S-ar putea să vă placă și
- Brachial Plexus Palsy: A Therapy Guide For Your BabyDocument8 paginiBrachial Plexus Palsy: A Therapy Guide For Your BabyNovy Dita100% (1)
- Beasley Et Al 2017 RespirologyDocument2 paginiBeasley Et Al 2017 RespirologyPromkes cibungbulangÎncă nu există evaluări
- CF Ventilation ManagementDocument10 paginiCF Ventilation ManagementSherry SaidÎncă nu există evaluări
- Raphelson Et Al 2023 Sleep Apnea and Chronic Obstructive Pulmonary Disease Overlap More Common Than You ThinkDocument2 paginiRaphelson Et Al 2023 Sleep Apnea and Chronic Obstructive Pulmonary Disease Overlap More Common Than You ThinkmickychaladiÎncă nu există evaluări
- Vincent-Slutsky2020 Article WeVeNeverSeenAPatientWithARDSDocument3 paginiVincent-Slutsky2020 Article WeVeNeverSeenAPatientWithARDSHoracio Panzardo GonzálezÎncă nu există evaluări
- High-Flow Nasal Oxygen-The Pendulum Continues To Swing in The Assessment of Critical Care TechnologyDocument2 paginiHigh-Flow Nasal Oxygen-The Pendulum Continues To Swing in The Assessment of Critical Care TechnologyRodrigoSachiFreitasÎncă nu există evaluări
- Ventilation During Lung Resection and Critical Care ComparativeDocument11 paginiVentilation During Lung Resection and Critical Care Comparativeema moralesÎncă nu există evaluări
- Chest: Point/Counterpoint EditorialsDocument3 paginiChest: Point/Counterpoint Editorialsgiseladelarosa2006Încă nu există evaluări
- Evaluando El Asma SeveroDocument3 paginiEvaluando El Asma SeveroJaime Guillén OrdóñezÎncă nu există evaluări
- ARDS ParalisisDocument7 paginiARDS ParalisisMarvin M. Vargas AlayoÎncă nu există evaluări
- Correct Inhalation Technique Is Critical in Achieving GoodDocument2 paginiCorrect Inhalation Technique Is Critical in Achieving GoodSelvy YusmaÎncă nu există evaluări
- Pertanyaan 7Document14 paginiPertanyaan 7WicakÎncă nu există evaluări
- Low 2018Document9 paginiLow 2018Hendri WahyudiÎncă nu există evaluări
- Evidence-Based Management of Acute Lung Injury and Acute Respiratory Distress SyndromeDocument17 paginiEvidence-Based Management of Acute Lung Injury and Acute Respiratory Distress SyndromeretÎncă nu există evaluări
- Comment: See Page E218Document2 paginiComment: See Page E218BBD BBDÎncă nu există evaluări
- Pi Is 0885392410001600Document8 paginiPi Is 0885392410001600AzarudeenÎncă nu există evaluări
- Vant HultDocument6 paginiVant HultQuel PaivaÎncă nu există evaluări
- Advances in The Support of Respiratory FailureDocument7 paginiAdvances in The Support of Respiratory FailureFabio RepettoÎncă nu există evaluări
- BMJ Open 2015 ZhangDocument10 paginiBMJ Open 2015 ZhangLuis CordovaÎncă nu există evaluări
- Roberts 2019 Year in Review Adult Invasive MechDocument6 paginiRoberts 2019 Year in Review Adult Invasive MechJose Luis Escobar zabaleguiÎncă nu există evaluări
- Rodrigo S (2020)Document8 paginiRodrigo S (2020)Awaluddin Andhy MÎncă nu există evaluări
- Airway Clearance DysfunctionDocument27 paginiAirway Clearance Dysfunctionane2saÎncă nu există evaluări
- Acute Medicine Surgery - 2024 - Hoshino - Future Directions of Lung Protective Ventilation Strategies in AcuteDocument8 paginiAcute Medicine Surgery - 2024 - Hoshino - Future Directions of Lung Protective Ventilation Strategies in AcuteDiego AzevedoÎncă nu există evaluări
- Zampieri 2019Document8 paginiZampieri 2019Peter AgabaÎncă nu există evaluări
- Airway Clearance Techniques For Patients With Acute Exacerbations of Chronic Obstructive Pulmonary Disease: Physical Therapy Practice in SwedenDocument8 paginiAirway Clearance Techniques For Patients With Acute Exacerbations of Chronic Obstructive Pulmonary Disease: Physical Therapy Practice in SwedenEva FisioÎncă nu există evaluări
