Documente Academic
Documente Profesional
Documente Cultură
DR Case Pres Updated 1
Încărcat de
Ethan NamoDescriere originală:
Drepturi de autor
Formate disponibile
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentDrepturi de autor:
Formate disponibile
DR Case Pres Updated 1
Încărcat de
Ethan NamoDrepturi de autor:
Formate disponibile
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
NORMAL SPONTANEOUS DELIVERY
A Clinical Case Study Presented to the
Faculty of the College of Nursing
Our Lady of Fatima University
Valenzuela City
In Partial Fulfillment of the
Requirements in NCMA217 RLE
Submitted by:
Relado, Irish Lyn D.C.
Romero, Cyrine Mae G.
Ruga, Alexandra Francesca V.
Sabuero, Jannela Paula R.
San Pedro, Patricia Mae N.
Santos, Ethan Troy S.
Sausa, Mythelene O.
Sta. Ana, Rheichelle Anne M.
Tresvalles, Andrea C.
Villarojo, James Edward A.
Wahab, Naiem B.
Submitted to: Evelyn Banaag, RN
1 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
Table of Contents
INTRODUCTION...................................................................................................................... 3-4
OBJECTIVES ................................................................................................................................5
General objectives ........................................................................................................................5
Specific objectives ........................................................................................................................5
PATIENT’S PROFILE .................................................................................................................6
Chief complaint ............................................................................................................................6
History of present illness ..............................................................................................................6
History of past illness ...................................................................................................................6
Family health history ....................................................................................................................6
Personal-social history .................................................................................................................7
Gyne history .................................................................................................................................7
OB history ....................................................................................................................................7
PHYSICAL ASSESSMENT .........................................................................................................8
GORDON’S HEALTH STATUS ........................................................................................... 9-10
TEXTBOOK DISCUSSION .......................................................................................................11
FEMALE EXTERNAL REPRODUCTIVE ORGAN ...............................................................11
FEMALE EXTERNAL REPRODUCTIVE ORGAN ......................................................... 12-14
PATHOPHYSIOLOGY .............................................................................................................15
COURSE IN THE WARD ..........................................................................................................16
LABORATORY RESULTS.................................................................................................. 17-18
NURSING CARE PLAN ....................................................................................................... 19-21
DRUG STUDY ....................................................................................................................... 22-25
DISCHARGE PLANNING ................................................................................................... 26-27
REFERENCES .............................................................................................................................28
PERSONAL DATA ............................................................................................................... 29-30
2 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
INTRODUCTION
Pregnancy is the state of carrying a developing embryo or fetus within the female body.
This condition is confirmed through a blood test, urine test, ultrasound, detection of fetal
heartbeat. It lasts about 40 weeks and can be measured from a woman’s last menstrual period.
(Shiel, 2018) Healthcare providers refer to three segments of pregnancy called trimester. In each
trimester, the fetus will meet specific developmental milestones. For the first trimester, it lasts
for the first 12 weeks of pregnancy and is crucial for the baby’s development. At conception, the
egg and sperm combine to form a zygote, which will implant in the uterine wall, all of the major
organs and structures begin to form. During the first trimester, the woman may experience many
changes such as morning sickness or nausea at 6-8 weeks. For the second trimester, it lasts
between week 13 and 26 of pregnancy. In addition to the major structures and organs, other
important parts of the body will also form during the second trimester. Braxton-Hicks
contractions may start toward the end of the second trimester. Lastly, the third trimester lasts
from week 27 until delivery which is usually around week 40. As the woman gets closer to the
delivery, the baby should turn into a head down position to make birth easier. Anxiety about
delivery and parenthood are also common toward the end of pregnancy. (NICHD, 2016)
In 2016, a total of 1,731,289 live births was registered which is equivalent to a crude
birth rate (CBR) of 16.8 or about 17 births per thousand population.
More males (903,694 or 52.0%) were born than females (827,595 or 48.0%) which
resulted in a sex ratio of 109 males per 100 females.
On the average, there were about 4,730 babies born daily or about 197 babies born per
hour or approximately three babies born per minute.
