S-ar putea să vă placă și
- Soa T TannouryDocument3 paginiSoa T TannourySoumabho DasÎncă nu există evaluări
- EMG TestingDocument50 paginiEMG TestingSoumabho DasÎncă nu există evaluări
- 2001 Self-Assessment Examination For Residents (Sae-R) Multiple-Choice Questions Booklet Abridged VersionDocument23 pagini2001 Self-Assessment Examination For Residents (Sae-R) Multiple-Choice Questions Booklet Abridged VersionSoumabho DasÎncă nu există evaluări
- Abridged Version: 2002 Self-Assessment Examination For Residents (SAE-R) Answer Key and Commentary On Preferred ChoiceDocument13 paginiAbridged Version: 2002 Self-Assessment Examination For Residents (SAE-R) Answer Key and Commentary On Preferred ChoiceSoumabho DasÎncă nu există evaluări
- 2005 Self-Assessment Examination For Residents (Sae-R) : Abridged VersionDocument22 pagini2005 Self-Assessment Examination For Residents (Sae-R) : Abridged VersionSoumabho DasÎncă nu există evaluări
- Co A Volpe 12 16 21Document6 paginiCo A Volpe 12 16 21Soumabho DasÎncă nu există evaluări
- 2002SAEquestions PDFDocument28 pagini2002SAEquestions PDFSoumabho Das100% (1)
- 08SAER AbridgedDocument22 pagini08SAER AbridgedBabon BaboÎncă nu există evaluări
- Abridged Version: 2002 Self-Assessment Examination For Residents (SAE-R) Answer Key and Commentary On Preferred ChoiceDocument13 paginiAbridged Version: 2002 Self-Assessment Examination For Residents (SAE-R) Answer Key and Commentary On Preferred ChoiceSoumabho DasÎncă nu există evaluări
- 2001 Self-Assessment Examination For Residents (SAE-R) Multiple-Choice Questions Answer Key and Commentary On Preferred ChoiceDocument11 pagini2001 Self-Assessment Examination For Residents (SAE-R) Multiple-Choice Questions Answer Key and Commentary On Preferred ChoiceSoumabho DasÎncă nu există evaluări
- 2008 AnswersDocument16 pagini2008 AnswersSoumabho DasÎncă nu există evaluări
- 2004 SAEanswersDocument12 pagini2004 SAEanswersSoumabho DasÎncă nu există evaluări
- 2007 AnswersDocument13 pagini2007 AnswersSoumabho DasÎncă nu există evaluări
- 2002SAEquestions PDFDocument28 pagini2002SAEquestions PDFSoumabho Das100% (1)
- 8 - Ganglion Impar InjectionDocument1 pagină8 - Ganglion Impar InjectionSoumabho DasÎncă nu există evaluări
- 2005 Self-Assessment Examination For Residents (SAE-R) Multiple-Choice Questions Answer Key and Commentary On Preferred ChoiceDocument11 pagini2005 Self-Assessment Examination For Residents (SAE-R) Multiple-Choice Questions Answer Key and Commentary On Preferred ChoiceSoumabho DasÎncă nu există evaluări
- Capgras DelusionDocument1 paginăCapgras DelusionSoumabho DasÎncă nu există evaluări
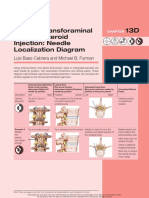
- Lumbar Transforaminal Epidural Steroid Injection: Needle Localization DiagramDocument2 paginiLumbar Transforaminal Epidural Steroid Injection: Needle Localization DiagramSoumabho DasÎncă nu există evaluări
- Best Practices For Intrathecal Baclofen Therapy - Screening TestDocument7 paginiBest Practices For Intrathecal Baclofen Therapy - Screening TestSoumabho DasÎncă nu există evaluări
- Dilution Reconstitution Injection GuideDocument2 paginiDilution Reconstitution Injection GuideSoumabho DasÎncă nu există evaluări
- 9 - Sacral Insufficiency Fracture Repair-SacroplastyDocument7 pagini9 - Sacral Insufficiency Fracture Repair-SacroplastySoumabho DasÎncă nu există evaluări
- 7C - Caudal Epidural Steroid Injection - Ultrasound GuidanceDocument5 pagini7C - Caudal Epidural Steroid Injection - Ultrasound GuidanceSoumabho DasÎncă nu există evaluări
- 9 - Sacral Insufficiency Fracture Repair-SacroplastyDocument7 pagini9 - Sacral Insufficiency Fracture Repair-SacroplastySoumabho DasÎncă nu există evaluări
- 2 - Needle TechniquesDocument8 pagini2 - Needle TechniquesSoumabho DasÎncă nu există evaluări
- Pump Off Authorization FormDocument1 paginăPump Off Authorization FormSoumabho DasÎncă nu există evaluări
- Intrathecal Baclofen PumpDocument19 paginiIntrathecal Baclofen PumpSoumabho DasÎncă nu există evaluări
- Best Practices For Intrathecal Baclofen Therapy - Dosing and Long-Term ManagementDocument9 paginiBest Practices For Intrathecal Baclofen Therapy - Dosing and Long-Term ManagementSoumabho DasÎncă nu există evaluări
- Best Practices For Intrathecal Baclofen Therapy - Patient SelectionDocument9 paginiBest Practices For Intrathecal Baclofen Therapy - Patient SelectionSoumabho DasÎncă nu există evaluări