- Noninvasive Ventilation For Patients Presenting With Acute Respiratory Failure: The Randomized Controlled TrialsDocument11 paginiNoninvasive Ventilation For Patients Presenting With Acute Respiratory Failure: The Randomized Controlled TrialsCesar C SÎncă nu există evaluări
- Symptomatic Patients Without Airflow Obstruction2016Document4 paginiSymptomatic Patients Without Airflow Obstruction2016Ella EllaÎncă nu există evaluări
- Severe Asthma in Primary Care: Identification and ManagementDocument8 paginiSevere Asthma in Primary Care: Identification and ManagementIzza UrfanÎncă nu există evaluări
- Cap AsmaDocument10 paginiCap AsmaAuliaÎncă nu există evaluări
- Bronchial Asthma Research PaperDocument6 paginiBronchial Asthma Research Paperniisexgkf100% (1)
- Cardiopulmonary Laboratory Biomarkers in The Evaluation of Acute Dyspnea - Open Acces Emerg Med 2016Document11 paginiCardiopulmonary Laboratory Biomarkers in The Evaluation of Acute Dyspnea - Open Acces Emerg Med 2016ErnestoÎncă nu există evaluări
- AsmathDocument6 paginiAsmathRido SaputraÎncă nu există evaluări
- Managing Breathlessness: A Palliative Care Approach: Chloe Chin, Sara BoothDocument9 paginiManaging Breathlessness: A Palliative Care Approach: Chloe Chin, Sara BoothRitu ShewaniÎncă nu există evaluări
- The Acute Respiratory Distress Syndrome in 2013: Review Open AccessDocument6 paginiThe Acute Respiratory Distress Syndrome in 2013: Review Open Accessindriyanti natasya ayu utami kottenÎncă nu există evaluări
- Symptomatic Treatment of Cough Among Adult Patients With Lung Cancer CHEST Guideline and Expert Panel ReportDocument14 paginiSymptomatic Treatment of Cough Among Adult Patients With Lung Cancer CHEST Guideline and Expert Panel ReportThaísa NogueiraÎncă nu există evaluări
- Dasenbrook higherPEEP 11 PrintedDocument8 paginiDasenbrook higherPEEP 11 PrintedОлег СатишурÎncă nu există evaluări
- ALI and ARDS - Challenges and Advances - An Issue of Critical Care ClinicsDocument324 paginiALI and ARDS - Challenges and Advances - An Issue of Critical Care ClinicsOanamikaela VaidaÎncă nu există evaluări
- Acuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiesDocument16 paginiAcuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiessamuelÎncă nu există evaluări
- Mechanical Ventilation - Lessons From The ARDSNet TrialDocument5 paginiMechanical Ventilation - Lessons From The ARDSNet TrialRDG20202Încă nu există evaluări
- Adaptive Support Ventilation From Intubation To ExDocument2 paginiAdaptive Support Ventilation From Intubation To ExIvulik87Încă nu există evaluări
- Accepted Manuscript: Paediatric Respiratory ReviewsDocument16 paginiAccepted Manuscript: Paediatric Respiratory ReviewsAlvaro Guillen CerpaÎncă nu există evaluări
- Overview of Common Causes of Chronic Cough: ACCP Evidence-Based Clinical Practice GuidelinesDocument4 paginiOverview of Common Causes of Chronic Cough: ACCP Evidence-Based Clinical Practice GuidelineschuckyonfireÎncă nu există evaluări
- Clinical Translational All - 2013 - L Tvall - Asthma Control Emergency Visits Lung Function and FENO in Asthma andDocument1 paginăClinical Translational All - 2013 - L Tvall - Asthma Control Emergency Visits Lung Function and FENO in Asthma andFuerza Dedicacion OmegaÎncă nu există evaluări
- ExtubationDocument7 paginiExtubationbalab2311Încă nu există evaluări
- Pharmacologictreatments Foracuterespiratory DistresssyndromeDocument17 paginiPharmacologictreatments Foracuterespiratory DistresssyndromeLuis HernándezÎncă nu există evaluări