Almost half (851,088 or 49.2%) of the total registered live births in 2016 were born out
of wedlock. The three regions that recorded the highest number of illegitimate children born in
2016 by usual residence of mother were CALABARZON (135,405), NCR (131,670) and Central
Luzon (92,867).
Normal labor is defined as the gradual subjugation and dilatation of the uterine cervix as
a result of rhythmic uterine contractions leading to the expulsion of the products of conception:
the delivery of the fetus, membranes, umbilical cord, and placenta. Laboring cannot be that easy;
thereby implicating that there are processes and stages to be undertaken to achieve spontaneous
delivery through which obstetrics have divided labor into four stages thereby explaining this
continuous process. (Chinweuba, 2018)
3 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
Stage I is usually the longest part of labor, begin with regular uterine contraction and
ends with complete cervical dilatation at 10cm.
Stage II lasts for three or more hours. However, the length of this stage depends upon the
mother’s position. This stage ends with the expulsion of the fetus.
Stage III focuses on the expulsion of the placenta from the mother. Placenta exclusion is
easier than delivery of the baby because it includes no bones, and this is during this stage that the
baby is placed on top of mother’s womb.
Stage IV does not include any expulsion of conception products for this stage as this is
generally accepted as postpartum juncture. This phase is from the placental delivery to full
recovery of the mother.
Normal Spontaneous Delivery is a natural process that usually does not require
significant medical intervention unlike Caesarean Delivery which involves surgical procedure
(incisions in the abdomen and uterus) to deliver the baby. During normal/vaginal delivery the
primary focus is on how and in which position will the mother be comfortable delivering the
baby. The mother can lead the whole process of labor and delivery. The doctor and attending
nurse aid the mother while being alert for any kind of emergencies. (Berghella, 2018)
The labor and birth process is always accompanied by pain; several options for pain
control are available, ranging from intramuscular or intravenous doses of narcotics; for example,
general anesthesia.
4 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
OBJECTIVES
General Objectives
This case presentation seeks to establish the student knowledge about general health or
condition of the patient with possible complication, some treatment, nursing intervention and
background knowledge about the possible complication.
Specific Objectives
To understand the pathophysiology and etiology of the case presented.
To gather the drug therapy that related to the patient’s diagnosis.
To organize an applicable data that gathered to the case.
Provide effectively suitable and applicable nursing diagnosis related to the client medical
condition and skillfully give formulate a nursing care plan for the case that presented.
To apply suitable nursing intervention required for the patient condition in refence with a
concept to the disease and some learned theories.
To show a skillful in answering the applicable question with positive attitude toward
suggestion and criticism.
5 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
PATIENT’S PROFILE
Vital Information:
Name: Ms. CF
Age: 24
Address: Quezon City
Religion: Iglesia ni Cristo
Nationality: Filipino
Chief Complaint: labor pains
History of Present Illness:
Few hours prior to admission, the patient experienced labor pains, associated with good fetal
movement and watery vaginal discharge. No associated vaginal spotting. Persistence of
symptoms prompted the patient to consult the institution, hence admitted.
History of Past Illness:
(-) hypertension
(-) diabetes mellitus
(-) malignancy
(-) asthma
(-) goiter
(-) surgery
(-) blood transfusion
Family health history:
The patient has no heredofamilial diseases such as hypertension, diabetes mellitus, asthma,
malignancy, and goiter.
6 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
Personal-Social history:
The patient is the 4th of 5 siblings, a college graduate, and unemployed, living-in for 9
months to a 27 year-old security.
