S-ar putea să vă placă și
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentDe la EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentÎncă nu există evaluări
- The Treatment Strategy of An Oblique Complicated Crownroot Fracturecase Report PDC 1000110Document4 paginiThe Treatment Strategy of An Oblique Complicated Crownroot Fracturecase Report PDC 1000110Isabel Escobar MinotasÎncă nu există evaluări
- Diastemma ClosureDocument3 paginiDiastemma Closureisha sajjanharÎncă nu există evaluări
- Management of A Palatal Gingival Groove in A Maxillary Lateral Incisor: A Case ReportDocument4 paginiManagement of A Palatal Gingival Groove in A Maxillary Lateral Incisor: A Case ReporthappykglayÎncă nu există evaluări
- Hemisection A Treatment Option For An Endodontically Treated Molar With Vertical Root FractureDocument3 paginiHemisection A Treatment Option For An Endodontically Treated Molar With Vertical Root FracturePaulo CastroÎncă nu există evaluări
- Tanpa Judul PDFDocument7 paginiTanpa Judul PDFnadyashintakasihÎncă nu există evaluări
- Conservative and Esthetic Management of Diastema Closure Using Porcelain Laminate VeneersDocument5 paginiConservative and Esthetic Management of Diastema Closure Using Porcelain Laminate VeneersLuis Alberto Carpio MorenoÎncă nu există evaluări
- Case Report Management of Adverse Tissue Response To Faulty Pontic Design-A Case ReportDocument5 paginiCase Report Management of Adverse Tissue Response To Faulty Pontic Design-A Case ReportNajeeb UllahÎncă nu există evaluări
- Journal Occlusal 2Document4 paginiJournal Occlusal 2Felianda ThaliaÎncă nu există evaluări
- Frenectomy - Different TechniquesDocument7 paginiFrenectomy - Different TechniquesIJAR JOURNALÎncă nu există evaluări
- Interdisciplinary Management of A Severely Compromised Periodontal Patient - Case ReportDocument10 paginiInterdisciplinary Management of A Severely Compromised Periodontal Patient - Case ReportAPinhaoFerreiraÎncă nu există evaluări
- Distalization of Impacted Mandibular SecondDocument6 paginiDistalization of Impacted Mandibular SecondPatricia BurbanoÎncă nu există evaluări
- Preservation of A Split Tooth - JC 3.1Document49 paginiPreservation of A Split Tooth - JC 3.1veena rÎncă nu există evaluări
- Case Report19Document6 paginiCase Report19irfanaÎncă nu există evaluări
- Role of PeriodontistDocument5 paginiRole of PeriodontistNeetha ShenoyÎncă nu există evaluări
- Lingualized Occlusion-A Case ReportDocument4 paginiLingualized Occlusion-A Case ReportSkAliHassanÎncă nu există evaluări
- Frenectomy As A Multidisciplinary Prostho-Perio Management Approach For Partial Denture-A Case ReportDocument6 paginiFrenectomy As A Multidisciplinary Prostho-Perio Management Approach For Partial Denture-A Case ReportMidda SosmedÎncă nu există evaluări
- Dentigerous CystDocument6 paginiDentigerous CystZahid ManzoorÎncă nu există evaluări
- Jurnal Kasus Tambahan 3 - Khairin Yonni (12730)Document6 paginiJurnal Kasus Tambahan 3 - Khairin Yonni (12730)Khairin YonniÎncă nu există evaluări
- Protesis Fija Con Ataches. Rep Caso. 2020. Cureus. SivakumarDocument13 paginiProtesis Fija Con Ataches. Rep Caso. 2020. Cureus. SivakumarAngela AcostaÎncă nu există evaluări
- Gen Dent 2018Document4 paginiGen Dent 2018nandaÎncă nu există evaluări
- Case Report Endo Perio Lesions-A Synergistic ApproachDocument5 paginiCase Report Endo Perio Lesions-A Synergistic ApproachRyanka Dizayani PutraÎncă nu există evaluări
