S-ar putea să vă placă și
- The Leg: - Orthopedic Anatomy - Clinical Anatomy - Radiologic AnatomyDocument50 paginiThe Leg: - Orthopedic Anatomy - Clinical Anatomy - Radiologic Anatomyspeedy.catÎncă nu există evaluări
- Specific Nerve Injuries To The Lower ExtremitiesDocument2 paginiSpecific Nerve Injuries To The Lower Extremitieskimwell samsonÎncă nu există evaluări
- B15 M4 - Sports Injury (Dr. W. Mana-Ay 2014)Document8 paginiB15 M4 - Sports Injury (Dr. W. Mana-Ay 2014)Dakila Vine VillanÎncă nu există evaluări
- Normal and Abnormal Spontaneous ActivityDocument23 paginiNormal and Abnormal Spontaneous ActivityLuís PachecoÎncă nu există evaluări
- Anterior Interosseous Nerve Paralysis Due To Gantzer's MuscleDocument3 paginiAnterior Interosseous Nerve Paralysis Due To Gantzer's MuscleJunji Miller FukuyamaÎncă nu există evaluări
- IT acupuncture band treatmentDocument5 paginiIT acupuncture band treatmentVita MishtiiÎncă nu există evaluări
- Mri Artifacts FinalDocument44 paginiMri Artifacts FinalSunny SbaÎncă nu există evaluări
- 104 - Neurology Physiology) Spinal Cord - Golgi Tendon Organ Reflex (GTO)Document3 pagini104 - Neurology Physiology) Spinal Cord - Golgi Tendon Organ Reflex (GTO)Nikki Lin LiuÎncă nu există evaluări
- Arytenoid Dislocation: A New Diagnostic and Treatment ApproachDocument2 paginiArytenoid Dislocation: A New Diagnostic and Treatment ApproachChrisÎncă nu există evaluări
- OrtoDocument4 paginiOrtoLuís CorreiaÎncă nu există evaluări
- Ankle Joint and Ligament AnatomyDocument5 paginiAnkle Joint and Ligament AnatomyHafizah HoshniÎncă nu există evaluări
- P11. Retikularna Formacija I Ekstratalamički Aferentni Sustavi Moždane Kore P12. Opće Moždane Funkcije: EEG I Evocirani PotencijaliDocument119 paginiP11. Retikularna Formacija I Ekstratalamički Aferentni Sustavi Moždane Kore P12. Opće Moždane Funkcije: EEG I Evocirani PotencijaliGoran SimicÎncă nu există evaluări
- Rehabilitation Guidelines For Hip Arthroscopy Procedures: Figure 1 Hip Joint (Opened) Lateral ViewDocument8 paginiRehabilitation Guidelines For Hip Arthroscopy Procedures: Figure 1 Hip Joint (Opened) Lateral ViewDevi MigiekaÎncă nu există evaluări
- Modern CircuitDocument28 paginiModern Circuitمركز ريلاكس للعلاج الطبيعيÎncă nu există evaluări
- Spinal Orthoses: Type Examples Motion Restriction Indications NotesDocument2 paginiSpinal Orthoses: Type Examples Motion Restriction Indications NotesBD BesorioÎncă nu există evaluări
- Normal and Pathologic Peroneal Nerve On Routine MRI of The KneeDocument32 paginiNormal and Pathologic Peroneal Nerve On Routine MRI of The KneeCaitlynÎncă nu există evaluări
- Epi-Perineurial Anatomy, Innervation, and Axonal Nociceptive MechanismsDocument6 paginiEpi-Perineurial Anatomy, Innervation, and Axonal Nociceptive MechanismsPedro FonsecaÎncă nu există evaluări
- Posterior Interosseus Palsy With An Incidental Froment-Rauber Nerve Presenting As Pseudoclaw HandDocument5 paginiPosterior Interosseus Palsy With An Incidental Froment-Rauber Nerve Presenting As Pseudoclaw Handemilio9fernandez9gatÎncă nu există evaluări
- Anatomy Lower LimbDocument120 paginiAnatomy Lower LimbVn Dang100% (3)
- Thorax and Abdomen Muscle NotesDocument2 paginiThorax and Abdomen Muscle NotesJean OpallaÎncă nu există evaluări
- Changes in Low Back Pain in A Long DistanceDocument4 paginiChanges in Low Back Pain in A Long Distancedaniela cubillos escobarÎncă nu există evaluări
