S-ar putea să vă placă și
- Mary - Binet Kamat ITDocument5 paginiMary - Binet Kamat ITEva97doe100% (1)
- NIMHANS Psychological ReportDocument3 paginiNIMHANS Psychological ReportSuzanna100% (6)
- Sample MISIC ReportDocument2 paginiSample MISIC ReportHarsh Mehta100% (2)
- Developmental Psychopathology ChecklistDocument5 paginiDevelopmental Psychopathology ChecklistHimani100% (1)
- Norms MisicDocument4 paginiNorms Misicvk100% (3)
- Binet Kamat TestDocument2 paginiBinet Kamat Testpooja0% (1)
- WAPISDocument13 paginiWAPISLakshmi Saranya57% (7)
- TAT Uma Chaudhary - ClassDocument3 paginiTAT Uma Chaudhary - Classishita aggarwal100% (4)
- Vineland Social Maturity Scale: Indian AdaptationDocument2 paginiVineland Social Maturity Scale: Indian AdaptationKinjal A100% (2)
- DST Report FormatDocument3 paginiDST Report FormatNasir100% (2)
- BKTDocument14 paginiBKTVarun Viswanathan100% (1)
- Binet Kamat Test For General Mental AbilitiesDocument54 paginiBinet Kamat Test For General Mental AbilitiesSana Siddiq100% (14)
- Seguin Form BoardDocument5 paginiSeguin Form Boardashvin91% (11)
- MISIC - Manual EdtDocument20 paginiMISIC - Manual Edtnesuma88% (32)
- Nimhans Performa: Compalints and Their DurationDocument3 paginiNimhans Performa: Compalints and Their Durationsyamfox150845% (11)
- Vineland Social Maturity ScaleDocument7 paginiVineland Social Maturity ScaleMiti59% (17)
- VSMS ManualDocument17 paginiVSMS ManualSubhasri Viswanathan100% (1)
- Bhatia Battery TestDocument5 paginiBhatia Battery TestAkshita SinghÎncă nu există evaluări
- Percentile Range Level of MemoryDocument3 paginiPercentile Range Level of MemoryAleena Thakurta67% (3)
- Seguin Form Board TestDocument3 paginiSeguin Form Board TestKamini Shankar81% (16)
- Pgi Memory Scale PDF FreeDocument7 paginiPgi Memory Scale PDF FreehdynfdhjgdddfhhÎncă nu există evaluări
- Developmental Screening TestDocument21 paginiDevelopmental Screening TestNasir89% (27)
- Psychological Test Price List 2009Document54 paginiPsychological Test Price List 2009Meenu Minu67% (9)
- BKTDocument36 paginiBKTPriya PuriÎncă nu există evaluări
- Nimhans Case Proforma NewDocument15 paginiNimhans Case Proforma Newi love garfield100% (4)
- Indian Adaptation of The Thematic Appreciation TestDocument1 paginăIndian Adaptation of The Thematic Appreciation TestAiswarya Venkataramanan100% (1)
- Issues Related To Training Professional TherapistsDocument11 paginiIssues Related To Training Professional TherapistsSaroja Roy100% (1)
- Span of AttentionDocument4 paginiSpan of AttentionDeepak Saini100% (1)
- PGIBBD Interpretation - ManualDocument6 paginiPGIBBD Interpretation - Manualishita aggarwal100% (3)
- Binet KamatDocument6 paginiBinet Kamatsnehaoct67% (15)
- Multiphasic Questionnaire (MPQ) : SRM Medical College Hospital & Research CentreDocument10 paginiMultiphasic Questionnaire (MPQ) : SRM Medical College Hospital & Research CentreRakesh Babu100% (1)
- Vineland Social Maturity Scale PDFDocument7 paginiVineland Social Maturity Scale PDFlakshmi shankarÎncă nu există evaluări
- Vineland Social Maturity Scale PDFDocument10 paginiVineland Social Maturity Scale PDFAmeera Chauhan100% (4)
- Barkha Binet 2Document2 paginiBarkha Binet 2api-228136529Încă nu există evaluări
- WAPISDocument6 paginiWAPISabdu rauf100% (8)
- Human Figure Drawing (HFD) By: Koppitz: Dr. Tahira Yousaf Senior Assistant ProfessorDocument23 paginiHuman Figure Drawing (HFD) By: Koppitz: Dr. Tahira Yousaf Senior Assistant ProfessorEman SiddiqiÎncă nu există evaluări
