S-ar putea să vă placă și
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsDe la EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsÎncă nu există evaluări
- EKG Interpretation: Making EKG/ECG Interpretation Easy!De la EverandEKG Interpretation: Making EKG/ECG Interpretation Easy!Încă nu există evaluări
- ECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasDe la EverandECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasEvaluare: 5 din 5 stele5/5 (2)
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!De la EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Încă nu există evaluări
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachDe la EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachÎncă nu există evaluări
- EKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXDe la EverandEKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXEvaluare: 5 din 5 stele5/5 (2)
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookDe la EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookÎncă nu există evaluări
- Introduction to Electrophysiological Methods and InstrumentationDe la EverandIntroduction to Electrophysiological Methods and InstrumentationÎncă nu există evaluări
- Advanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineDocument88 paginiAdvanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineRoroÎncă nu există evaluări
- Ekg Normal Dan Acs Sudin TimurDocument59 paginiEkg Normal Dan Acs Sudin TimurArum MaharaniÎncă nu există evaluări
- Advance Cardiac Life Support: Short, Sweet and to the PointDe la EverandAdvance Cardiac Life Support: Short, Sweet and to the PointEvaluare: 3 din 5 stele3/5 (2)
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!De la EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!Încă nu există evaluări
- Cardiac Arrhythmia Recognition: an easy learning guideDe la EverandCardiac Arrhythmia Recognition: an easy learning guideÎncă nu există evaluări
- Understanding Clinical Cardiac Electrophysiology: A Conceptually Guided ApproachDe la EverandUnderstanding Clinical Cardiac Electrophysiology: A Conceptually Guided ApproachÎncă nu există evaluări
- Bonehead Electrocardiography: The Easiest and Best Way to Learn How to Read Electrocardiograms—No Bones About It!De la EverandBonehead Electrocardiography: The Easiest and Best Way to Learn How to Read Electrocardiograms—No Bones About It!Evaluare: 5 din 5 stele5/5 (2)
- Basics and modern practice of nasal high-flow therapyDe la EverandBasics and modern practice of nasal high-flow therapyEvaluare: 5 din 5 stele5/5 (1)
- Brugada Phenocopy: The Art of Recognizing the Brugada ECG PatternDe la EverandBrugada Phenocopy: The Art of Recognizing the Brugada ECG PatternÎncă nu există evaluări
- Hemodynamic Rounds: Interpretation of Cardiac Pathophysiology from Pressure Waveform AnalysisDe la EverandHemodynamic Rounds: Interpretation of Cardiac Pathophysiology from Pressure Waveform AnalysisÎncă nu există evaluări
- Basics of PacemakerDocument121 paginiBasics of Pacemakerjeenath justin doss100% (1)
- Acute Resuscitation and Crisis Management: Acute Critical Events Simulation (ACES)De la EverandAcute Resuscitation and Crisis Management: Acute Critical Events Simulation (ACES)David NeilipovitzÎncă nu există evaluări
- Electrocardiography Method (ECG/EKG): A Primary Guideline for Starters to Understand about Arrhythmias & EKG InterpretationDe la EverandElectrocardiography Method (ECG/EKG): A Primary Guideline for Starters to Understand about Arrhythmias & EKG InterpretationÎncă nu există evaluări
- ECG Master Class-2Document138 paginiECG Master Class-2Shohag ID Center100% (1)
- Cardiac PharmacologyDe la EverandCardiac PharmacologyR. Douglas WilkersonEvaluare: 5 din 5 stele5/5 (1)