Non-smoker
Non-alcoholic beverage drinker
(-) illicit drug use
(-) allergies (medication & food)
Gyne history:
Menarche: 12 years old
Interval: 28-30 days
Duration: 7 days
Amount: 4 pads/day (moderately soaked)
Symptoms: (+) dysmenorrhea
Coitarche: 23 years old
No. of sexual partner: 1
Last sexual contact: December 2018
Contraception: None
OB history:
G1P0
G1 2019, present pregnancy
Prenatal check-up: Lying-in (x7)
Admitting diagnosis: G1P0 pregnancy uterine 39 weeks 1/7 days AOG, cephalic in labor
7 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
PHYSICAL ASSESSMENT
Review of systems
General: patient is coherent with the following VS:
o BP – 110/80
o HR – 75
o RR – 17
o Temperature – 37.2
General: patient didn’t experience loss of appetite, but have a slight weight loss and feeling of
fatigue
Skin: patient’s skin is fair, warm to touch, moist with good skin turgor, with capillary refill time
of <2 seconds
HEENT: patient doesn’t have any headache, neck stiffness, colds, nasal discharge, bleeding
gums, oral ulcer, neck mass, & hoarseness
Respiratory: patient doesn’t have any cough, dyspnea, shortness of breath & pleuritic chest pain
CVS: patient didn’t experienced chest pain, palpitation, orthopnea, paroxysmal nocturnal
dyspnea but experiencing easy fatigability
GIT: patient doesn’t have dysphagia, hematemesis, nausea, vomiting, diarrhea, melena &
hypogastric pain but the patient noted difficulty of regular bowel movement
GUT: patient didn’t experienced dysuria, hematuria, retention, incontinence, frequency, &
urgency
Musculoskeletal: patient doesn’t have myalgia, arthralgia, & arthritis, but experiencing backache
because of giving birth
Endocrine: patient didn’t experienced polyuria, polydipsia, polyphagia, & heat/cold intolerance
Hematologic: patient is not pallor and not easy bruising
Neurologic: patient didn’t have any seizure, dizziness, tremors and hallucination
8 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
GORDON’S HEALTH STATUS
PATTERN BEFORE DURING INTERPRETATION
HOSPITALIZATION HOSPITALIZATION
HEALTH Patient is non-smoker, has Patient increases her Patient increase her values
PERCEPTION negative results for allergies, concern for her health, she and concerns towards her
PATTERN and sees herself healthy takes all her prescribed health
medications (cefuroxime,
methylergometrine maleate,
ferrous sulfate, ascorbic
acid, mefenamic acid)
NUTRITIONAL Patient has good appetite, eats Patient appears to be well Patient meets her proper
-METABOLIC trice a day, thinks she meet nourished nourishment from her food
PATTERN the prescribed water intake a and water intake
Patient is negative for
day
disease that may affect her
nutritional-metabolic
functions
ELIMINATION Patient has no problem Patient stated that she is Patient’s elimination patter
PATTERN regarding her urinary tract freely voiding at a regular changes due to condition
system. range, has improper bowel
excretion
Patient stated that she urinate
and defecate regularly
ACTIVITY/EX Patient’s exercise pattern Patient’s activity decreases Patient cannot function
ERCISE includes doing household due to her condition and normally due to condition
PATTERN chores such as cleaning her hospitalization.
house, cooking, ironing and
doing the laundry.
COGNITIVE- Patient is a college graduate Patient can express herself Patient thinks logically with
PERCEPTUAL clearly and logically regards to her condition
PATTERN
Patient appears to be in a
good state of mind
SLEEP/REST Patient has a normal cycle of Patient was easily disturbed Patient’s condition causes
PATTERN sleep, thinks she meet the during her sleep physical distress that can
normal or prescribed hours of result sleeping problems
sleep
SELF Patient sees herself as Patient sees herself normal Patient appears to be normal
9 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
PERCEPTION/ “chubby” at her condition and has nothing unusual in
SELF- appearance
CONCEPT
PATTERN
ROLE- Patient stated her status as Patient sees her and her Patient is dependent on her
RELATIONSHI single although she has a live- partner’s set up is an live-in partner
P PATTERN in partner important aspect of their
relationship
SEXUALITY/ Patient does not have diseases No changes Patient’s reproductive status
related to her reproductive does not affect her condition
REPRODUCTI functions
VE PATTERN
COPING/ Patient stated that she has low No changes Patient cannot tolerate pain
tolerance for pain well even after her
TOLERANCE hospitalization
PATTERN
VALUE/ Patient has a live-in partner No changes Patient may need her live-in
BELIEFS (security guard) for 9 months partner to be more supportive
whom she consider one of her
PATTERN important support system
10 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
Anatomy & Physiology
Female External Reproductive Organ
Our overview of the reproductive system begins at the external genital area – or vulva –
which runs from the pubic area downward to the anus. The mons pubis is a rounded mass of
fatty tissue that covers the pubic bone which is covered by pubic hair during puberty. The mons
pubis contains sebaceous gland that releases substances that are involved in pheromones (sexual
attraction). The two folds of fatty, fleshy tissue surround the entrance to the vagina and urinary
opening: the labia majora, or outer folds that enclose and protect the other external genital
organs and the labia minora, or inner fold that lie just inside the labia majora and surround the
openings to the vagina and urethra. The clitoris, a very sensitive organ for sexual stimulation and
can become erect that can result in an orgasm. The urethral orifice, which carries urine from the
bladder to the outside located under the clitoris and above the vaginal opening. The vaginal
opening is the entryway for the penis during sexual intercourse and the exit of blood during
menstruation and for the baby during birth. The hymen, a thin membrane protecting the entrance
of the vagina, stretches when you insert a tampon or have sexual intercourse. (Jessica E.