- Atlas of Muscle Innervation Zones 2012 PDFDocument145 paginiAtlas of Muscle Innervation Zones 2012 PDFSoumabho DasÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- LF1325LC 装机准备要求 LF1325LC installation requirementsDocument12 paginiLF1325LC 装机准备要求 LF1325LC installation requirementsEliasDraÎncă nu există evaluări
- Civil EngineeringDocument13 paginiCivil EngineeringMahmoud OuryemchiÎncă nu există evaluări
- The Learner The Learner : 1 QuarterDocument4 paginiThe Learner The Learner : 1 QuarterRode Jane SumambanÎncă nu există evaluări
- Uas Semt Genap Fix BING XIDocument12 paginiUas Semt Genap Fix BING XISaepulloh KurniaÎncă nu există evaluări
- Dr. Shekhar Challa Joins Bioscience Americas Board of AdvisorsDocument2 paginiDr. Shekhar Challa Joins Bioscience Americas Board of AdvisorsPR.comÎncă nu există evaluări
- The Power of Partnership: Underground Room & Pillar Lateral Development and DownholesDocument4 paginiThe Power of Partnership: Underground Room & Pillar Lateral Development and DownholesjoxegutierrezgÎncă nu există evaluări
- Transition FX3U - C To iQ-F Series HandbookDocument58 paginiTransition FX3U - C To iQ-F Series HandbookKelly Leandro MazieroÎncă nu există evaluări
- Design of Marina Structures and FacilitiesDocument23 paginiDesign of Marina Structures and FacilitiesAhmed Balah0% (1)
- Material Safety Data Sheet Glyphosate 5.4Document5 paginiMaterial Safety Data Sheet Glyphosate 5.4Ahfi Rizqi FajrinÎncă nu există evaluări
- 2 Day ALS Programme 24 Candidates IO ARS (March 2016) PDFDocument2 pagini2 Day ALS Programme 24 Candidates IO ARS (March 2016) PDFCojocariu Emanuel50% (2)
- Calcium Cyanide: Hydrogen Cyanide. CONSULT THE NEW JERSEYDocument6 paginiCalcium Cyanide: Hydrogen Cyanide. CONSULT THE NEW JERSEYbacabacabacaÎncă nu există evaluări
- Conut Shell: A Substitute For Aggregate in Mix Proportioning of CementDocument17 paginiConut Shell: A Substitute For Aggregate in Mix Proportioning of CementStephanie SilaoÎncă nu există evaluări
- Why Is ICS Important For Schools?Document8 paginiWhy Is ICS Important For Schools?Spit FireÎncă nu există evaluări
- Northern NVProvider DirectoryDocument82 paginiNorthern NVProvider DirectoryGuru NandeshwarÎncă nu există evaluări
- BFBANFIX - Activity Learning - 01Document2 paginiBFBANFIX - Activity Learning - 01Spheal GTÎncă nu există evaluări
- Pin ContentDocument20 paginiPin ContentSwetha100% (2)
- "Mode One" Author & Dating Coach Alan Roger Currie Releases Criticism of Alleged Harvey Weinstein BehaviorDocument3 pagini"Mode One" Author & Dating Coach Alan Roger Currie Releases Criticism of Alleged Harvey Weinstein BehaviorPR.com100% (1)
- Safety Data Sheet: Rhodamine B (C.I.45170) For MicrosDocument9 paginiSafety Data Sheet: Rhodamine B (C.I.45170) For MicrosSeshagiri KalyanasundaramÎncă nu există evaluări
- Construction of Genomic and cDNA Libraries-AmitDocument10 paginiConstruction of Genomic and cDNA Libraries-AmitPrashant BajpaiÎncă nu există evaluări
- Developments in Injection Moulding 3Document331 paginiDevelopments in Injection Moulding 3Salah HammamiÎncă nu există evaluări
- Minibeasts Differentiated Reading Comprehension ActivityDocument15 paginiMinibeasts Differentiated Reading Comprehension Activitymariam helmyÎncă nu există evaluări
- Boroscope Inspection Procedure 7th Stage StatorDocument15 paginiBoroscope Inspection Procedure 7th Stage StatorAPU SHOP BTH MS100% (2)
- Co JetDocument4 paginiCo JetJaime PaulÎncă nu există evaluări
- Sales Order Process - Key Steps, Attributes and Concepts - v7Document25 paginiSales Order Process - Key Steps, Attributes and Concepts - v7bob bluhmÎncă nu există evaluări
- Carti Libraria Victor Papilian Ian 2015Document8 paginiCarti Libraria Victor Papilian Ian 2015Petru AcozmeiÎncă nu există evaluări
- Program Thành TrungDocument3 paginiProgram Thành TrungQuốc HuyÎncă nu există evaluări
- WhatsApp Chat With Chinnu HeartDocument30 paginiWhatsApp Chat With Chinnu HeartSäi DäťťaÎncă nu există evaluări
- TympanometerDocument12 paginiTympanometerAli ImranÎncă nu există evaluări
- Strip Seal Expansion JointDocument13 paginiStrip Seal Expansion JointsmithÎncă nu există evaluări
- Early Theories On The Origin of Life On Earth: Creation TheoryDocument1 paginăEarly Theories On The Origin of Life On Earth: Creation TheoryAngel Elizaga IIÎncă nu există evaluări