- ISSN 2347-5579: Iatrogenic Dentistry and Periodontal Disease: A Review With Two CasesDocument3 paginiISSN 2347-5579: Iatrogenic Dentistry and Periodontal Disease: A Review With Two CasesVineet ArunÎncă nu există evaluări
- Ijda July-Sep 2015Document5 paginiIjda July-Sep 2015bhaskaracharya dontabhaktuniÎncă nu există evaluări
- Stefanini2020 Periimplant Papillae ReconstructionDocument11 paginiStefanini2020 Periimplant Papillae ReconstructionTravis HarveyÎncă nu există evaluări
- Prosthodontic Management of Combination Syndrome Case With Metal Reinforced Maxillary Complete Denture and Mandibular Teeth Suppor PDFDocument5 paginiProsthodontic Management of Combination Syndrome Case With Metal Reinforced Maxillary Complete Denture and Mandibular Teeth Suppor PDFMonalisha DasÎncă nu există evaluări
- Maxillary Labial Frenectomy by Using ConDocument6 paginiMaxillary Labial Frenectomy by Using ConShinta rahma MansyurÎncă nu există evaluări
- Endodontic Treatment of A Large Periradicular Lesion: A Case ReportDocument4 paginiEndodontic Treatment of A Large Periradicular Lesion: A Case ReportSholehudin Al AyubiÎncă nu există evaluări
- Endodontic Treatment of A Large Periradicular Lesion: A Case ReportDocument4 paginiEndodontic Treatment of A Large Periradicular Lesion: A Case ReportSholehudin Al AyubiÎncă nu există evaluări
- Department of Pediatric & Preventive DentistryDocument3 paginiDepartment of Pediatric & Preventive DentistryRenieKumalaÎncă nu există evaluări
- Bimaxilary ProtrusionDocument7 paginiBimaxilary ProtrusionD YasIr MussaÎncă nu există evaluări
- ARTICAL1Document7 paginiARTICAL1Aseel AnesÎncă nu există evaluări
- Apiko 1Document5 paginiApiko 1Asri DamayantiÎncă nu există evaluări
- Case Studies Collection 22Document39 paginiCase Studies Collection 22Eduard ConstantinÎncă nu există evaluări
- Hemisection of A Severely Decayed Mandibular Molar: A Case ReportDocument4 paginiHemisection of A Severely Decayed Mandibular Molar: A Case Reportkartika tiaraÎncă nu există evaluări
- New Treatment Option For An Incomplete Vertical Root Fracture Case StudyDocument4 paginiNew Treatment Option For An Incomplete Vertical Root Fracture Case StudyTarun KumarÎncă nu există evaluări
- ARTUCULO DR CHAVEZ AMELOGENESIS13256 - 2020 - Article - 2586Document7 paginiARTUCULO DR CHAVEZ AMELOGENESIS13256 - 2020 - Article - 2586marcelaÎncă nu există evaluări
- Oktawati 2020Document3 paginiOktawati 2020Mariatun ZahronasutionÎncă nu există evaluări
- Endodontc Surgical Management of Mucosal FenistrationDocument3 paginiEndodontc Surgical Management of Mucosal Fenistrationfun timesÎncă nu există evaluări
- Article 1525485399Document4 paginiArticle 1525485399anisah fadilahÎncă nu există evaluări
- A To Z Orthodontics Vol 20 SurgicalDocument23 paginiA To Z Orthodontics Vol 20 Surgicalshruti premsagarÎncă nu există evaluări
- Management of Fracture Tooth Fragment Reattachment: Case ReportDocument7 paginiManagement of Fracture Tooth Fragment Reattachment: Case Reportwaleed MagidÎncă nu există evaluări
- Orthodontic Management of Midline Diastema in Mixed DentitionDocument5 paginiOrthodontic Management of Midline Diastema in Mixed DentitionfatimahÎncă nu există evaluări
- TMP 371 BDocument4 paginiTMP 371 BFrontiersÎncă nu există evaluări
