S-ar putea să vă placă și
- Archive of SIDDocument5 paginiArchive of SIDEdy Anugrah PutraÎncă nu există evaluări
- Skin Graft: Technique, Indications and OutcomesDocument9 paginiSkin Graft: Technique, Indications and OutcomesIJAR JOURNALÎncă nu există evaluări
- Canalplasty For Exostosis With Maximal Skin PreservationDocument9 paginiCanalplasty For Exostosis With Maximal Skin PreservationAbegail LacsonÎncă nu există evaluări
- 59 Ijmrp 4 (4) 256-60Document5 pagini59 Ijmrp 4 (4) 256-60SK BONE & JOINT CARE DPIÎncă nu există evaluări
- Surgical Enucleation of Corn A Novel TechniqueDocument2 paginiSurgical Enucleation of Corn A Novel TechniqueRohit KumarÎncă nu există evaluări
- 2014 Article 1741Document4 pagini2014 Article 1741anton suponoÎncă nu există evaluări
- 3541 14379 2 PBDocument8 pagini3541 14379 2 PBCraj RajÎncă nu există evaluări
- Is Mesh Always Necessary in Every Small UmbilicalDocument8 paginiIs Mesh Always Necessary in Every Small UmbilicalLeonardo RibeiroÎncă nu există evaluări
- Modified Technique of Underlay Myringoplasty: Journal of Otolaryngology-ENT ResearchDocument4 paginiModified Technique of Underlay Myringoplasty: Journal of Otolaryngology-ENT ResearchAkanshaÎncă nu există evaluări
- Diastemma ClosureDocument3 paginiDiastemma Closureisha sajjanharÎncă nu există evaluări
- Zingaretti Et Al. 2019Document5 paginiZingaretti Et Al. 2019Walid SasiÎncă nu există evaluări
- The Advantages of External DR PDFDocument13 paginiThe Advantages of External DR PDFalitÎncă nu există evaluări
- Clinical Study: Vacuum Assisted Closure Therapy Versus Standard Wound Therapy For Open Musculoskeletal InjuriesDocument9 paginiClinical Study: Vacuum Assisted Closure Therapy Versus Standard Wound Therapy For Open Musculoskeletal InjuriesAndika FahruroziÎncă nu există evaluări
- 논문원문Document4 pagini논문원문Donghee LeeÎncă nu există evaluări
- Mathieu2020 Soft Tissue Reconstruction in The Leg by Orthopedic Surgeons Practices at An African Trauma CenterDocument5 paginiMathieu2020 Soft Tissue Reconstruction in The Leg by Orthopedic Surgeons Practices at An African Trauma CenterThach Nguyen NgocÎncă nu există evaluări
- Medip, ISJ-2381 ODocument6 paginiMedip, ISJ-2381 OmarvinmtcirujanoÎncă nu există evaluări
- Brief Communication: Nitin Mokal, Navdeep ChavanDocument4 paginiBrief Communication: Nitin Mokal, Navdeep ChavanANOOP HANDAÎncă nu există evaluări
- Original Article: AbstractDocument3 paginiOriginal Article: AbstractMarco Antonio MiraveteÎncă nu există evaluări
- A Comparative Study of N-Butyl Cyanoacrylate and Conventional Silk Sutures in The Closure of Intra Oral Incisions After Modified CorticotomyPeizocisionDocument10 paginiA Comparative Study of N-Butyl Cyanoacrylate and Conventional Silk Sutures in The Closure of Intra Oral Incisions After Modified CorticotomyPeizocisionInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Post-Operative Complications of Periodontal SurgeryDocument2 paginiPost-Operative Complications of Periodontal SurgeryReshmaa RajendranÎncă nu există evaluări
- Basic Suture Techniques For Oral MucosaDocument12 paginiBasic Suture Techniques For Oral MucosaNurul Hanifah100% (1)
- Acfs 2021 00297Document10 paginiAcfs 2021 00297이호원Încă nu există evaluări
