S-ar putea să vă placă și
- ITF033 eSRSEmployerEnrollmentForm V04 PDFDocument1 paginăITF033 eSRSEmployerEnrollmentForm V04 PDFDarlyn EtangÎncă nu există evaluări
- Esrs Employer Enrollment Form: Employer ID Number Employer/Business Name Pag-IBIG Servicing Branch Employer TypeDocument1 paginăEsrs Employer Enrollment Form: Employer ID Number Employer/Business Name Pag-IBIG Servicing Branch Employer TypeGina Garcia100% (1)
- TMF190 eSRSEmployerEnrollmentForm V04 PDFDocument1 paginăTMF190 eSRSEmployerEnrollmentForm V04 PDFLSM MILCÎncă nu există evaluări
- eSRS Reg Form 2 PDFDocument1 paginăeSRS Reg Form 2 PDFDarlyn EtangÎncă nu există evaluări
- TMF190 eSRSEmployerEnrollmentForm V04 PDFDocument1 paginăTMF190 eSRSEmployerEnrollmentForm V04 PDFKim Espart CastilloÎncă nu există evaluări
- TMF190 eSRSEmployerEnrollmentForm V04 PDFDocument1 paginăTMF190 eSRSEmployerEnrollmentForm V04 PDFKim Espart CastilloÎncă nu există evaluări
- Esrs Employer Enrollment Form: Employer ID Number Employer Name Pag-IBIG Servicing Branch Employer TypeDocument1 paginăEsrs Employer Enrollment Form: Employer ID Number Employer Name Pag-IBIG Servicing Branch Employer TypeJo LouiseÎncă nu există evaluări
- E SRSDocument1 paginăE SRSLaurence RabuyaÎncă nu există evaluări
- TMF190 ESRSEmployerEnrollmentForm V05Document1 paginăTMF190 ESRSEmployerEnrollmentForm V05dylanÎncă nu există evaluări
- Pagibig E-RegDocument1 paginăPagibig E-RegMaricor TambalÎncă nu există evaluări
- Pag-IBIG Employer Enrollment FormDocument2 paginiPag-IBIG Employer Enrollment FormJhonna Magtoto100% (2)
- PFF002 - Employer's Data Form - V04 - PDF PDFDocument2 paginiPFF002 - Employer's Data Form - V04 - PDF PDFarlyn100% (1)
- eSRS Reg Form PDFDocument1 paginăeSRS Reg Form PDFDarlyn Etang100% (1)
- Pag-IBIG Employer Enrollment FormDocument1 paginăPag-IBIG Employer Enrollment FormDarlyn Etang100% (1)
- TMF 2020Document1 paginăTMF 2020Brianna Mendez100% (1)
- PFF002 EmployersDataForm V06Document2 paginiPFF002 EmployersDataForm V06hitme bensiÎncă nu există evaluări
- Employer's Data Form (EDF, HQP-PFF-002, V03.2) PDFDocument2 paginiEmployer's Data Form (EDF, HQP-PFF-002, V03.2) PDFPamela Angelica Obaniana FisicoÎncă nu există evaluări
- Pag-IBIG Fund Employer Registration Form GuideDocument2 paginiPag-IBIG Fund Employer Registration Form GuideRoniel Cedeño100% (5)
- Employers Data Form 2019Document2 paginiEmployers Data Form 2019Michelle Hernandez50% (2)
- TMF190 eSRSEmployerEnrollmentForm V05Document1 paginăTMF190 eSRSEmployerEnrollmentForm V05Selwyn John G. GuiruelaÎncă nu există evaluări
- BCIF Version 7Document1 paginăBCIF Version 7Denise RadomesÎncă nu există evaluări
- Pag-IBIG Employer Registration Form GuideDocument2 paginiPag-IBIG Employer Registration Form GuideHRD-EFI PampangaÎncă nu există evaluări
- Pag-IBIG Employer Registration FormsDocument3 paginiPag-IBIG Employer Registration FormsJhen S. Domingo100% (1)
- (For IISP Branch Only) : Application AgreementDocument2 pagini(For IISP Branch Only) : Application AgreementRachel CabanlitÎncă nu există evaluări