- An Innovative Technique To Restore The Non Vital Teeth With Wide Open Canals - A Clinical StudyDocument4 paginiAn Innovative Technique To Restore The Non Vital Teeth With Wide Open Canals - A Clinical StudyIOSRjournalÎncă nu există evaluări
- Badami 2011Document5 paginiBadami 2011ayoubÎncă nu există evaluări
- A Two-Step Separation Technique For Fused Teeth: Clinical ReportDocument3 paginiA Two-Step Separation Technique For Fused Teeth: Clinical ReportAya Ibrahim YassinÎncă nu există evaluări
- Yang Articulo 16Document5 paginiYang Articulo 16hugo alonso porras alvarezÎncă nu există evaluări
- HaseebaK EtalDocument5 paginiHaseebaK EtalIndah VitasariÎncă nu există evaluări
- 2020 Article 265Document7 pagini2020 Article 265Fabian BarretoÎncă nu există evaluări
- 23 Case Rep1 Palatogingival GrooveDocument7 pagini23 Case Rep1 Palatogingival GrooveDr.O.R.GANESAMURTHIÎncă nu există evaluări
- Periodontal Plastic Surgery in The Management of Multiple Gingival Recessions Two Therapeutic ApproachesDocument5 paginiPeriodontal Plastic Surgery in The Management of Multiple Gingival Recessions Two Therapeutic ApproachesInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Management of Fractured Lateral Incisor by Surgical Extrusion and Its Prosthetic RehabilitationA Case ReportDocument5 paginiManagement of Fractured Lateral Incisor by Surgical Extrusion and Its Prosthetic RehabilitationA Case ReportInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Combined Endo-Perio Lesion in An Anterior Tooth, Its Management & Resolution - A Case ReportDocument4 paginiCombined Endo-Perio Lesion in An Anterior Tooth, Its Management & Resolution - A Case ReportsulistiyaÎncă nu există evaluări
- Clinical Case Reports - 2023 - Vyver - Apexification of Dens Evaginatus in A Mandibular Premolar A Case ReportDocument6 paginiClinical Case Reports - 2023 - Vyver - Apexification of Dens Evaginatus in A Mandibular Premolar A Case ReportIqra KhanÎncă nu există evaluări
- Journal of The World Federation of OrthodontistsDocument6 paginiJournal of The World Federation of OrthodontistsJuan Carlos MeloÎncă nu există evaluări
- Black Triangle PDFDocument4 paginiBlack Triangle PDFzinniaÎncă nu există evaluări
- SRMJResDentSci24352-6390498 174504Document4 paginiSRMJResDentSci24352-6390498 174504Sandeep singhÎncă nu există evaluări
- Case Report/Clinical Technique Nonsurgical Endodontic Treatment of Dens Invaginatus With Large Periradicular Lesion: A CaseDocument4 paginiCase Report/Clinical Technique Nonsurgical Endodontic Treatment of Dens Invaginatus With Large Periradicular Lesion: A CaseVikas DeepÎncă nu există evaluări
- Implicaciones Periodontales Del Tratamiento Quirúrgico-OrtodónticoDocument9 paginiImplicaciones Periodontales Del Tratamiento Quirúrgico-OrtodónticoAlfredo NovoaÎncă nu există evaluări
- Analysis of Ancol Beach Object Development Using Business Model Canvas ApproachDocument8 paginiAnalysis of Ancol Beach Object Development Using Business Model Canvas ApproachAnonymous izrFWiQÎncă nu există evaluări
- Teacher Leaders' Experience in The Shared Leadership ModelDocument4 paginiTeacher Leaders' Experience in The Shared Leadership ModelAnonymous izrFWiQÎncă nu există evaluări
- Design and Analysis of Humanitarian Aid Delivery RC AircraftDocument6 paginiDesign and Analysis of Humanitarian Aid Delivery RC AircraftAnonymous izrFWiQÎncă nu există evaluări
