsDocument62 paginiPalliative Ca Re For Children With Ca Ncer - : A Guide For Pa RentsDrMBÎncă nu există evaluări
- Germany CV Format-Sample OnlyDocument6 paginiGermany CV Format-Sample Onlydeamhi nursing serviceÎncă nu există evaluări
- Miscarriage Case Presentation Community MedicineDocument25 paginiMiscarriage Case Presentation Community MedicineThuta128Încă nu există evaluări
- Follow-Up of High-Risk Newborn: DR Ankur PriyadarshiDocument90 paginiFollow-Up of High-Risk Newborn: DR Ankur PriyadarshiAnkur PriyadarshiÎncă nu există evaluări
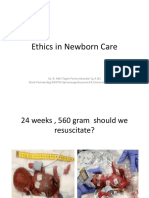
- Ethical Issues in Newborn Care: DR - Subramanyam.S Moderator - DR - SnehaDocument14 paginiEthical Issues in Newborn Care: DR - Subramanyam.S Moderator - DR - SnehaSnehaÎncă nu există evaluări
- Antenatal Care: by Dekebo G. (Gyn/Obs Resident) ModeratorDocument110 paginiAntenatal Care: by Dekebo G. (Gyn/Obs Resident) ModeratorBEREKETÎncă nu există evaluări
- Anc Inc PNCDocument29 paginiAnc Inc PNCDrArun SinghÎncă nu există evaluări
- DR Mufihatul Muniroh, Msi, Med, PH.D - Prenatal GC - WebinarNIPT-4Document49 paginiDR Mufihatul Muniroh, Msi, Med, PH.D - Prenatal GC - WebinarNIPT-4Eka Handayani OktharinaÎncă nu există evaluări
- Case Presentation Placenta PreviaDocument37 paginiCase Presentation Placenta PreviaJasmin Sabna100% (2)
- Anc 0000000000000030Document9 paginiAnc 0000000000000030maya amaliaÎncă nu există evaluări
- Effect of Initiation of Breast-Feeding Within One HourDocument20 paginiEffect of Initiation of Breast-Feeding Within One HourscribdmihÎncă nu există evaluări
- Detecting High Risk Pregnancy: Dr. Varsha L. DeshmukhDocument52 paginiDetecting High Risk Pregnancy: Dr. Varsha L. DeshmukhDiana Rose R. UlepÎncă nu există evaluări
- B-2 Pediatric Palliative Care Hospice MeetingDocument53 paginiB-2 Pediatric Palliative Care Hospice Meetingainia nur faradillaÎncă nu există evaluări
- Fetal Anomaly Scan GuidelinesDocument40 paginiFetal Anomaly Scan GuidelinesDrPraveen SharmaÎncă nu există evaluări
- Managing Placenta Previa: A Case StudyDocument38 paginiManaging Placenta Previa: A Case StudyJasmin SabnaÎncă nu există evaluări
- Ethic in Newborn CareDocument29 paginiEthic in Newborn CareIsmail GunawanÎncă nu există evaluări
- Palliative Care in Children (Aziza Shad, M.D.)Document47 paginiPalliative Care in Children (Aziza Shad, M.D.)National Press FoundationÎncă nu există evaluări
- senior project presentation 1Document30 paginisenior project presentation 1api-732018343Încă nu există evaluări
- MCN Case Presentation Group 2 1Document68 paginiMCN Case Presentation Group 2 1Mary-Ann JagonobÎncă nu există evaluări
- Visual Diagnosis and Dysmorphology Series: Trisomy 21 Approach and ManagementDocument21 paginiVisual Diagnosis and Dysmorphology Series: Trisomy 21 Approach and ManagementisauraÎncă nu există evaluări
- Syed MCHDocument83 paginiSyed MCHMushfiq RahmanÎncă nu există evaluări
- Life or Death in The NICUDocument11 paginiLife or Death in The NICUlquezada05Încă nu există evaluări
- Safe Motherhood Part-1Document52 paginiSafe Motherhood Part-1Syed MaazÎncă nu există evaluări
- Trends in The Midwifery and Obstetrical NursingDocument26 paginiTrends in The Midwifery and Obstetrical NursingNilakshi Barik Mandal89% (9)
- Term Small For Gestation BabyDocument21 paginiTerm Small For Gestation BabyCHANÎncă nu există evaluări
- Well Baby 2020 With NotesDocument119 paginiWell Baby 2020 With NotesSamsam Almarez BacaltosÎncă nu există evaluări
- Chapter 20Document52 paginiChapter 20api-3743202Încă nu există evaluări
- PQCNC 2023 Safe SleepDocument13 paginiPQCNC 2023 Safe SleepkcochranÎncă nu există evaluări
- Preventive Pediatrics Part 3Document5 paginiPreventive Pediatrics Part 3mkct111Încă nu există evaluări