- Pag-Ibig Loyalty Card Plus Account Holder'S Contact Details Change Request FormDocument1 paginăPag-Ibig Loyalty Card Plus Account Holder'S Contact Details Change Request FormBreahziel ParillaÎncă nu există evaluări
- Employer'S Virtual Pag-Ibig Enrollment FormDocument2 paginiEmployer'S Virtual Pag-Ibig Enrollment FormRobert Paul A Moreno0% (2)
- BCIF - Ver9 With DPA and Bill Delivery Agreement - 02022022Document1 paginăBCIF - Ver9 With DPA and Bill Delivery Agreement - 02022022Tegnap NehjÎncă nu există evaluări
- Lgu Bcif SampleDocument1 paginăLgu Bcif SampleRodelLaborÎncă nu există evaluări
- PHOTO BUYER INFORMATIONDocument2 paginiPHOTO BUYER INFORMATIONiyaÎncă nu există evaluări
- Apply for Moratorium on Pag-IBIG STL PaymentsDocument2 paginiApply for Moratorium on Pag-IBIG STL PaymentsJhonson MedranoÎncă nu există evaluări
- HLF576 ApplicationMoratoriumHLAmortizationPayments V01Document2 paginiHLF576 ApplicationMoratoriumHLAmortizationPayments V01ivyÎncă nu există evaluări
- AAF238 OTBPublicAuctionJuridical V02Document2 paginiAAF238 OTBPublicAuctionJuridical V02JC JoseÎncă nu există evaluări
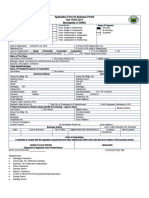
- Application Form For Business Permit Tax Year 2017 Municipality of GAMUDocument1 paginăApplication Form For Business Permit Tax Year 2017 Municipality of GAMUGamu DILGÎncă nu există evaluări
- Bcif Front PartnershipDocument1 paginăBcif Front PartnershipASDFÎncă nu există evaluări
- BCIF - Ver7 With DPA - 02052018 PDFDocument1 paginăBCIF - Ver7 With DPA - 02052018 PDFJon Colinares50% (2)
- Bplo Unified Form PDFDocument2 paginiBplo Unified Form PDFTristan Lindsey Kaamiño AresÎncă nu există evaluări
- Philippines Business Permit ApplicationDocument3 paginiPhilippines Business Permit ApplicationMr. Kitty CatÎncă nu există evaluări
- Applicationform New Grey ScaleDocument2 paginiApplicationform New Grey ScaleStanley ValencianaÎncă nu există evaluări
- Business Customer Information FormDocument2 paginiBusiness Customer Information FormWalter O BrianÎncă nu există evaluări
- Customer Information Form PDFDocument1 paginăCustomer Information Form PDFNasseb Jaan AliÎncă nu există evaluări
- Employer'S Data Form (Edf) : InstructionsDocument2 paginiEmployer'S Data Form (Edf) : InstructionsVictor CaubeÎncă nu există evaluări
- HLF201 LetterOfIntent (NPARP) V01Document2 paginiHLF201 LetterOfIntent (NPARP) V01Emil PerveraÎncă nu există evaluări
- Philippine Business Permit Application FormDocument1 paginăPhilippine Business Permit Application FormJESSA VILLEGAS TALINGTINGÎncă nu există evaluări
- Calamity Loan Application SummaryDocument2 paginiCalamity Loan Application SummaryReddy RentarÎncă nu există evaluări
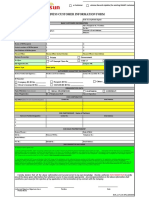
- Business Customer Information Form: Registered Business Name: Store/Shop/Outlet Name/Trade NameDocument2 paginiBusiness Customer Information Form: Registered Business Name: Store/Shop/Outlet Name/Trade Namelhuk banaag100% (2)
- HB City - Business-License-ApplicationDocument2 paginiHB City - Business-License-ApplicationPatrick SullivanÎncă nu există evaluări