- Experimental Investigation On Performance of Pre-Mixed Charge Compression Ignition EngineDocument5 paginiExperimental Investigation On Performance of Pre-Mixed Charge Compression Ignition EngineAnonymous izrFWiQÎncă nu există evaluări
- Investigations On BTTT As Qualitative Tool For Identification of Different Brands of Groundnut Oils Available in Markets of IndiaDocument5 paginiInvestigations On BTTT As Qualitative Tool For Identification of Different Brands of Groundnut Oils Available in Markets of IndiaAnonymous izrFWiQÎncă nu există evaluări
- Women in The Civil Service: Performance, Leadership and EqualityDocument4 paginiWomen in The Civil Service: Performance, Leadership and EqualityAnonymous izrFWiQÎncă nu există evaluări
- Incidence of Temporary Threshold Shift After MRI (Head and Neck) in Tertiary Care CentreDocument4 paginiIncidence of Temporary Threshold Shift After MRI (Head and Neck) in Tertiary Care CentreAnonymous izrFWiQÎncă nu există evaluări
- Evaluation of Assessing The Purity of Sesame Oil Available in Markets of India Using Bellier Turbidity Temperature Test (BTTT)Document4 paginiEvaluation of Assessing The Purity of Sesame Oil Available in Markets of India Using Bellier Turbidity Temperature Test (BTTT)Anonymous izrFWiQÎncă nu există evaluări
- Bioadhesive Inserts of Prednisolone Acetate For Postoperative Management of Cataract - Development and EvaluationDocument8 paginiBioadhesive Inserts of Prednisolone Acetate For Postoperative Management of Cataract - Development and EvaluationAnonymous izrFWiQÎncă nu există evaluări
- Securitization of Government School Building by PPP ModelDocument8 paginiSecuritization of Government School Building by PPP ModelAnonymous izrFWiQÎncă nu există evaluări
- Knowledge and Utilisation of Various Schemes of RCH Program Among Antenatal Women and Mothers Having Less Than Five Child in A Semi-Urban Township of ChennaiDocument5 paginiKnowledge and Utilisation of Various Schemes of RCH Program Among Antenatal Women and Mothers Having Less Than Five Child in A Semi-Urban Township of ChennaiAnonymous izrFWiQÎncă nu există evaluări
- Platelet-Rich Plasma in Orthodontics - A ReviewDocument6 paginiPlatelet-Rich Plasma in Orthodontics - A ReviewAnonymous izrFWiQÎncă nu există evaluări
- IJISRT19AUG928Document6 paginiIJISRT19AUG928Anonymous izrFWiQÎncă nu există evaluări
- Child Rights Violation and Mechanism For Protection of Children Rights in Southern Africa: A Perspective of Central, Eastern and Luapula Provinces of ZambiaDocument13 paginiChild Rights Violation and Mechanism For Protection of Children Rights in Southern Africa: A Perspective of Central, Eastern and Luapula Provinces of ZambiaAnonymous izrFWiQÎncă nu există evaluări
- Enhanced Opinion Mining Approach For Product ReviewsDocument4 paginiEnhanced Opinion Mining Approach For Product ReviewsAnonymous izrFWiQÎncă nu există evaluări
- A Wave Energy Generation Device Using Impact Force of A Breaking Wave Based Purely On Gear CompoundingDocument8 paginiA Wave Energy Generation Device Using Impact Force of A Breaking Wave Based Purely On Gear CompoundingAnonymous izrFWiQÎncă nu există evaluări
- Application of Analytical Hierarchy Process Method On The Selection Process of Fresh Fruit Bunch Palm Oil SupplierDocument12 paginiApplication of Analytical Hierarchy Process Method On The Selection Process of Fresh Fruit Bunch Palm Oil SupplierAnonymous izrFWiQÎncă nu există evaluări