McLaughlin & Jennifer Knudtson, 2019)
11 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
Female Internal Reproductive Organ
The Ovaries
The function of the two ovaries is to produce, mature and discharge ova (the egg cells). In
the process of producing ova, the ovaries also produce estrogen and progesterone and initiate and
regulate menstrual cycles.
The Fallopian Tubes
The fallopian tubes arise from each upper corner of the uterine body and extend outward
and backward until each opens at its distal end, next to an ovary. Their function is to convey the
ovum from the ovaries to the uterus and to provide a place for fertilization of the ovum by the
sperm.
The Uterus
The uterus is a hollow, muscular, pear-shaped organ located in the lower pelvis posterior
to the bladder and anterior to the rectum. In a non-pregnant state, it weighs approximately 60g.
The function of the uterus is to receive the ovum from the fallopian tube; provide a place for
implantation and nourishment; furnish protection to a growing fetus; and, at maturity of the fetus,
expel it to the woman’s body.
12 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
Anatomically, the uterus consists of three divisions: the corpus, the isthmus and the
cervix. The corpus, uppermost part and forms the bulk of the organ. The portion of the uterus
between the points of attachment of the fallopian tube is termed the fundus. During pregnancy,
the corpus is the portion of the structure that expands to contain the growing fetus. The fundus is
the portion that can be palpated abdominally to determine the amount of uterine growth during
pregnancy, to measure the force of uterine contractions during labor, and to assess that the uterus
is returning to its non-pregnant state. The isthmus is the short segment between the body and
cervix. During pregnancy, this portion also enlarges greatly to aid in accommodating the
growing fetus. The cervix is the lowest part of the uterus. Its central cavity is termed the cervical
canal. The opening of the canal at the junction of the cervix and isthmus is the internal cervical
os; the distal opening of the vagina is the external cervical os.
The Vagina
The vagina is a hollow, musculomembranous canal located posterior to the bladder and
anterior to the rectum. It extends from the cervix of the uterus to the external vulva. Its function
is to act as the organ of intercourse and to convey sperm to the cervix. With childbirth, it expands
to serve as the birth canal.
The Physiology of Menstruation
Four body structures are involved in the physiology of menstrual cycle: the
hypothalamus, the pituitary gland, the ovaries, and the uterus. For a menstrual cycle to be
complete all four organs must contribute their part; inactivity of any part results in an incomplete
or ineffective cycle.
During the first half of menstrual cycle, the level of estrogen on the 3rd day is low. It will
stimulate the hypothalamus to release follicle stimulating hormone releasing factor (FSHRF).
After that, FSHRF stimulates anterior pituitary gland to release follicle stimulating hormone
(FSH). This hormone will help oocyte to mature. The FSH stimulates the ovary to release
estrogen, then estrogen converts the follicle from the ovary to Graafian Follicle (GF) and it
causes the thickening of the endometrium of uterus particularly myometrium.
On the 13th day of menstruation the level of estrogen become high and the level of
progesterone is low, it starts the second half of menstruation that will cause stimulation to the
hypothalamus to release luteinizing hormone releasing factor (LHRF). This hormone stimulates
the anterior pituitary gland to release luteinizing hormone (LH). High level of LH stimulates the
ovary to release progesterone & it also stimulates ovulation. This hormone, progesterone –
converts Graafian follicle into corpus luteum that has a lifespan of 2 weeks. Progesterone also
13 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
stimulates the uterus to increase vascularity of endometrium (capillaries gives water, glucose,
oxygen, and amino acid) causing the uterus being fully nourished.