- Using Diode Laser For Soft Tissue Incision of Oral Cavity: Case ReportDocument8 paginiUsing Diode Laser For Soft Tissue Incision of Oral Cavity: Case ReportAndhika GilangÎncă nu există evaluări
- OMX Volume 12 Issue 1 Pages 14-20Document7 paginiOMX Volume 12 Issue 1 Pages 14-20JyothishÎncă nu există evaluări
- Shoelace Techni e For Delayed Primary Closure of FasciotomiesDocument2 paginiShoelace Techni e For Delayed Primary Closure of FasciotomiesMiguel Angel Lamas RamirezÎncă nu există evaluări
- Bone-Anchored Hearing Aid: A Comparison of Surgical TechniquesDocument7 paginiBone-Anchored Hearing Aid: A Comparison of Surgical TechniquesShanaz KanandaÎncă nu există evaluări
- Endonasal Dacryocystorhinostomy, About 52 CasesDocument5 paginiEndonasal Dacryocystorhinostomy, About 52 CasesInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Novel TechniqueDocument6 paginiNovel Techniquekapilmalik2007Încă nu există evaluări
- Standardized Sternal Coverage Bota Et AlDocument7 paginiStandardized Sternal Coverage Bota Et AlOli BotaÎncă nu există evaluări
- Management of Trismus by Masseter Myotomy: January 2014Document4 paginiManagement of Trismus by Masseter Myotomy: January 2014Afifah Ratih RosavinaÎncă nu există evaluări
- Ijomi 15 415Document4 paginiIjomi 15 415Bagis Emre GulÎncă nu există evaluări
- Hernia UmmaDocument9 paginiHernia UmmaHeny KambuÎncă nu există evaluări
- From The Experience of Surgical Treatment of Patients With Scar Deformities of The Lower LimbsDocument5 paginiFrom The Experience of Surgical Treatment of Patients With Scar Deformities of The Lower LimbsCentral Asian StudiesÎncă nu există evaluări
- Fixation of Split Skin Graft Using Cyanoacrylate Tissue Adhesive Versus Skin Stapling: A Comparative StudyDocument4 paginiFixation of Split Skin Graft Using Cyanoacrylate Tissue Adhesive Versus Skin Stapling: A Comparative StudysindujasaravananÎncă nu există evaluări
- Cogajo Nasoseptal PediculadoDocument7 paginiCogajo Nasoseptal PediculadoRafa LopezÎncă nu există evaluări
- JCM 11 03305Document8 paginiJCM 11 03305Vainatheya AnanthÎncă nu există evaluări
- Minimal Incision in Parotidectomy: Reconstructive SurgeryDocument5 paginiMinimal Incision in Parotidectomy: Reconstructive SurgeryUriel Tre CaÎncă nu există evaluări
- Jurnal TelingaDocument9 paginiJurnal TelingaHasan HusienÎncă nu există evaluări
- 3) Singh2017Document5 pagini3) Singh2017joteja8497Încă nu există evaluări
- Management of Odontogenic Tumors / Orthodontic Courses by Indian Dental AcademyDocument82 paginiManagement of Odontogenic Tumors / Orthodontic Courses by Indian Dental Academyindian dental academyÎncă nu există evaluări
- JClinOphthalmolRes43143-3289519 090815Document6 paginiJClinOphthalmolRes43143-3289519 090815Wielda MutafadhilahÎncă nu există evaluări
- 137394-Article Text-367387-1-10-20160609Document2 pagini137394-Article Text-367387-1-10-20160609Luis GarciaÎncă nu există evaluări
- CLAVUS - An Overview and Case StudyDocument3 paginiCLAVUS - An Overview and Case StudyInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Cierre de Piel de Herida de Estoma Con Tecnica Purse-StringDocument7 paginiCierre de Piel de Herida de Estoma Con Tecnica Purse-Stringjesus aguirreÎncă nu există evaluări