- IJISRT19AUG928Document6 paginiIJISRT19AUG928Anonymous izrFWiQÎncă nu există evaluări
- Risk Assessment: A Mandatory Evaluation and Analysis of Periodontal Tissue in General Population - A SurveyDocument7 paginiRisk Assessment: A Mandatory Evaluation and Analysis of Periodontal Tissue in General Population - A SurveyAnonymous izrFWiQÎncă nu există evaluări
- Comparison of Continuum Constitutive Hyperelastic Models Based On Exponential FormsDocument8 paginiComparison of Continuum Constitutive Hyperelastic Models Based On Exponential FormsAnonymous izrFWiQÎncă nu există evaluări
- Trade Liberalization and Total Factor Productivity of Indian Capital Goods IndustriesDocument4 paginiTrade Liberalization and Total Factor Productivity of Indian Capital Goods IndustriesAnonymous izrFWiQÎncă nu există evaluări
- SWOT Analysis and Development of Culture-Based Accounting Curriculum ModelDocument11 paginiSWOT Analysis and Development of Culture-Based Accounting Curriculum ModelAnonymous izrFWiQÎncă nu există evaluări
- Effect Commitment, Motivation, Work Environment On Performance EmployeesDocument8 paginiEffect Commitment, Motivation, Work Environment On Performance EmployeesAnonymous izrFWiQÎncă nu există evaluări
- Exam Anxiety in Professional Medical StudentsDocument5 paginiExam Anxiety in Professional Medical StudentsAnonymous izrFWiQ100% (1)
- Pharmaceutical Waste Management in Private Pharmacies of Kaski District, NepalDocument23 paginiPharmaceutical Waste Management in Private Pharmacies of Kaski District, NepalAnonymous izrFWiQÎncă nu există evaluări
- Revived Article On Alternative Therapy For CancerDocument3 paginiRevived Article On Alternative Therapy For CancerAnonymous izrFWiQÎncă nu există evaluări
- Assessment of Health-Care Expenditure For Health Insurance Among Teaching Faculty of A Private UniversityDocument7 paginiAssessment of Health-Care Expenditure For Health Insurance Among Teaching Faculty of A Private UniversityAnonymous izrFWiQÎncă nu există evaluări
- The Influence of Benefits of Coastal Tourism Destination On Community Participation With Transformational Leadership ModerationDocument9 paginiThe Influence of Benefits of Coastal Tourism Destination On Community Participation With Transformational Leadership ModerationAnonymous izrFWiQÎncă nu există evaluări
- To Estimate The Prevalence of Sleep Deprivation and To Assess The Awareness & Attitude Towards Related Health Problems Among Medical Students in Saveetha Medical CollegeDocument4 paginiTo Estimate The Prevalence of Sleep Deprivation and To Assess The Awareness & Attitude Towards Related Health Problems Among Medical Students in Saveetha Medical CollegeAnonymous izrFWiQÎncă nu există evaluări
- Cekic Nagas2016 PDFDocument8 paginiCekic Nagas2016 PDFAkanksha MahajanÎncă nu există evaluări
- Dental CingulumDocument2 paginiDental Cingulumakm BasharÎncă nu există evaluări
- Iotn Training SlidesDocument38 paginiIotn Training SlidesAchini LiyanageÎncă nu există evaluări
- Dentition and Detection of Age in AnimalsDocument25 paginiDentition and Detection of Age in AnimalsMuhammad Ali ShuvoÎncă nu există evaluări
- Updated Prometic Dental Exam 2018: Important NoticesDocument51 paginiUpdated Prometic Dental Exam 2018: Important NoticesMohsen Saeed OzaibiÎncă nu există evaluări