After ovulation, if there is sexual intercourse and fertilization, the woman will expect not
to have her menstrual cycle for the next month. If pregnancy occurs, the corpus luteum’s life
span will extend from 2 weeks to 2 months. After 2 months, corpus luteum cannot support the
growing fetus anymore, so placenta will replace it up to 9th month of the pregnancy. During the
9th month, placenta is already degenerating and aging, it can’t prevent uterine contraction
anymore so the woman is ready for labor and delivery. If no sexual intercourse happen, the
corpus luteum will not extend its life, it will go back to its original form, which is the follicle.
Low estrogen and low progesterone will suggest the uterus to contract and shed off.
14 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
PATHOPHYSIOLOGY
Fertilization (Union of sperm and ovum)
Zygote – Unicellular
(Intermingling of haploid paternal 23 X or Y and maternal 23 X chromosomes)
Series of mitotic cell division - cleavage
(In 24hours become two cell organism)
In 72 hours become 16 cell organism – Morula
Morula enters the uterus on the 3rd day through peristaltic movement
Separate into two parts by fluid from the uterus on the 4th day
The outer layer gave rise The inner layer gave rise to
the placenta (thropoblast) to the embryo (embryoblast)
Blastocysts attaches to endometrium
on the 6th day
Implantation
Embryonic development begins during
2nd week continues through the 8th week
Fetal development is from 9th week to birth
Newborn baby via vaginal delivery
15 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
COURSE IN THE WARD
Date Time Focus Data, action & response
9/01/19 6:15 Prolonged pain D = received on with cast up to femur
A = admitted on 7cm dilate, VS monitored
BP – 110/80
PR – 76
RR – 18
Temperature – 36.2
9/01/19 6:50 Labor pain D = 1 hour from ER accompanied by none via
wheelchair, conscious and coherent, identified
and consent verified
A = assist to LR, placed on bed safely and
comfortably, hooked to NST, monitored FHT,
VS, and progress of labor
9/01/19 Fully dilatation Assist to DR table placed on lithotomy
position
Perineal preparation done
RMLE done by Dr. Cs
Delivered an alive baby by Dr. Cg
Placenta and cord complete
Hooked D5LR to run for 8 hours+ 10IU of
oxytocin
RMLE repair done
Cleanse and padded to recovery room
VS monitored and recorded
For D/C IE
Keep side rails up
Endorsed
9/01/19 12:00 noon Admission Monitor from DR station accepted by NSD
Placed on bed comfortably
On DAT
To start an oral meds
Perineal and genital hygiene instructed
Attended
16 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
LABORATORY RESULTS
PELVIC ULTRASOUND
Ultrasound Findings Result
Number of Fetus Single
Presentation Cephalic
Placenta Posterior HIGH lying placenta, Grade 2 in Maturity
Amniotic Fluid Adequate
Cardiac Rate 1497bpm
Fetal Movement Good
Gender Boy
Estimated date of delivery August 30. 1019
Fetal Parameter Result
Biparietal diameter 87mm 35 weeks 2 days
Head Circumference 305mm 34 weeks 0 days
Abdominal Circumference 328mm 35 weeks 5 days
Femur Length 64mm 33 weeks 3 days
17 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
URINALYSIS
MACROSCOPIC EXAMINATION
TEST RESULT REFERENCE
Color Yellow
Appearance SL - Turbid
PH 6.5 4.5 – 8.0
SP.GR 1.005 <1.040
Glucose Negative Negative
Protein Trace Negative
MICROSCOPIC EXAMINATION
TEST RESULT REFERENCE SIGNIFICANT
WBC 8 – 12 0 – 2 /HPF It may indicate inflammation or
infection
RBC 0–3 0 – 2 /HPF
Epithelial Cell Moderate It may indicate infection
A.Urenate/Phos Few
Mucus Thread Rare
Bacteria Few
18 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
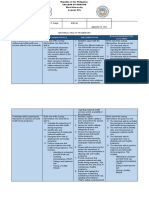
ASSESSMENT DIAGNOSIS BACKGROUND PLANNING INTERVENTION RATIONALE EVALUATIO
KNOWLEDGE N
SUBJECTIVE: Constipation Postpartum After 5 hours INDEPENDENT After 5 hours of
related to constipation, with of nursing nursing
“hindi ako maka -Encourage fluid -Assist in