- Ectopic Heartbeats, (Extrasystoles) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandEctopic Heartbeats, (Extrasystoles) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Practical Handbook of Advanced Interventional Cardiology: Tips and TricksDe la EverandPractical Handbook of Advanced Interventional Cardiology: Tips and TricksÎncă nu există evaluări
- Wolff-Parkinson- White-Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandWolff-Parkinson- White-Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Emergency Department Resuscitation of the Critically Ill, 2nd Edition: A Crash Course in Critical CareDe la EverandEmergency Department Resuscitation of the Critically Ill, 2nd Edition: A Crash Course in Critical CareÎncă nu există evaluări
- Heart Valve Diseases, A Simple Guide to These ConditionsDe la EverandHeart Valve Diseases, A Simple Guide to These ConditionsÎncă nu există evaluări
- Haemodynamic Monitoring & Manipulation: an easy learning guideDe la EverandHaemodynamic Monitoring & Manipulation: an easy learning guideÎncă nu există evaluări
- Bennett's Cardiac Arrhythmias: Practical Notes on Interpretation and TreatmentDe la EverandBennett's Cardiac Arrhythmias: Practical Notes on Interpretation and TreatmentÎncă nu există evaluări
- Cardiac Care: An Introduction for Healthcare ProfessionalsDe la EverandCardiac Care: An Introduction for Healthcare ProfessionalsÎncă nu există evaluări
- ACLS Advanced Cardiovascular Life Support Provider Manual 2023De la EverandACLS Advanced Cardiovascular Life Support Provider Manual 2023Încă nu există evaluări
- Cardiac PacingDocument89 paginiCardiac Pacingsandwhale056Încă nu există evaluări
- Hemodynamics in The Cath Lab 2Document45 paginiHemodynamics in The Cath Lab 2usfcards100% (1)
- IV PDFDocument63 paginiIV PDFelbagouryÎncă nu există evaluări
- Advanced Practice in Critical Care: A Case Study ApproachDe la EverandAdvanced Practice in Critical Care: A Case Study ApproachSarah McGloinÎncă nu există evaluări
- DubinDocument14 paginiDubinС. Марина100% (1)
- Critical Decisions in Emergency and Acute Care ElectrocardiographyDe la EverandCritical Decisions in Emergency and Acute Care ElectrocardiographyÎncă nu există evaluări
- Basics of EKG InterpretationDocument132 paginiBasics of EKG InterpretationSiddhant GautamÎncă nu există evaluări
- Anesthesia for Congenital Heart DiseaseDe la EverandAnesthesia for Congenital Heart DiseaseStephen A. StayerÎncă nu există evaluări
- Cardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandCardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- OB-GYN QuestionsDocument10 paginiOB-GYN QuestionsArianne Joy C. TamarayÎncă nu există evaluări
- Pharmaa Topnotch ReviewDocument14 paginiPharmaa Topnotch ReviewArianne Joy C. TamarayÎncă nu există evaluări
- Clinical Microbiology QuestionsDocument18 paginiClinical Microbiology QuestionsArianne Joy C. TamarayÎncă nu există evaluări
- Anahisto ReviewerDocument13 paginiAnahisto ReviewerArianne Joy C. TamarayÎncă nu există evaluări
- Benign Gyecologic LesionDocument158 paginiBenign Gyecologic LesionArianne Joy C. TamarayÎncă nu există evaluări
- Dermatology Cutaneous Bacterial InfectionsDocument139 paginiDermatology Cutaneous Bacterial InfectionsArianne Joy C. TamarayÎncă nu există evaluări
- ENTDocument15 paginiENTArianne Joy C. TamarayÎncă nu există evaluări
- Microbiology Comprehensive ExamDocument15 paginiMicrobiology Comprehensive ExamArianne Joy C. TamarayÎncă nu există evaluări
- Parasitology Lec ExamDocument6 paginiParasitology Lec ExamArianne Joy C. TamarayÎncă nu există evaluări
- Liver and Spleen DiseasesDocument72 paginiLiver and Spleen DiseasesArianne Joy C. TamarayÎncă nu există evaluări
- Docshare - Tips - High Yield Biochemistrypdf PDFDocument41 paginiDocshare - Tips - High Yield Biochemistrypdf PDFArianne Joy C. TamarayÎncă nu există evaluări
- Indiabix MicroDocument88 paginiIndiabix MicroArianne Joy C. TamarayÎncă nu există evaluări
- Recall Series Anatomy Recall (PDF) Lorne H. Blackbourne PDFDocument282 paginiRecall Series Anatomy Recall (PDF) Lorne H. Blackbourne PDFArianne Joy C. TamarayÎncă nu există evaluări