- Prevalensi MalocclusionDocument5 paginiPrevalensi MalocclusionIdelia GunawanÎncă nu există evaluări
- Histology of Tooth DevelopmentDocument31 paginiHistology of Tooth DevelopmentMuzzamil MughalÎncă nu există evaluări
- Flavio Esthetic JigDocument14 paginiFlavio Esthetic Jigjotapintor100% (4)
- Dental Anatomy and Physiology Course OverviewDocument2 paginiDental Anatomy and Physiology Course OverviewMarinel VillaneraÎncă nu există evaluări
- Managing Impacted Upper Canine with Surgical ExposureDocument6 paginiManaging Impacted Upper Canine with Surgical ExposureBinta Bhirawa AnoragaÎncă nu există evaluări
- Treatment Planning for Loss of First Permanent MolarsDocument6 paginiTreatment Planning for Loss of First Permanent Molarsplayer osamaÎncă nu există evaluări
- Contemporary Oral and Maxillofacial Pathology, 2nd EditionDocument456 paginiContemporary Oral and Maxillofacial Pathology, 2nd Editionaisyarahma zanuaryÎncă nu există evaluări
- PAR Scoring Sheet - 2017Document1 paginăPAR Scoring Sheet - 2017Assem AbdejawwadÎncă nu există evaluări
- Formative CellsDocument33 paginiFormative CellsSrishti SrivastavaÎncă nu există evaluări
- Endodontics Chapter Questions SummaryDocument7 paginiEndodontics Chapter Questions SummaryBinayak UpadhyayaÎncă nu există evaluări
- 300 Dental Anatomy Facts in 38 CharactersDocument13 pagini300 Dental Anatomy Facts in 38 Charactersmilagros falconÎncă nu există evaluări
- Dental Diseases and Conditions ListDocument1 paginăDental Diseases and Conditions ListPenagihan Rs Tugu IbuÎncă nu există evaluări
- Prometric Dental Exam QuestionsDocument10 paginiPrometric Dental Exam QuestionsmidhunÎncă nu există evaluări
- Radiography, Dental (LENGKAP)Document57 paginiRadiography, Dental (LENGKAP)mimanchi_megumiÎncă nu există evaluări
- 05 Hardy 1951 The Developments in The Occlusal Patterns of Artificial TeethDocument15 pagini05 Hardy 1951 The Developments in The Occlusal Patterns of Artificial Teethjorefe12Încă nu există evaluări
- Smile Arc Protection Part 2Document4 paginiSmile Arc Protection Part 2M.Laura100% (1)
- Mass Retraction Movement of The Anterior Upper Teeth Using Orthodontic Mini-Implants As AnchorageDocument6 paginiMass Retraction Movement of The Anterior Upper Teeth Using Orthodontic Mini-Implants As AnchorageYerly Ramirez MuñozÎncă nu există evaluări
- Adts Guidelines For Access CavityDocument7 paginiAdts Guidelines For Access Cavityrojek63Încă nu există evaluări
- Daftar Pustaka Maxilar Rapid ExpansionDocument3 paginiDaftar Pustaka Maxilar Rapid ExpansionMegaRafikaBarorohÎncă nu există evaluări
- Articulo MsxillaryDocument13 paginiArticulo MsxillaryAndres CarvajalÎncă nu există evaluări
- 2 Biomechanical Considerations For Controlling Target Tooth Movement With Mini-ImplantsDocument10 pagini2 Biomechanical Considerations For Controlling Target Tooth Movement With Mini-ImplantsZepol MlmÎncă nu există evaluări
- Lectenamel 161125053323Document86 paginiLectenamel 161125053323prince1324shÎncă nu există evaluări
- Intrusion With Mini ImplantDocument13 paginiIntrusion With Mini Implantdrzana78100% (1)
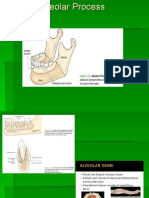
- Alveolar BoneDocument24 paginiAlveolar BoneHanna SouthwellÎncă nu există evaluări
- Dental Caries Classification Guide - Types, Stages & FactorsDocument80 paginiDental Caries Classification Guide - Types, Stages & FactorsAjinkya KadamÎncă nu există evaluări