- Cis FormDocument1 paginăCis Formzyd82pmg54Încă nu există evaluări
- Pag-IBIG MPL Loan ApplicationDocument2 paginiPag-IBIG MPL Loan ApplicationBecca BelenÎncă nu există evaluări
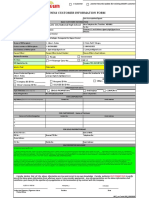
- Business Customer Information Form: Registered Business Name: Store/Shop/Outlet Name/Trade NameDocument3 paginiBusiness Customer Information Form: Registered Business Name: Store/Shop/Outlet Name/Trade NameRodelLaborÎncă nu există evaluări
- Https2Fwww Pagibigfund Gov Ph2Fdocument2Fpdf2Fdlforms2Fprovidentrelated2FDocument4 paginiHttps2Fwww Pagibigfund Gov Ph2Fdocument2Fpdf2Fdlforms2Fprovidentrelated2FKingÎncă nu există evaluări
- HLF047 ApplicationMoratoriumHLAmortizationPayments V03Document1 paginăHLF047 ApplicationMoratoriumHLAmortizationPayments V03JamesÎncă nu există evaluări
- MCRF Pagibig FormDocument3 paginiMCRF Pagibig FormFrench Kamile PagcuÎncă nu există evaluări
- Employer'S Change of Information Form (Ecif) : InstructionsDocument2 paginiEmployer'S Change of Information Form (Ecif) : InstructionsGarcia Supermart, Inc.Încă nu există evaluări
- Address Contact Details Change Form PDFDocument2 paginiAddress Contact Details Change Form PDFtarun_akkuÎncă nu există evaluări
- New Customer Records UpdateDocument3 paginiNew Customer Records Updatepretty mangayÎncă nu există evaluări
- Business Customer Information Form: Registered Business Name: MANG JUAN'S RESTO Store/Shop/Outlet Name/Trade NameDocument1 paginăBusiness Customer Information Form: Registered Business Name: MANG JUAN'S RESTO Store/Shop/Outlet Name/Trade NameRivera OwenÎncă nu există evaluări
- SLF065 MultiPurposeLoanApplicationForm V03Document2 paginiSLF065 MultiPurposeLoanApplicationForm V03Belle Adante100% (1)
- Evaluation of Some Virtual Phone Numbers ServicesDe la EverandEvaluation of Some Virtual Phone Numbers ServicesÎncă nu există evaluări
- Goods and Services Tax (GST) Filing Made Easy: Free Software Literacy SeriesDe la EverandGoods and Services Tax (GST) Filing Made Easy: Free Software Literacy SeriesÎncă nu există evaluări
- How To Structure Your Business For Success: Everything You Need To Know To Get Started Building Business CreditDe la EverandHow To Structure Your Business For Success: Everything You Need To Know To Get Started Building Business CreditÎncă nu există evaluări
- Finals Emptech ReviewerDocument3 paginiFinals Emptech ReviewerClaudine ConcepcionÎncă nu există evaluări
- Killer User Guide 4.0Document15 paginiKiller User Guide 4.0hlkhnklht6s555Încă nu există evaluări
- Contact Center Services NC II AssessmentDocument6 paginiContact Center Services NC II AssessmentTrexie P. Peralta50% (2)
- July 2020 Coordinated Inauthentic Behavior ReportDocument32 paginiJuly 2020 Coordinated Inauthentic Behavior ReportJhon MarvinÎncă nu există evaluări
- EC Integration GuideDocument56 paginiEC Integration GuideMrPollitoÎncă nu există evaluări
- Amit Vadhadiya Saving Ac PDFDocument11 paginiAmit Vadhadiya Saving Ac PDFKotadiya ChiragÎncă nu există evaluări