- Effect of Progressive Muscle Relaxation Combined With Deep Breathing Technique Immediately After Aerobic Exercises On Essential HypertensionDocument2 paginiEffect of Progressive Muscle Relaxation Combined With Deep Breathing Technique Immediately After Aerobic Exercises On Essential HypertensionNetraÎncă nu există evaluări
- The Little Black Book of Ecg Secrets PDFDocument12 paginiThe Little Black Book of Ecg Secrets PDFamaandreiÎncă nu există evaluări
- Interpretation of Head CT Scan Ischaemic StrokeDocument7 paginiInterpretation of Head CT Scan Ischaemic StrokePutra DhyatmikaÎncă nu există evaluări
- PaediatricEMQsAAMallick PDFDocument7 paginiPaediatricEMQsAAMallick PDFMuzhaffar Abdullah100% (1)
- Supraventricular TachycardiaDocument20 paginiSupraventricular TachycardiaBenyWirananggalaÎncă nu există evaluări
- Daftar Pustaka StemiDocument2 paginiDaftar Pustaka StemiEndang Rahayu Fuji LestaryÎncă nu există evaluări
- Ebook Cardiology Board Review and Self Assessment A Companion Guide To Hursts The Heart PDF Full Chapter PDFDocument67 paginiEbook Cardiology Board Review and Self Assessment A Companion Guide To Hursts The Heart PDF Full Chapter PDFjohn.eastman290100% (26)
- Aorta Replacement and Repair Thoracic Aortic DissectionDocument3 paginiAorta Replacement and Repair Thoracic Aortic DissectionprofarmahÎncă nu există evaluări
- Clinchers 100 Important PointsDocument21 paginiClinchers 100 Important PointsNeha GoelÎncă nu există evaluări
- Dr. Atif Sher ASCVD CardioConDocument21 paginiDr. Atif Sher ASCVD CardioConwali ahmedÎncă nu există evaluări
- Ischemic Heart Disease PWDocument13 paginiIschemic Heart Disease PWEunica RamosÎncă nu există evaluări
- Example of Nursing Diagnosis Risk For Decreased Cardiac OutputDocument5 paginiExample of Nursing Diagnosis Risk For Decreased Cardiac OutputAndi Faramida HamzahÎncă nu există evaluări
- Congenital Heart Diseases: TopicsDocument19 paginiCongenital Heart Diseases: TopicsMaheen SyedÎncă nu există evaluări
- Echocardiography Assessment of Coronary Artery DiseaseDocument28 paginiEchocardiography Assessment of Coronary Artery DiseaseYibeltal AssefaÎncă nu există evaluări
- Care Plan Unstable AnginaDocument4 paginiCare Plan Unstable Anginaالغزال الذهبي50% (6)
- Ecg Indice 9788876407246Document12 paginiEcg Indice 9788876407246AndreaHistoryXÎncă nu există evaluări
- CAD, HPN, HyperlipidemiaDocument8 paginiCAD, HPN, Hyperlipidemiasarguss14100% (2)
- Physio MCqsDocument3 paginiPhysio MCqsraguchandra7527Încă nu există evaluări
- Case Study Congestive Heart Failure Patho)Document8 paginiCase Study Congestive Heart Failure Patho)Mj Silva100% (3)
- Saudi License Exam (SLE) 3rd Edt. UQUDocument445 paginiSaudi License Exam (SLE) 3rd Edt. UQUkingmedic98% (41)
- Delta Wave - LITFL Medical Blog - ECG Library BasicsDocument9 paginiDelta Wave - LITFL Medical Blog - ECG Library BasicsLauraÎncă nu există evaluări
- First Aid of Heart AttackDocument3 paginiFirst Aid of Heart Attackarram madhaviÎncă nu există evaluări
- ECG Self Study BookDocument390 paginiECG Self Study BookChandramohan SettyÎncă nu există evaluări
- MnemonicDocument4 paginiMnemonicdrsajjadpathan1113Încă nu există evaluări
- Materi Dasar EkgDocument52 paginiMateri Dasar EkgFirsandiPrasastyaFikryGozali100% (2)
- Jadwal Sympo Edit1Document3 paginiJadwal Sympo Edit1reyÎncă nu există evaluări
- ECG in Emergency MedicineDocument228 paginiECG in Emergency MedicineBobbyGustafsonÎncă nu există evaluări
- Rheumatic Heart DiseaseDocument3 paginiRheumatic Heart DiseaseWay LeeÎncă nu există evaluări
- Chapter62-Management of Patients With Cerebrovascular DisordersDocument35 paginiChapter62-Management of Patients With Cerebrovascular DisordersAhmed 123100% (1)
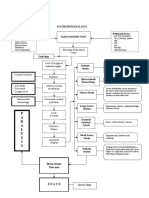
- Pathophysiology: P A R A L Y S I SDocument1 paginăPathophysiology: P A R A L Y S I SJordan Garcia AguilarÎncă nu există evaluări