- Physical Rehabilitation 2.2 Rehabilitation of Lower Limb Musculoskeletal DisordersDocument6 paginiPhysical Rehabilitation 2.2 Rehabilitation of Lower Limb Musculoskeletal DisordersJAIRISH YZABELLE SALVADORÎncă nu există evaluări
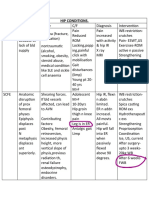
- HIP CONDITIONS GUIDEDocument2 paginiHIP CONDITIONS GUIDEseemaÎncă nu există evaluări
- Examination of The HipDocument33 paginiExamination of The HipTumbal BroÎncă nu există evaluări
- Lecture Outline Q's 206Document3 paginiLecture Outline Q's 206Mina TadrosÎncă nu există evaluări
- Electrodiagnostic in Sciatica NeuropathyDocument37 paginiElectrodiagnostic in Sciatica NeuropathyRizka_aprilÎncă nu există evaluări
- REFLEXESDocument15 paginiREFLEXESSonali Soumyashree100% (2)
- NeuroscienceDocument5 paginiNeuroscienceChing MacarubboÎncă nu există evaluări
- 4 - Motor SystemDocument20 pagini4 - Motor SystemAliÎncă nu există evaluări
- Cranial Nerves in Health and Disease (2nd Edition) - (XI. Accessory Nerve)Document11 paginiCranial Nerves in Health and Disease (2nd Edition) - (XI. Accessory Nerve)Pierre PradelÎncă nu există evaluări
- Tendon TransferDocument6 paginiTendon TransferMd Ahsanuzzaman PinkuÎncă nu există evaluări
- Tollin-2005-Interaural Phase andDocument10 paginiTollin-2005-Interaural Phase andCabinet VeterinarÎncă nu există evaluări
- Riche-Cannieu Anastomosis With Partial Transection of The Median NerveDocument3 paginiRiche-Cannieu Anastomosis With Partial Transection of The Median NerveAdam L. SchreiberÎncă nu există evaluări
- Herpes Zoster-Predicting and Minimizing The Impact of Post-Herpetic NeuralgiaDocument8 paginiHerpes Zoster-Predicting and Minimizing The Impact of Post-Herpetic NeuralgiaDevi DamayantiÎncă nu există evaluări
- 10.3) Lower Extremity - Ankle & FootDocument9 pagini10.3) Lower Extremity - Ankle & FootDION ANN SAYSONÎncă nu există evaluări
- UseofMulliganSNAGs PDFDocument1 paginăUseofMulliganSNAGs PDFMestereaga AlinÎncă nu există evaluări
- 10.1) Lower Extremity - HipDocument7 pagini10.1) Lower Extremity - HipDION ANN SAYSONÎncă nu există evaluări
- Brain Activity - Cortical Evoked Potent To An Auditory Illus, Binaural BeatsDocument23 paginiBrain Activity - Cortical Evoked Potent To An Auditory Illus, Binaural BeatsCarlos SilvaÎncă nu există evaluări
- Exercise 1: Problems)Document8 paginiExercise 1: Problems)api-479717740Încă nu există evaluări
- ElectromyographyDocument54 paginiElectromyographymohanprasannaÎncă nu există evaluări
- Orthopaedics FinalDocument124 paginiOrthopaedics Finaldbchoudhary77Încă nu există evaluări
- The Enthesis Organ Concept - Why Enthesopathies May Not Present As Focal Insertional Disorders. Arthritis & Rheumatism 2004Document8 paginiThe Enthesis Organ Concept - Why Enthesopathies May Not Present As Focal Insertional Disorders. Arthritis & Rheumatism 2004micamart.94Încă nu există evaluări
- Physiology OSPEDocument19 paginiPhysiology OSPEzephyrverliceÎncă nu există evaluări
- Auditory Brainstem ResponseDocument18 paginiAuditory Brainstem ResponseFree dataÎncă nu există evaluări
- Open Inguinal Hernia Repair Lichtenstein CadaverDocument9 paginiOpen Inguinal Hernia Repair Lichtenstein CadaverTeja Laksana NukanaÎncă nu există evaluări
- 吳易澄-花蓮2023-04-16 AnkleDocument36 pagini吳易澄-花蓮2023-04-16 AnkletsungyuchiÎncă nu există evaluări
- Saphenous Nerve EntrapmentDocument2 paginiSaphenous Nerve Entrapmentemilio9fernandez9gatÎncă nu există evaluări