- Short Term Outcomes of Stapled Hemorrhoidectomy Our Experience at GMC SrinagarDocument4 paginiShort Term Outcomes of Stapled Hemorrhoidectomy Our Experience at GMC SrinagarInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Alogénico Vs AutoóogoDocument4 paginiAlogénico Vs AutoóogoMaximiliano Jara ContrerasÎncă nu există evaluări
- VYplastyDocument6 paginiVYplastyVineet ArunÎncă nu există evaluări
- Sasjs 62 56-59Document4 paginiSasjs 62 56-59Marco Antonio MiraveteÎncă nu există evaluări
- Hard Palate Dermis Fat Composite Graft For Reconstruction of Contracted Anophthalmic SocketDocument7 paginiHard Palate Dermis Fat Composite Graft For Reconstruction of Contracted Anophthalmic SocketSaraelsy MonterrosoÎncă nu există evaluări
- Endoscopically Access YANG - TMJ ProsthesisDocument6 paginiEndoscopically Access YANG - TMJ ProsthesisClínica BMFÎncă nu există evaluări
- Ravikiran Naalla, 2020Document7 paginiRavikiran Naalla, 2020Ahmed SalahÎncă nu există evaluări
- Yu 그리고 Qiu - 2018 - Efficacy of the split-thickness labial flap methodDocument6 paginiYu 그리고 Qiu - 2018 - Efficacy of the split-thickness labial flap methodsupercool0120Încă nu există evaluări
- Soleus Muscle Flap For The Coverage of Pre-Tibial Defect of Middle Third of LegDocument6 paginiSoleus Muscle Flap For The Coverage of Pre-Tibial Defect of Middle Third of LegHassan KhanÎncă nu există evaluări
- Delta Wiring Technique To Treat Bony Mallet Fracture Technique Description and Case SeriesDocument4 paginiDelta Wiring Technique To Treat Bony Mallet Fracture Technique Description and Case SeriesInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Piezosurgery Versus Rotatory Osteotomy in Mandibular Impacted Third Molar ExtractionDocument17 paginiPiezosurgery Versus Rotatory Osteotomy in Mandibular Impacted Third Molar ExtractionHUYNH TRINHÎncă nu există evaluări
- 9685 40464 1 PBDocument3 pagini9685 40464 1 PBTri Sakti Sunda RomdhoniÎncă nu există evaluări
- Reupload Skin Graft ManagementDocument20 paginiReupload Skin Graft Managementhawaalia534100% (1)
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentDe la EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentÎncă nu există evaluări
- Graftless Solutions for the Edentulous PatientDe la EverandGraftless Solutions for the Edentulous PatientSaj JivrajÎncă nu există evaluări
- Interventional Treatment of Wounds: A Modern Approach for Better OutcomesDe la EverandInterventional Treatment of Wounds: A Modern Approach for Better OutcomesDennis P. OrgillÎncă nu există evaluări
- Contributo - 2017 - Blumgart S Surgery of The Liver Biliary Tract and PancreasDocument17 paginiContributo - 2017 - Blumgart S Surgery of The Liver Biliary Tract and PancreasJoe JoeÎncă nu există evaluări
- Video Conten - 2017 - Blumgart S Surgery of The Liver Biliary Tract and PancreaDocument1 paginăVideo Conten - 2017 - Blumgart S Surgery of The Liver Biliary Tract and PancreaJoe JoeÎncă nu există evaluări
- Varicocele C To MyDocument1 paginăVaricocele C To MyJoe JoeÎncă nu există evaluări
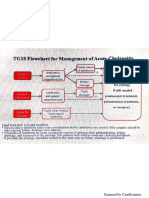
- Tokyo GuidelineDocument7 paginiTokyo GuidelineJoe JoeÎncă nu există evaluări
- Risk Management Reports SummaryDocument440 paginiRisk Management Reports Summarybenjamin GalarzaÎncă nu există evaluări
- Opportunistic Parasitic InfectionsDocument57 paginiOpportunistic Parasitic Infectionstummalapalli venkateswara raoÎncă nu există evaluări