- Introduction To Newborn ScreeningDocument28 paginiIntroduction To Newborn ScreeningfuufÎncă nu există evaluări
- Antenatal AssessmentDocument40 paginiAntenatal AssessmentKailash NagarÎncă nu există evaluări
- Maternal 2 Lecture All Lessons 2Document29 paginiMaternal 2 Lecture All Lessons 2Julian SantosÎncă nu există evaluări
- JR BayuDocument15 paginiJR Bayualmira.shahnazÎncă nu există evaluări
- Il Effects of Dai Treatment FinalDocument96 paginiIl Effects of Dai Treatment FinalDr SadiaÎncă nu există evaluări
- High Risk Approach in Maternal and Child HealthDocument6 paginiHigh Risk Approach in Maternal and Child Healthjyotshna sahoo100% (5)
- Control PrenatalDocument66 paginiControl PrenatalDeli CalaniÎncă nu există evaluări
- CHN FinalsDocument15 paginiCHN FinalsLuna sibilityÎncă nu există evaluări
- Community MedicineDocument248 paginiCommunity MedicineFaisal MahbubÎncă nu există evaluări
- Neonatal Palliative Care: Current Opinion in Pediatrics January 2017Document7 paginiNeonatal Palliative Care: Current Opinion in Pediatrics January 2017Raul VillacresÎncă nu există evaluări
- PQCNC Dialogues 2019 Intensive Care DecisionsDocument75 paginiPQCNC Dialogues 2019 Intensive Care DecisionskcochranÎncă nu există evaluări
- 11 Genetics Lecture - Prenatal Diagnosis & Prevention of Genetic DisordersDocument55 pagini11 Genetics Lecture - Prenatal Diagnosis & Prevention of Genetic DisordersAMIRA HELAYELÎncă nu există evaluări
- Antenatal Care: Continuing Medical Education Activities For Non-Specialists DR TC Pun 27/2/2002Document84 paginiAntenatal Care: Continuing Medical Education Activities For Non-Specialists DR TC Pun 27/2/2002tchale1Încă nu există evaluări
- Nursing Management of PregnancyDocument69 paginiNursing Management of PregnancyNANDHINIÎncă nu există evaluări
- Mother Child HealthDocument62 paginiMother Child HealthTauseef AhmadÎncă nu există evaluări
- @anesthesia Books 2016 Oxford TextbookDocument1.016 pagini@anesthesia Books 2016 Oxford TextbookAnny VelásquezÎncă nu există evaluări
- Study AuditDocument28 paginiStudy Audithj ndukaÎncă nu există evaluări
- High RiskDocument38 paginiHigh RiskDiana Rose R. Ulep100% (1)
- Educational Topic 32: Obstetric Procedures: U 2: O S C: PDocument4 paginiEducational Topic 32: Obstetric Procedures: U 2: O S C: PStetho LoveÎncă nu există evaluări
- Problems Related To Prematurity, Post Maturity, Problems Related To Gestational WeightDocument88 paginiProblems Related To Prematurity, Post Maturity, Problems Related To Gestational WeightNikky SilvestreÎncă nu există evaluări
- Wits Obstetrics 2008Document134 paginiWits Obstetrics 2008Muvenn Kannan100% (1)
- Term Breech TrialDocument9 paginiTerm Breech TrialAndy Tan Wei KeatÎncă nu există evaluări
- Management of The Rhesus Negative MotherDocument32 paginiManagement of The Rhesus Negative MothertotalpregnancycareÎncă nu există evaluări
- Pediatric Oncology Nursing CareDocument33 paginiPediatric Oncology Nursing CareBSN2G- SABLA-ON LORRAINE ANNEÎncă nu există evaluări
- Abortion, Anc, and CS: Focus+ Lecture SeriesDocument24 paginiAbortion, Anc, and CS: Focus+ Lecture SeriesTianah davisÎncă nu există evaluări
- Medication Error Report Revised 21022018 FinalDocument175 paginiMedication Error Report Revised 21022018 FinalDewi Wara ShintaÎncă nu există evaluări
- W1 and W4 Introduction and Use of Drug Utilisation Metrics Prof PontDocument36 paginiW1 and W4 Introduction and Use of Drug Utilisation Metrics Prof PontDewi Wara ShintaÎncă nu există evaluări
- SimPHARM Free Trial Start Up GuideDocument2 paginiSimPHARM Free Trial Start Up GuideDewi Wara ShintaÎncă nu există evaluări
- 6368 13314 1 SM PDFDocument7 pagini6368 13314 1 SM PDFWahyu SulistyoriniÎncă nu există evaluări