- Telaah 1Document3 paginiTelaah 1anri albarruÎncă nu există evaluări
- Medscape Neurophysiological MonitoringDocument10 paginiMedscape Neurophysiological MonitoringTomagratchÎncă nu există evaluări
- Refleks ArcsDocument34 paginiRefleks Arcskiedd_04100% (1)
- Biomechanics-Lumbar Facet Pain Biomechanics, Neuroanatomy and NeurophysiologyDocument13 paginiBiomechanics-Lumbar Facet Pain Biomechanics, Neuroanatomy and NeurophysiologyMuhammad FahmyÎncă nu există evaluări
- Luke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Document3 paginiLuke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Tyler Lawrence CoyeÎncă nu există evaluări
- Clinicals of NeuroanatomyDocument9 paginiClinicals of Neuroanatomyaneeqahmed99Încă nu există evaluări
- Urooj MergedDocument14 paginiUrooj MergedkashafÎncă nu există evaluări
- Journal of Orthopaedics: B.T. Pushpa, Siddharth N. Aiyer, Muhil Kannan, Anupama Maheswaran, S. RajasekaranDocument2 paginiJournal of Orthopaedics: B.T. Pushpa, Siddharth N. Aiyer, Muhil Kannan, Anupama Maheswaran, S. RajasekaranmohÎncă nu există evaluări
- Peripheral Neuropathy Clinical ApproachDocument19 paginiPeripheral Neuropathy Clinical ApproachNur Nadzifah Zainal AbidinÎncă nu există evaluări
- United Neurodiagnostic Professionals of America - EMG and Evoked Potentials in The Operating Room During Spinal SurgeryDocument12 paginiUnited Neurodiagnostic Professionals of America - EMG and Evoked Potentials in The Operating Room During Spinal SurgeryShauki AliÎncă nu există evaluări
- Lower Extremity Anatomy: Sari Tri Yulianti, S.FT., M.BiomedDocument73 paginiLower Extremity Anatomy: Sari Tri Yulianti, S.FT., M.BiomedDindaÎncă nu există evaluări
- Elbow & Hand Clinical ConditionsDocument7 paginiElbow & Hand Clinical ConditionsPhoebe DemegilloÎncă nu există evaluări
- Transcutaneous Electrical Nerve Stimulation (TENS) For Pain Relief: Electrode Placement Atlas(2018 editon)De la EverandTranscutaneous Electrical Nerve Stimulation (TENS) For Pain Relief: Electrode Placement Atlas(2018 editon)Evaluare: 5 din 5 stele5/5 (4)
- Intra-Vena Immunoglobulin Treatment and Prognosis in Guillain-Barre SyndromeDocument32 paginiIntra-Vena Immunoglobulin Treatment and Prognosis in Guillain-Barre Syndromesatyagraha84Încă nu există evaluări
- Dr. Djohan Ardiansyah, SP.S (K)Document60 paginiDr. Djohan Ardiansyah, SP.S (K)satyagraha84Încă nu există evaluări
- WWW - Stroke.nih - Gov: Stroke Strikes Fast. You Should TooDocument4 paginiWWW - Stroke.nih - Gov: Stroke Strikes Fast. You Should Toosatyagraha84Încă nu există evaluări
- Vecchie T 1997Document18 paginiVecchie T 1997satyagraha84Încă nu există evaluări
- Overview Guillain Barre Syndrome Update, What Should We KnowDocument39 paginiOverview Guillain Barre Syndrome Update, What Should We Knowsatyagraha84Încă nu există evaluări
- GCS Assessment Aid BahasaDocument51 paginiGCS Assessment Aid BahasaLulu MafrudhotulÎncă nu există evaluări
- European Stroke Organisation Recommendations To Establish A Stroke Unit and Stroke CenterDocument13 paginiEuropean Stroke Organisation Recommendations To Establish A Stroke Unit and Stroke Centersatyagraha84Încă nu există evaluări
- CLINICAL PRESENTATION AND DIAGNOSIS OF GLIOMADocument60 paginiCLINICAL PRESENTATION AND DIAGNOSIS OF GLIOMAsatyagraha84Încă nu există evaluări
- Use of Aed in Hepatic and Renal DsDocument16 paginiUse of Aed in Hepatic and Renal Dssatyagraha84Încă nu există evaluări