physiologic symptoms such as intervention, intervention, the
dumi” as intake of 2500- improving
verbalized by changes from pain or discomfort, the patient 3000 ml per day stool patient was be
patient. birth as straining, and hard will be consistency established or
evidence by stool, is a common establish or -Encourage eating return her
improper condition, return her high fiber rich -To enhance normal patterns
bowel affecting mothers. normal foods easy defecation of bowel
OBJECTIVE:
excretion Haemorrhoids, patterns of -Auscultate the -Bowel sounds functioning
BP : 110/80 pain at the bowel bowel sounds are generally
PR : 75 episiotomy site, functioning decreased in
RR : 17 effects of -Determine the
constipation
TEMP : 36.8 pregnancy
stool color,
consistency, -To identify
Weak in hormones and
frequency, and causative
appearance haematinics used
amount factor and
in pregnancy can appropriate
Stool color: increase the risk of -Clean anus
intervention
Dark brown postpartum properly after
constipation performs bowel -To prevent
Consistency: movement infection of
Hard, lumpy, episiotomy
DEPENDENT:
and sausage like
-To defecate
-Discuss the factor
Daily BM: faster
of enema by
Every other day administer of
physician
19 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
ASSESSMENT DIAGNOSIS BACKGROUND PLANNING INTERVENTION RATIONALE EVALUATIO
KNOWLEDGE N
SUBJECTIVE: Alteration in The mother is After 8 hours INDEPENDENT: : To relieve at After 8 hours of
comfort at the experiencing the client’s least a small nursing
“hindi ako : Provide health
perineal are discomfort that discomfort amount of the intervention:
mapakali feeling teaching that
related to could stress the will lessen discomfort and
ko may itchiness is part of The mother’s
episiotomy mother out of and will not prevent
gumagapang sa healing process discomfort will
and frustration and a get worse infection
may ari ko” as lessen and will
episiorrhaphy possible accidental : Clean gently with
verbalized by the continue to
scratch at the soap and cold
patient decrease if said
affected or area of water. Don’t wash
with warm or hot intervention will
discomfort be followed
water because heat
OBJECTIVE: could melt the
“Facial thread
: To prevent
grimacing,
: Tell the patient further
uncontrolled,
that the perineal discomfort and
scratching of
area must not be faster wound
groin from time
touched even if the healing
to time, twitch of
patient has the urge
the legs” :To prevent
to scratch it
spread of
- BP: 110/80
: Tell the client to microorganism
- PR: 75 perform hand s via hand
washing more contact.
- RR: 17 often.
- Temp: 37.2 : Tell the client that
consumption of : Proteins
protein based fluid encourage
such as milk, faster wound
yoghurts, soy based healing.
fluids like taho.
: Neosporin is
DEPENDENT: an antibacterial
ointment that
: use antibacterial encourages
ointments as
healing and
prescribed like
prevents
Neosporin
infection
20 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
ASSESSMENT DIAGNOSIS BACKGROUND PLANNING INTERVENTION RATIONALE EVALUATIO
KNOWLEDGE N
SUBJECTIVE: Fatigue Fatigue an overall After 8 hours *monitor vital *may decrease After 8 hours of
related to feeling of tiredness of nursing signs, noting pulse nervous nursing
“Hindi ako
normal or lack of energy interventions rate at rest and energy, interventions,
makatulog ng
spontaneous when you’re will display when active. promoting the patient was
maayos, wala
delivery as fatigue you have improved relaxation. able to display
akong ganang *note development
evidence by no motivation and ability to improved ability
kumilos of tachypnea, *reduces
inability to no energy. participate in to participate in
pakiramdam ko dyspnea, pallor and stimuli that
desired
ang hina hina ng maintain usual cyanosis. may aggravate desired
activities.
katawan ko” as routines. agitation, activities.
*provide quiet
verbalized by the hyperactivity
environment, cool
patient. and insomnia.