- Asthma Thesis PDFDocument5 paginiAsthma Thesis PDFmichellejohnsoncharleston100% (2)
- Long Term Management of Obstructive Sleep Apnea AnDocument9 paginiLong Term Management of Obstructive Sleep Apnea AnsukiyantoÎncă nu există evaluări
- Atsc 2011 Niv 03Document12 paginiAtsc 2011 Niv 03Silvermist EiceliÎncă nu există evaluări
- The Answer For Inhaled Antibiotics in Pneumonia IsDocument3 paginiThe Answer For Inhaled Antibiotics in Pneumonia IsEnrique JaraÎncă nu există evaluări
- Practice Guidelines: ACCP Releases Statement On Dyspnea Treatment in Patients With Advanced Lung or Heart DiseaseDocument2 paginiPractice Guidelines: ACCP Releases Statement On Dyspnea Treatment in Patients With Advanced Lung or Heart DiseaseSartini Roma Dame NainggolanÎncă nu există evaluări
- (PULMO) 2012 ARDS - The New Berlin DefinitionDocument4 pagini(PULMO) 2012 ARDS - The New Berlin DefinitionerikaÎncă nu există evaluări
- Non-Invasive Positive Pressure Ventilation in Acute Respiratory Failure: Providing Competent CareDocument9 paginiNon-Invasive Positive Pressure Ventilation in Acute Respiratory Failure: Providing Competent CareAndana TrisaviÎncă nu există evaluări
- Evidence Based SearchDocument5 paginiEvidence Based SearchGluteus MAXÎncă nu există evaluări
- As 2Document11 paginiAs 2Patrick SteinbergÎncă nu există evaluări
- Copd 10 1703Document7 paginiCopd 10 1703Maria Camila SanabriaÎncă nu există evaluări
- Hfo 2Document9 paginiHfo 2markus_danusantosoÎncă nu există evaluări
- European Respiratory Society Guidelines For The Diagnosis of Asthma in AdultsDocument25 paginiEuropean Respiratory Society Guidelines For The Diagnosis of Asthma in AdultsLee Foo WengÎncă nu există evaluări
- Alveolar Recruitment Maneuvers Under General AnesthesiaDocument12 paginiAlveolar Recruitment Maneuvers Under General AnesthesiaBetzaBarriosÎncă nu există evaluări
- Less Is More in Mechanical Ventilation, LGattinoniDocument3 paginiLess Is More in Mechanical Ventilation, LGattinoniErnesto De HaroÎncă nu există evaluări
- Resp Emer in ChildrenDocument35 paginiResp Emer in ChildrenvgmanjunathÎncă nu există evaluări
- Diagnosis and Treatment of Chronic CoughDe la EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoÎncă nu există evaluări
- Spondylolisthesis PDFDocument121 paginiSpondylolisthesis PDFishak_alsophÎncă nu există evaluări
- Absent Architectures: Post-War Housing in British Children's Picture Books (1960-Present)Document26 paginiAbsent Architectures: Post-War Housing in British Children's Picture Books (1960-Present)Novy DitaÎncă nu există evaluări
- Jospt 2009 2857Document11 paginiJospt 2009 2857Novy DitaÎncă nu există evaluări
- Infrared RadiationDocument226 paginiInfrared RadiationhackÎncă nu există evaluări
- Knee Orthopedic TestsDocument47 paginiKnee Orthopedic Testsnnick0Încă nu există evaluări
- Physical Therapy in Sport: Book ReviewDocument1 paginăPhysical Therapy in Sport: Book ReviewNovy DitaÎncă nu există evaluări
- Ijspt 06 241 PDFDocument13 paginiIjspt 06 241 PDFNovy DitaÎncă nu există evaluări
- Icf Core Set For Os To ArthritisDocument5 paginiIcf Core Set For Os To ArthritisNovy DitaÎncă nu există evaluări
- TCD - 207 Operating Board For Back-Side SUB Run Communication Error (Err - Rear - Sub)Document1 paginăTCD - 207 Operating Board For Back-Side SUB Run Communication Error (Err - Rear - Sub)Daniel GatdulaÎncă nu există evaluări
- Bank Details and Payment MethodsDocument1 paginăBank Details and Payment Methodsetrit0% (1)
- MT7605B DSDocument7 paginiMT7605B DSVishal dtuÎncă nu există evaluări