- Piriformis Pyomyositis, An Unusual Presentation of Leg Pain Post Partum Case Report and Review of LiteratureDocument4 paginiPiriformis Pyomyositis, An Unusual Presentation of Leg Pain Post Partum Case Report and Review of Literaturesatyagraha84Încă nu există evaluări
- Stroke Unit Position Paper FINALDocument4 paginiStroke Unit Position Paper FINALsatyagraha84Încă nu există evaluări
- STROKE UNITS AND CAREDocument8 paginiSTROKE UNITS AND CAREsatyagraha84Încă nu există evaluări
- Windows PC: Appendix 1 EMG Lecture With LIVE SOUNDS How To Use The DVD-ROMDocument4 paginiWindows PC: Appendix 1 EMG Lecture With LIVE SOUNDS How To Use The DVD-ROMsatyagraha84Încă nu există evaluări
- Nervous System Phisiology of Nervous Tissues. SynapsesDocument65 paginiNervous System Phisiology of Nervous Tissues. Synapsessatyagraha84Încă nu există evaluări
- Correction: (Stroke. 2018 49:e233-E234. DOI: 10.1161/STR.0000000000000172.) DOI: 10.1161/STR.0000000000000172Document2 paginiCorrection: (Stroke. 2018 49:e233-E234. DOI: 10.1161/STR.0000000000000172.) DOI: 10.1161/STR.0000000000000172satyagraha84Încă nu există evaluări
- ATT00001Document1 paginăATT00001satyagraha84Încă nu există evaluări
- Serial Sampling of Serum Protein Biomarkers For Monitoring Human Traumatic Brain Injury Dynamics: A Systematic ReviewDocument23 paginiSerial Sampling of Serum Protein Biomarkers For Monitoring Human Traumatic Brain Injury Dynamics: A Systematic Reviewsatyagraha84Încă nu există evaluări
- Handbook of Pain Management PDFDocument105 paginiHandbook of Pain Management PDFsatyagraha84Încă nu există evaluări
- Consensus ETON 1Document7 paginiConsensus ETON 1satyagraha84Încă nu există evaluări
- Prospective Evaluation of Visual Function For Early Detection of Ethambutol ToxicityDocument5 paginiProspective Evaluation of Visual Function For Early Detection of Ethambutol Toxicitysatyagraha84Încă nu există evaluări
- Drug-Induced Peripheral NeuropathyDocument8 paginiDrug-Induced Peripheral Neuropathysatyagraha84Încă nu există evaluări
- Registrasi Ulang10Document5 paginiRegistrasi Ulang10satyagraha84Încă nu există evaluări
- Ijms 16 11903Document63 paginiIjms 16 11903satyagraha84Încă nu există evaluări
- Continuous Pulse Oximetry in Acute Hemiparetic StrokeDocument5 paginiContinuous Pulse Oximetry in Acute Hemiparetic Strokesatyagraha84Încă nu există evaluări
- Toxic NeuropathiesDocument11 paginiToxic Neuropathiessatyagraha84Încă nu există evaluări
- VA/DoD mTBI Guideline Updates Diagnosis and TreatmentDocument133 paginiVA/DoD mTBI Guideline Updates Diagnosis and Treatmentsatyagraha84Încă nu există evaluări
- Medication, Toxic, and Vitamin-Related NeuropathiesDocument22 paginiMedication, Toxic, and Vitamin-Related Neuropathiessatyagraha84Încă nu există evaluări
- Clinical Evaluation and Treatment of Transverse MyelitisDocument57 paginiClinical Evaluation and Treatment of Transverse MyelitisAlexandre VieiraÎncă nu există evaluări
- Brainsci 07 00142Document11 paginiBrainsci 07 00142satyagraha84Încă nu există evaluări
- Schools of PsychologyDocument30 paginiSchools of PsychologyMdl C DayritÎncă nu există evaluări
- Intro - New Covenant TheologyDocument15 paginiIntro - New Covenant TheologyDavid SalazarÎncă nu există evaluări
- Zen and The Art of Trumpet Play - Mark Van CleaveDocument55 paginiZen and The Art of Trumpet Play - Mark Van Cleavesz.sledz100% (1)
- 05 Mesina v. PeopleDocument7 pagini05 Mesina v. PeopleJason ToddÎncă nu există evaluări