- Blackhatprofools: Internet MarketingDocument7 paginiBlackhatprofools: Internet MarketingJeff OgunsholaÎncă nu există evaluări
- All CS MCQsDocument82 paginiAll CS MCQsShuseel Baral100% (2)
- Directing Your Own Porn Lenguage of LustDocument13 paginiDirecting Your Own Porn Lenguage of LustValpo Valparaiso100% (2)
- AdminGuideVSP57 Rev07August2013 MobilIronDocument834 paginiAdminGuideVSP57 Rev07August2013 MobilIronJMMÎncă nu există evaluări
- Irokas - Aida Sydney 2013Document17 paginiIrokas - Aida Sydney 2013snehaÎncă nu există evaluări
- Function Point AnalysisDocument111 paginiFunction Point AnalysisVTR Ravi Kumar100% (2)
- Computer History Timeline - Keren ElvirDocument11 paginiComputer History Timeline - Keren Elvirapi-294367390Încă nu există evaluări
- The InetAddress Class Has No Visible ConstructorsDocument18 paginiThe InetAddress Class Has No Visible ConstructorsAnkit Tiwari0% (1)
- E Novia Engineering CentralDocument364 paginiE Novia Engineering Centralnarred74100% (1)
- NMS Ibuilder Guide 8.0.2.5Document412 paginiNMS Ibuilder Guide 8.0.2.5crispix2000Încă nu există evaluări
- 2 MDB - Movies, TV and Celebrities - IMDbDocument4 pagini2 MDB - Movies, TV and Celebrities - IMDbBala MuruganÎncă nu există evaluări
- Study On How Dark Web Facilitate Cyber Security Experts To Improve Business SecuritDocument8 paginiStudy On How Dark Web Facilitate Cyber Security Experts To Improve Business SecuritIJRASETPublicationsÎncă nu există evaluări
- Ibeta Completes Spoofing and Liveness Testing ProjectDocument2 paginiIbeta Completes Spoofing and Liveness Testing ProjectPR.comÎncă nu există evaluări
- Situational Questions - InterviewDocument3 paginiSituational Questions - InterviewLadimer SabidaÎncă nu există evaluări
- CSE 338 Lab Manual 5Document7 paginiCSE 338 Lab Manual 5Russel PeterÎncă nu există evaluări
- Hydraulic Pumps and MotorsDocument1 paginăHydraulic Pumps and MotorsChumporn SaraphatmarkyingÎncă nu există evaluări
- Manual Adobe AnimateDocument482 paginiManual Adobe AnimateMaycol Vivanco Mayta100% (2)
- Cisco Pppoe Server Configuration Example: Sign UpDocument10 paginiCisco Pppoe Server Configuration Example: Sign UpAnonymous 2zqZO1rZÎncă nu există evaluări
- E Commerce 2019 Business Technology and Society 15th Edition Laudon Solutions ManualDocument18 paginiE Commerce 2019 Business Technology and Society 15th Edition Laudon Solutions Manualdillonbowmankwyreifmap100% (15)
- Peopletools Tables (Where The Metadata Is Stored) : Project Items List Via SQLDocument22 paginiPeopletools Tables (Where The Metadata Is Stored) : Project Items List Via SQLRajendra PilludaÎncă nu există evaluări
- Mrs. Abha SoniDocument15 paginiMrs. Abha SoniRainee KocharÎncă nu există evaluări
- Chapter 4 Enhanced Interior Gateway Protocol (EIGRP)Document53 paginiChapter 4 Enhanced Interior Gateway Protocol (EIGRP)Bi Jr.Încă nu există evaluări
- Online Math Teaching ReportDocument5 paginiOnline Math Teaching Reportjamil publicoÎncă nu există evaluări
- Tato Architects - ArchDailyDocument6 paginiTato Architects - ArchDailySerly Hutami PutriÎncă nu există evaluări