- Vineland Social Maturity TestDocument7 paginiVineland Social Maturity Testrafiqa40% (5)
- Vsms PracDocument8 paginiVsms Pracaditi singh50% (2)
- Sidhant IQ+SLDDocument3 paginiSidhant IQ+SLDNik DÎncă nu există evaluări
- VSMS Procedure For PracticalDocument7 paginiVSMS Procedure For PracticalPankaj Kumar100% (6)
- Problem Behaviour ChecklistDocument4 paginiProblem Behaviour ChecklistAsma Lakdawala83% (6)
- Bhatia Sample ReportDocument1 paginăBhatia Sample ReportNazema_Sagi100% (2)
- Asssessment of Intelligence of Children Using Malin'S Intelligence Scale For Indian ChildrenDocument12 paginiAsssessment of Intelligence of Children Using Malin'S Intelligence Scale For Indian Childrenpriyanshi khandelwal100% (1)
- Vineland Social Maturity ScaleDocument18 paginiVineland Social Maturity ScalePalak Gupta100% (3)
- Seguin Form Board (S.F.B) TestDocument1 paginăSeguin Form Board (S.F.B) TestfalguniÎncă nu există evaluări
- Binet Kamat Test Data SheetDocument3 paginiBinet Kamat Test Data Sheetspurthi_16100% (1)
- Vineland Social Maturity Scale (VSMS)Document18 paginiVineland Social Maturity Scale (VSMS)Aiswarya Venkataramanan83% (6)
- ISAA ToolDocument21 paginiISAA Toolkrishnaveni arulkumarÎncă nu există evaluări
- Psychological Assessment Report: 1) NIMHANS Neuropsychological BatteryDocument3 paginiPsychological Assessment Report: 1) NIMHANS Neuropsychological BatteryKavitha MA100% (1)
- Arun Misic NotesDocument4 paginiArun Misic Notesapi-228136529Încă nu există evaluări
- Pgi Memory ScaleDocument7 paginiPgi Memory Scaleabdu rauf93% (29)
- CIS PracticalDocument10 paginiCIS Practicalaysha fariha100% (1)
- Vineland Social Maturity ScaleDocument17 paginiVineland Social Maturity ScalePRITI PUNWANI 2022433786% (14)
- Practical No. 04 Sentence Completion Test AIM/OBJECTIVES: The Objectives of This Test Is To Measure Certain Personality Traits. AnDocument4 paginiPractical No. 04 Sentence Completion Test AIM/OBJECTIVES: The Objectives of This Test Is To Measure Certain Personality Traits. AnChetana D100% (3)
- VSMSDocument9 paginiVSMSAiswarya Venkataramanan60% (5)
- Psych OutlineDocument4 paginiPsych OutlineSam Raven AndresÎncă nu există evaluări
- Clinical Evaluation of The Psychiatric PatientDocument4 paginiClinical Evaluation of The Psychiatric Patienthannjazz100% (1)
- Psychiatric Assessment and Evaluation: History TakingDocument9 paginiPsychiatric Assessment and Evaluation: History TakingWaheedullah AhmadiÎncă nu există evaluări
- Thirteen Areas of AssessmentDocument3 paginiThirteen Areas of AssessmentkcÎncă nu există evaluări
- Family Case Analysis Format I.: College of NursingDocument4 paginiFamily Case Analysis Format I.: College of NursingclarÎncă nu există evaluări
- Tele Medicine Practice Guidelines, MOHFW, Govt of IndiaDocument48 paginiTele Medicine Practice Guidelines, MOHFW, Govt of IndiaManish SharmaÎncă nu există evaluări
- PDFDocument19 paginiPDFSarika VarshneyÎncă nu există evaluări
- Advion WDG Marketing Leaflet - English PDFDocument4 paginiAdvion WDG Marketing Leaflet - English PDFSarika VarshneyÎncă nu există evaluări
- Press Communique-English 4 Feb 2020 PDFDocument1 paginăPress Communique-English 4 Feb 2020 PDFSarika VarshneyÎncă nu există evaluări
- Isbn 978-1-29203-961-9Document7 paginiIsbn 978-1-29203-961-9BeenishÎncă nu există evaluări