- Fundamentals of Human Neuropsychology 7th Edition Kolb Test BankDocument26 paginiFundamentals of Human Neuropsychology 7th Edition Kolb Test BankDanielYoungabrn100% (60)
- # Law and MoralityDocument16 pagini# Law and MoralityBRYAN LING PING YEE UnknownÎncă nu există evaluări
- Work Breakdown StructureDocument3 paginiWork Breakdown StructureEllie Annelle LazaroÎncă nu există evaluări
- Who May Apply Under Article 32: Article 32 and Article 226 Comparative StudyDocument2 paginiWho May Apply Under Article 32: Article 32 and Article 226 Comparative StudySai Malavika TuluguÎncă nu există evaluări
- Ethics Lecture Notes For Academic Year - Situation 1 Your Family Is An Exclusive Vacation On A - StuDocuDocument1 paginăEthics Lecture Notes For Academic Year - Situation 1 Your Family Is An Exclusive Vacation On A - StuDocuRaveine JabatÎncă nu există evaluări
- Yu-Gi-Oh Nightmare Troubadour InfoDocument12 paginiYu-Gi-Oh Nightmare Troubadour InfoBrandon Bradley0% (1)
- Two Sides of Effective Oral CommunicationDocument17 paginiTwo Sides of Effective Oral CommunicationSharath KumarÎncă nu există evaluări
- Sample Thesis Title in Business ManagementDocument6 paginiSample Thesis Title in Business Managementlisabrownomaha100% (2)
- Aprils Detox GuideDocument20 paginiAprils Detox GuideKwasi BempongÎncă nu există evaluări
- PSM641UX TechnicalManua-V1.03Document128 paginiPSM641UX TechnicalManua-V1.03arulsethuÎncă nu există evaluări
- Biosimilars: Pros and Cons in Current Practice: MBBS, MRCP (Uk), FRCP (Edin), FamsDocument51 paginiBiosimilars: Pros and Cons in Current Practice: MBBS, MRCP (Uk), FRCP (Edin), FamshoneyworksÎncă nu există evaluări
- Activity 6 - Autograph BingoDocument1 paginăActivity 6 - Autograph Bingoapi-277504884Încă nu există evaluări
- Bolomeya Model For Normal Concrete Mix DesignDocument6 paginiBolomeya Model For Normal Concrete Mix DesignprincessrandotaÎncă nu există evaluări
- Gajendra-Moksha HTMLDocument7 paginiGajendra-Moksha HTMLankitÎncă nu există evaluări
- Project Report - Campus ConnectDocument19 paginiProject Report - Campus ConnectruchiyaÎncă nu există evaluări
- R209292y@students Msu Ac ZWDocument7 paginiR209292y@students Msu Ac ZWColias DubeÎncă nu există evaluări
- Accounting Knowledge N SkillDocument17 paginiAccounting Knowledge N SkillNur HidayahÎncă nu există evaluări
- Life Cycle of A BirdDocument3 paginiLife Cycle of A BirdMary Grace YañezÎncă nu există evaluări
- Daily Aspirin Therapy Understand The Benefits and RisksDocument5 paginiDaily Aspirin Therapy Understand The Benefits and RisksNicholas OwensÎncă nu există evaluări
- 1 Unpacking The SelfDocument13 pagini1 Unpacking The SelfJEMABEL SIDAYENÎncă nu există evaluări
- Tanada, Et Al. Vs Angara, Et Al., 272 SCRA 18, GR 118295 (May 2, 1997)Document3 paginiTanada, Et Al. Vs Angara, Et Al., 272 SCRA 18, GR 118295 (May 2, 1997)Lu CasÎncă nu există evaluări
- ML for Humans: A Journey from Ignorance to OxfordDocument27 paginiML for Humans: A Journey from Ignorance to OxfordDivyanshu Sachan50% (2)
- Cunningham S Book of Shadows PDFDocument258 paginiCunningham S Book of Shadows PDFAngela C. Allen100% (10)
- scn625 Summativeeval SarahltDocument6 paginiscn625 Summativeeval Sarahltapi-644817377Încă nu există evaluări
- SPELD SA A Trip To The Top End-DSDocument16 paginiSPELD SA A Trip To The Top End-DSThien Tho NguyenÎncă nu există evaluări
- EnHanced4 WB KeyDocument293 paginiEnHanced4 WB Keyezzeldin3khater100% (2)