- Severe VentriculitisDocument7 paginiSevere VentriculitisDewi Wara ShintaÎncă nu există evaluări
- BTS - SIGN Asthma Guideline Quick Reference Guide 2016 PDFDocument29 paginiBTS - SIGN Asthma Guideline Quick Reference Guide 2016 PDFC. S.Încă nu există evaluări
- Appendix 10 Patient Profile TemplateDocument6 paginiAppendix 10 Patient Profile TemplateAL Rizwan AsifÎncă nu există evaluări
- Case 10 Shutter IslandDocument3 paginiCase 10 Shutter IslandAnkith ReddyÎncă nu există evaluări
- Colposcopy 2Document29 paginiColposcopy 2Prabhakar SrinivasanÎncă nu există evaluări
- STIs O & GDocument59 paginiSTIs O & GNoraÎncă nu există evaluări
- Glaucoma Management and Target IOPDocument24 paginiGlaucoma Management and Target IOPElfi RisalmaÎncă nu există evaluări
- University of Caloocan City: Bachelor of Arts Major in Political Science The Problem and Its BackgroundDocument7 paginiUniversity of Caloocan City: Bachelor of Arts Major in Political Science The Problem and Its BackgroundJericko Perez AvilaÎncă nu există evaluări
- The Effects of Foster Care Placement On Young Children's Mental HealthDocument6 paginiThe Effects of Foster Care Placement On Young Children's Mental HealthZefry Wahyu PurnamaÎncă nu există evaluări
- K-37 Septic Tank Treatment SDSDocument7 paginiK-37 Septic Tank Treatment SDSRicardo AlvaradoÎncă nu există evaluări
- A Study On Consumers Perception of Millets As A Staple FoodDocument69 paginiA Study On Consumers Perception of Millets As A Staple FoodJerin Geo JosÎncă nu există evaluări
- Renal Colic and Joint DeformitiesDocument19 paginiRenal Colic and Joint DeformitiesAhmad Syahmi YZ100% (1)
- Causes and Treatment of Onychauxis or Nail HypertrophyDocument3 paginiCauses and Treatment of Onychauxis or Nail HypertrophyKathleen BazarÎncă nu există evaluări
- Care Plan Handbook TemplateDocument34 paginiCare Plan Handbook TemplateBreanna Hopkins100% (1)
- Obstetrics 4Document9 paginiObstetrics 4Darrel Allan MandiasÎncă nu există evaluări
- CDI For ARIADocument3 paginiCDI For ARIAAshish SharmaÎncă nu există evaluări
- Paracetamol 10mg/ml Solution For Infusion PIL - UKDocument2 paginiParacetamol 10mg/ml Solution For Infusion PIL - UKnurainiÎncă nu există evaluări
- Cor-Ban 27 LDocument2 paginiCor-Ban 27 LMahammadÎncă nu există evaluări
- BP6 15depression PDFDocument75 paginiBP6 15depression PDFada ramosÎncă nu există evaluări
- Ielts Speaking 3Document34 paginiIelts Speaking 3Asad GondalÎncă nu există evaluări
- ILs Second DefenseDocument17 paginiILs Second DefenseYlrish ReyesÎncă nu există evaluări
- Yoga Therapy Intake FormDocument6 paginiYoga Therapy Intake FormGina Tricamo100% (1)
- Hashimoto ThyroiditisDocument6 paginiHashimoto Thyroiditismananginsiang100% (1)
- Case Study 1 (ENGINEERING OF SOSITY)Document22 paginiCase Study 1 (ENGINEERING OF SOSITY)mohd irfanÎncă nu există evaluări
- Types of fitness activities and modifiable risk factorsDocument14 paginiTypes of fitness activities and modifiable risk factorsMaria Cristy CanceranÎncă nu există evaluări
- Viva XT Brochure - 201203539IEp3Document6 paginiViva XT Brochure - 201203539IEp3Lubna LuaiÎncă nu există evaluări
- Lecture 1 HOPE 1Document2 paginiLecture 1 HOPE 1cally20smithÎncă nu există evaluări
- Medical Examination FormDocument1 paginăMedical Examination FormEric ZarrielloÎncă nu există evaluări
- Pre-Test Hope 2Document4 paginiPre-Test Hope 2Jodel GombaÎncă nu există evaluări
- Chrysalis Borja ResumeDocument1 paginăChrysalis Borja Resumeapi-282022271Încă nu există evaluări
- Curriculum: Minimal Access UrologyDocument14 paginiCurriculum: Minimal Access UrologyANOOP HANDAÎncă nu există evaluări
- Asthma Management in 40 CharactersDocument10 paginiAsthma Management in 40 CharactersAmalÎncă nu există evaluări