- Worksheet Thought Distortion Response.04Document4 paginiWorksheet Thought Distortion Response.04Sarika VarshneyÎncă nu există evaluări
- Sarvabhashin En-Kn Script PDFDocument255 paginiSarvabhashin En-Kn Script PDFSarika VarshneyÎncă nu există evaluări
- DepressionDocument1 paginăDepressionSarika VarshneyÎncă nu există evaluări
- Isbn 978-1-29203-961-9Document7 paginiIsbn 978-1-29203-961-9BeenishÎncă nu există evaluări
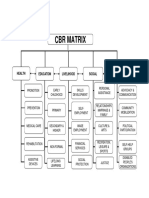
- CBR Matrix 11.10 PDFDocument1 paginăCBR Matrix 11.10 PDFSarika VarshneyÎncă nu există evaluări
- Statistics GuideDocument14 paginiStatistics GuideMarco Antonio CovieloÎncă nu există evaluări
- Draft NEP 2019 en RevisedDocument484 paginiDraft NEP 2019 en RevisedArjun PrabhakaranÎncă nu există evaluări
- MlcuDocument3 paginiMlcuSarika VarshneyÎncă nu există evaluări
- RCI Clarification LetterDocument1 paginăRCI Clarification LetterSarika VarshneyÎncă nu există evaluări
- Newsletter RtdcsstyDocument5 paginiNewsletter RtdcsstySarika VarshneyÎncă nu există evaluări
- A Pa Format Example 2Document3 paginiA Pa Format Example 2deadpool_merc2000Încă nu există evaluări
- Python For DADocument47 paginiPython For DAAnand Ranjan100% (2)
- Sports Psychology PDFDocument6 paginiSports Psychology PDFSarika VarshneyÎncă nu există evaluări
- The "Index Technique" in Worn Dentition: A New and Conservative ApproachDocument32 paginiThe "Index Technique" in Worn Dentition: A New and Conservative ApproachHektor Hak100% (1)
- Cannabis Sativa Aka MarijuanaDocument22 paginiCannabis Sativa Aka MarijuanaFuckÎncă nu există evaluări
- Final-Minutes of 9th Meeting of EEC PDFDocument14 paginiFinal-Minutes of 9th Meeting of EEC PDFShakil KhanÎncă nu există evaluări
- Drug-Induced Nephrotoxicity: Cynthia A. Naughton, Pharmd, BCPS, North Dakota State University College of PharmacyDocument8 paginiDrug-Induced Nephrotoxicity: Cynthia A. Naughton, Pharmd, BCPS, North Dakota State University College of PharmacyAbdur Rachman Ba'abdullahÎncă nu există evaluări
- Adrenergic DrugsDocument2 paginiAdrenergic DrugsSunshine_Bacla_4275Încă nu există evaluări
- Use of Essential Oils Following Traumatic Burn Injury A Case StudyDocument12 paginiUse of Essential Oils Following Traumatic Burn Injury A Case StudyShandaPrimaDewiÎncă nu există evaluări
- Behavioral Psychology EssayDocument5 paginiBehavioral Psychology Essayapi-432362448100% (1)
- Conversational HypnosisDocument1 paginăConversational HypnosisNunky HendrawanÎncă nu există evaluări
- Body Image and Shame - No Body Is PerfectDocument4 paginiBody Image and Shame - No Body Is PerfectVanessa Million100% (2)
- Manav Rachna Sports Science BrochureDocument23 paginiManav Rachna Sports Science Brochurealbha oberoiÎncă nu există evaluări
- Caring For The Heart Failure Patient: Contemporary Nursing InterventionsDocument8 paginiCaring For The Heart Failure Patient: Contemporary Nursing Interventionsnurulanisa0703Încă nu există evaluări
- Lupus Power Point Fact SheetDocument21 paginiLupus Power Point Fact Sheetacmarcus89Încă nu există evaluări
- Professional Nursing OrganizationDocument4 paginiProfessional Nursing OrganizationCid Benedict PabalanÎncă nu există evaluări
- DKS CatalogueDocument17 paginiDKS CatalogueHorea Mihai OargaÎncă nu există evaluări
- Creating A Productive Learning EnvironmentDocument43 paginiCreating A Productive Learning EnvironmentDeSpirit Neverdies100% (1)