- Health7 Q3 Module7Document18 paginiHealth7 Q3 Module7Joams artsÎncă nu există evaluări
- Achilles TendonDocument2 paginiAchilles TendonojuditaÎncă nu există evaluări
- ORAL SPRAY Range - Biovencer HealthcareDocument12 paginiORAL SPRAY Range - Biovencer Healthcaredr NayanBharadwajÎncă nu există evaluări
- Trauma-Burn Job Aid - FINALDocument2 paginiTrauma-Burn Job Aid - FINALJuan Antonio GarcíaÎncă nu există evaluări
- Airawat Group Presentation-Education & Road Safety For CorporatesDocument28 paginiAirawat Group Presentation-Education & Road Safety For CorporatessvnehalÎncă nu există evaluări
- Lesson 1 HandwashingDocument16 paginiLesson 1 HandwashingNene AgnasÎncă nu există evaluări
- Disaster Management Continuum Pre-DisasterDocument2 paginiDisaster Management Continuum Pre-DisasterPearl JuntillaÎncă nu există evaluări
- Children's Rights and Responsibilities 2020 - PROCAREDocument6 paginiChildren's Rights and Responsibilities 2020 - PROCAREstanely ndlovu0% (1)
- 7 Adverse Reactions To TransfusionDocument7 pagini7 Adverse Reactions To TransfusionPutriÎncă nu există evaluări
- Solar Annual Report 2010-11Document106 paginiSolar Annual Report 2010-11equityanalystinvestorÎncă nu există evaluări
- 2016 ACPL Expanded Content OutlineDocument9 pagini2016 ACPL Expanded Content OutlineiisforintheskyÎncă nu există evaluări
- Nutrition and MicrobiologyDocument6 paginiNutrition and MicrobiologyJean Paul IzeÎncă nu există evaluări
- MCQ of NeurologyDocument45 paginiMCQ of Neurologyeffe26100% (7)
- Argument Essay Sarah SimonizDocument4 paginiArgument Essay Sarah Simonizapi-270884210Încă nu există evaluări
- Tgas Bahasa InggrisDocument2 paginiTgas Bahasa Inggrisbilly jordiÎncă nu există evaluări
- Focusing On Children Mental HealthDocument2 paginiFocusing On Children Mental HealthDzatil HusniÎncă nu există evaluări
- Perceptual and Memory Biases For Health PDFDocument12 paginiPerceptual and Memory Biases For Health PDFRoxana MălinÎncă nu există evaluări
- BioginkgoDocument8 paginiBioginkgoCherry San DiegoÎncă nu există evaluări
- Krishna ThulasiDocument7 paginiKrishna ThulasisreyakÎncă nu există evaluări
- Bi Support Groups1Document6 paginiBi Support Groups1api-301357752Încă nu există evaluări
- Project Proposal Template PTADocument3 paginiProject Proposal Template PTAP Olarte ESÎncă nu există evaluări
- Final PNIDocument43 paginiFinal PNIWhisperer Bowen50% (2)
- Libs 2804 Assignment 1 Fall 2021Document2 paginiLibs 2804 Assignment 1 Fall 2021api-537166164Încă nu există evaluări
- Stages. 1.filipino Food Pyramid Guide: 1.a.pregnancyDocument11 paginiStages. 1.filipino Food Pyramid Guide: 1.a.pregnancyChristine Joy MolinaÎncă nu există evaluări
- Nwnewgradprogramcl KbasakosDocument1 paginăNwnewgradprogramcl Kbasakosapi-457168955Încă nu există evaluări
- Philosophy: I.Meaning of PhilosophyDocument12 paginiPhilosophy: I.Meaning of Philosophysivagiri.pÎncă nu există evaluări
- Dental Negligence in Clinical PracticeDocument18 paginiDental Negligence in Clinical PracticeLutfun NessaÎncă nu există evaluări
- Imhotep Journal May 2010 Vol 7 - Afrikan Conceptualizations of Wellness & IllnessDocument64 paginiImhotep Journal May 2010 Vol 7 - Afrikan Conceptualizations of Wellness & Illnessbestmatrix1Încă nu există evaluări