- Learning Dynamics and Vibrations by MSC AdamsDocument80 paginiLearning Dynamics and Vibrations by MSC AdamsFrancuzzo DaniliÎncă nu există evaluări
- Apayao Quickstat: Indicator Reference Period and DataDocument4 paginiApayao Quickstat: Indicator Reference Period and DataLiyan CampomanesÎncă nu există evaluări
- Cameron Residences - Official Project Brief - 080719Document47 paginiCameron Residences - Official Project Brief - 080719neil dÎncă nu există evaluări
- CTA Case Digests - 07.23.2021Document5 paginiCTA Case Digests - 07.23.2021Emrico CabahugÎncă nu există evaluări
- Rules and Regulations Governing Private Schools in Basic Education - Part 2Document103 paginiRules and Regulations Governing Private Schools in Basic Education - Part 2Jessah SuarezÎncă nu există evaluări
- Gendex 9200 enDocument204 paginiGendex 9200 enArturo Jimenez Terrero80% (5)
- 2019 Specimen Paper 3 Mark SchemeDocument6 pagini2019 Specimen Paper 3 Mark SchemeProjeck HendraÎncă nu există evaluări
- Appointments & Other Personnel Actions Submission, Approval/Disapproval of AppointmentDocument7 paginiAppointments & Other Personnel Actions Submission, Approval/Disapproval of AppointmentZiiee BudionganÎncă nu există evaluări
- Accounting QuestionsDocument16 paginiAccounting QuestionsPrachi ChananaÎncă nu există evaluări
- Financial Ratio Analysis FormulasDocument4 paginiFinancial Ratio Analysis FormulasVaishali Jhaveri100% (1)
- Formal Methods Assignment PDFDocument25 paginiFormal Methods Assignment PDFAdla FikriyahÎncă nu există evaluări
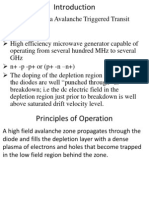
- Trapatt ModeDocument30 paginiTrapatt Modebchaitanya_555100% (1)
- Flexible, Dynamic VR Simulation of A Future River Lock Facilitates Prevention Through Design in Occupational Safety and HealthDocument2 paginiFlexible, Dynamic VR Simulation of A Future River Lock Facilitates Prevention Through Design in Occupational Safety and HealthEdgar Alexander Hurtado MolochoÎncă nu există evaluări
- COEN 252 Computer Forensics: Incident ResponseDocument39 paginiCOEN 252 Computer Forensics: Incident ResponseDudeviswaÎncă nu există evaluări
- CV - Oscar ChampionDocument3 paginiCV - Oscar ChampionKarina Gamarra NinaÎncă nu există evaluări
- Transportation Problem 2Document11 paginiTransportation Problem 2Chasity WrightÎncă nu există evaluări
- Report On PesoDocument10 paginiReport On PesoAerish RioverosÎncă nu există evaluări
- Java 9 Real - TimeDocument57 paginiJava 9 Real - TimeDiego AmayaÎncă nu există evaluări
- 3 Filtration Lecture NotesDocument16 pagini3 Filtration Lecture NotesRuben SIbayanÎncă nu există evaluări
- Safety Manual For DumperDocument9 paginiSafety Manual For DumperHimanshu Bhushan100% (1)
- 5 GR No. 93468 December 29, 1994 NATU Vs TorresDocument9 pagini5 GR No. 93468 December 29, 1994 NATU Vs Torresrodolfoverdidajr100% (1)
- ''Adhibeo'' in LatinDocument5 pagini''Adhibeo'' in LatinThriw100% (1)
- 01 FundamentalsDocument20 pagini01 FundamentalsTay KittithatÎncă nu există evaluări
- AWS Solution Architect SampleDocument3 paginiAWS Solution Architect SamplepandiecÎncă nu există evaluări
- Advancing An Essential Clinical Data Set in Canada InfographicDocument1 paginăAdvancing An Essential Clinical Data Set in Canada InfographicNICHAEL MARIA CELINA UYÎncă nu există evaluări
- From 1-73Document95 paginiFrom 1-73Shrijan ChapagainÎncă nu există evaluări
- UTAR Convocation Checklist For Graduands Attending Convocation (March 2019) - 1Document5 paginiUTAR Convocation Checklist For Graduands Attending Convocation (March 2019) - 1JoyleeeeeÎncă nu există evaluări