- Eric Berg CVDocument6 paginiEric Berg CVHaralambicÎncă nu există evaluări
- Midazolam Injection: New Zealand Data SheetDocument14 paginiMidazolam Injection: New Zealand Data SheetAlin AdelineÎncă nu există evaluări
- Adverse Reaction Blood BankDocument10 paginiAdverse Reaction Blood BankyourfamilydoctorÎncă nu există evaluări
- ParacetamolDocument24 paginiParacetamolFriné MirandaÎncă nu există evaluări
- MT Traditional and Alert Hypnosis For Education A Literature ReviewDocument12 paginiMT Traditional and Alert Hypnosis For Education A Literature ReviewFrancisca GonçalvesÎncă nu există evaluări
- SCLC A Cancer PowerpointDocument7 paginiSCLC A Cancer Powerpointapi-353368377Încă nu există evaluări
- Wound DebridementDocument21 paginiWound DebridementKrisna MuhammadÎncă nu există evaluări
- Prehospital Antibiotic Prophylaxis For Open Fractures: Practicality and SafetyDocument11 paginiPrehospital Antibiotic Prophylaxis For Open Fractures: Practicality and SafetyMarco Culqui SánchezÎncă nu există evaluări
- Phase III Clinical Trials - 2014-15Document23 paginiPhase III Clinical Trials - 2014-15Ali TasleemÎncă nu există evaluări
- Comprehensive Cognitive-Behavior TherapyDocument106 paginiComprehensive Cognitive-Behavior Therapypsihologice100% (4)
- SulfonamidesDocument22 paginiSulfonamidesFaizan Tariq100% (1)
- Psych Midterm ExamDocument6 paginiPsych Midterm Examteabagman100% (3)
- Diabetic Foot ImfectionsDocument26 paginiDiabetic Foot ImfectionsYoga Pribadi UtomoÎncă nu există evaluări
- TriageDocument14 paginiTriageNiko AndreanÎncă nu există evaluări
- COPD LeafletDocument2 paginiCOPD LeafletAN KnEeÎncă nu există evaluări
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (24)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (80)
- Summary of The 48 Laws of Power: by Robert GreeneDe la EverandSummary of The 48 Laws of Power: by Robert GreeneEvaluare: 4.5 din 5 stele4.5/5 (233)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisDe la EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (9)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4 din 5 stele4/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (169)
- Codependent No More: How to Stop Controlling Others and Start Caring for YourselfDe la EverandCodependent No More: How to Stop Controlling Others and Start Caring for YourselfEvaluare: 5 din 5 stele5/5 (88)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (1)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDe la EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningEvaluare: 4 din 5 stele4/5 (3)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDe la EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeEvaluare: 4.5 din 5 stele4.5/5 (253)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDe la EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryEvaluare: 4 din 5 stele4/5 (44)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- Troubled: A Memoir of Foster Care, Family, and Social ClassDe la EverandTroubled: A Memoir of Foster Care, Family, and Social ClassEvaluare: 4.5 din 5 stele4.5/5 (26)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosDe la Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosEvaluare: 4.5 din 5 stele4.5/5 (207)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryDe la EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryEvaluare: 4.5 din 5 stele4.5/5 (157)