S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Surge CounterDocument2 paginiSurge CounterJavier CuzcoÎncă nu există evaluări
- Pakistan Wapda - Power Wing: Standard Operating ProceduresDocument8 paginiPakistan Wapda - Power Wing: Standard Operating Procedureszahra batoolÎncă nu există evaluări
- 01-Toy Product DesignDocument54 pagini01-Toy Product DesignJuanÎncă nu există evaluări
- Urban Problems and SolutionsDocument12 paginiUrban Problems and SolutionsJohn Lloyd Agapito50% (2)
- GNDU Contract Jobs 2013 Advertisement PDFDocument8 paginiGNDU Contract Jobs 2013 Advertisement PDFAnonymous zwCV8ZÎncă nu există evaluări
- Grieving The Loss of A Life You WantedDocument11 paginiGrieving The Loss of A Life You WantedNiftyÎncă nu există evaluări
- Pre-Placement Training Program: Sample Profiling (All About You)Document2 paginiPre-Placement Training Program: Sample Profiling (All About You)RISHAV RAJ GUPTAÎncă nu există evaluări
- Akruti Marathi MultiFont Engine ReadmeDocument22 paginiAkruti Marathi MultiFont Engine Readmenmshingote2779% (38)
- Cell Cycle Karyotyping Lab ReportDocument11 paginiCell Cycle Karyotyping Lab ReportRichie JustinÎncă nu există evaluări
- PETSOC-98-02-06 Mattar, L. McNeil, R. The Flowing Gas-Material Balance PDFDocument4 paginiPETSOC-98-02-06 Mattar, L. McNeil, R. The Flowing Gas-Material Balance PDFSolenti D'nouÎncă nu există evaluări
- Viaje Del SolDocument3 paginiViaje Del SolJanella UmiehÎncă nu există evaluări
- Intro Ducci OnDocument38 paginiIntro Ducci OnCARLOS EDUARDO AGUIRRE LEONÎncă nu există evaluări
- Reemergent Scientism, Postmodernism, and Dialogue Across DifferencesDocument7 paginiReemergent Scientism, Postmodernism, and Dialogue Across DifferencesJose Luis Ramos CañonÎncă nu există evaluări
- Refraction Through A Lens PDFDocument3 paginiRefraction Through A Lens PDFPrudhvi JoshiÎncă nu există evaluări
- De Cuong On Thi HK2 Tieng Anh 10Document5 paginiDe Cuong On Thi HK2 Tieng Anh 10hoangtouri2512Încă nu există evaluări
- Voltage Drop CalculatorDocument6 paginiVoltage Drop CalculatorMariano SanchezÎncă nu există evaluări
- NC1 AC Contactor, 9 95A: Contactors ContactorsDocument2 paginiNC1 AC Contactor, 9 95A: Contactors ContactorsYamendra GurungÎncă nu există evaluări
- Pipeline Construction InspecDocument48 paginiPipeline Construction InspecAliDadKhan100% (2)
- Swot Analysis of Revlon IncDocument5 paginiSwot Analysis of Revlon IncSubhana AsimÎncă nu există evaluări
- Foreign Direct Investment in Manufacturing and Service Sector in East AfricaDocument13 paginiForeign Direct Investment in Manufacturing and Service Sector in East AfricaFrancis NyoniÎncă nu există evaluări
- Probability spaces and σ-algebras: Scott SheffieldDocument12 paginiProbability spaces and σ-algebras: Scott SheffieldRikta DasÎncă nu există evaluări
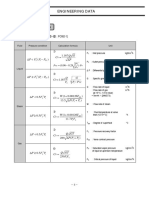
- Engineering Data: 2. CV CalculationDocument1 paginăEngineering Data: 2. CV Calculationdj22500Încă nu există evaluări
- Mae 1202: Aerospace Practicum: Lecture 4: Introduction To Basic Aerodynamics 3Document38 paginiMae 1202: Aerospace Practicum: Lecture 4: Introduction To Basic Aerodynamics 3زهديابوانسÎncă nu există evaluări
- Avenger 220 Cruise Street BS IVDocument79 paginiAvenger 220 Cruise Street BS IVShubham AatopartsÎncă nu există evaluări
- Dystopian LiteratureDocument3 paginiDystopian LiteratureLol LeeÎncă nu există evaluări
- Tavistock PrimerDocument13 paginiTavistock PrimerSharon Schaff100% (1)
- The Complete MARILLION Discography V2 PDFDocument13 paginiThe Complete MARILLION Discography V2 PDFtotalmenteprovisorioÎncă nu există evaluări
- 67 - Es - Ut Republic Csalamade BooDocument47 pagini67 - Es - Ut Republic Csalamade BooTyler LeeÎncă nu există evaluări
- Comparing Registers: MIPS vs. ARM AssemblyDocument12 paginiComparing Registers: MIPS vs. ARM Assemblyshruti chouhanÎncă nu există evaluări
- Painting and Weathering Unlocked PDFDocument91 paginiPainting and Weathering Unlocked PDFWrensEye100% (6)