*report an room, decreased
OBJECTIVE: increase in sensory stimuli, *increased
activity soothing colors, irritability of
*Decreased
tolerance quiet music. the CNS may
performance
including cause patient to
*encourage patient
*greater need for activities of be easily
to restrict activity
sleep and rest daily living. excited.
and rest in bed as
*irritability Long term: much as possible. *although help
may be
- Temp:37.2 After months *provide comfort
necessary, self-
of nursing measures like
- PR:75 esteem is
interventions, judicious touch and
enhanced when
- RR:17 the patient; cool showers.
patient does
* is free from *avoid topics that some things for
- BP:110/80
weakness and irritate or upset the self.
risk for patient. Discuss
*encourages
complication ways to respond to
patient to do as
s has been these feelings.
much as
prevented. *identify or possible while
implement energy conserving
saving technique limited energy
like sitting while and preventing
doing a task. fatigue.
21 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
DRUG ACTION INDICATIO CONTRAIN SIDE EFFECTS NURSING PATIENT
NS & DICATION CONSIDERATIO TEACHING
DOSAGE NS
Generic Inhibits cell- -for - Drug may GI: diarrhea, - Patient should - Tell patient to
name: wall uncomplicated appear in pseudomembranous consider take drug as
CEFUROXIM synthesis, skin and skin- breast milk colitis, nausea, temporarily prescribed even if
E ACETIL promoting structure anorexia, vomiting discontinuing feeling better
osmotic infection -Drug may breast-feeding
Brand name: instability; increase risk Hematologic: during the -Warn patient that
Ceftin usually Adult: 250 or of bleeding hemolytic anemia, treatment the bitter taste is
Bactericidal 500mg P.O thrombocytopenia, hard to mask, even
Classification: BID for 10 - -Monitor patient with food.
transient
Antibiotic days. Contraindicat neutropenia, regularly
ed to patients - Instruct patient to
eosinophilia.
Route: - hypersensitiv -Monitor patient notify prescriber
P.O Uncomplicate e to the drug Skin: for signs and about rash, loose
d UTI maculopapular, and symptoms of stools, diarrhea, or
Dose: Adults: 250mg erythematous rashes, superinfection and evidence of
500mg q8 for P.O BID for 7 urticarial, pain, diarrhea superinfection
7 days to 10 days induration
- Inform client to
Other: anaphylaxis, take drug on full
hypersensitivity, stomach
reactions, serum
sickness
22 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
DRUG ACTION INDICATIO CONTRAINDIC SIDE NURSING PATIENT
NS & ATION EFFECTS CONSIDERATIO TEACHING
DOSAGE NS
Generic Ferrous The -Large dose may GI: irritation, -Give between -Tell patient to
name: Sulfate is an prevention or aggravate peptic obstruction, meals with water observe daily
FERROUS essential treatment of ulcer, regional perforation but may give with pattern of bowel
SULFATE enteritis and -Nausea meals if activities and the
component iron
ulcerative colitis -Stomach pain gastrointestinal consistency of the
Brand name: in the deficiency -Urine discomfort occurs stool
Fersulfate Iron formation of anemia due to -Severe Iron discoloration
hemoglobin inadequate Poisoning/Toxicit -Vomiting -Avoid -Take with
Classification: s, diet, y: -Diarrhea simultaneous Ascorbic Acid for
Enzymatic myoglobin malabsorption, vomiting administration of better absorption
Mineral and and pregnancy and severe antacids or
Iron abdominal tetracycline -Egg
enzymes. It blood loss
preparation pain and milk inhibit
is necessary diarrhea absorption
Route: for effective dehydratio
P.O erythropoies n -Monitor serum
is and hyperventi iron, total iron
Dose: transport or lation
1 tab OD utilisation of pallor or -binding capacity,
cyanosis reticulocyte count,
oxygen
cardiovascular hemoglobin and
collapse ferritin
23 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
DRUG ACTION INDICATIO CONTRAIN SIDE EFFECTS NURSING PATIENT
NS & DICATION CONSIDERATIO TEACHING
DOSAGE NS
Generic Like that of - It is used for -This drug is -Abdominal pain. - Monitor vital - Educate patient
name: other the short-term contraindicat -Constipation. signs. about signs of a
Mefenamic NSAIDs, is treatment of ed in patients -Diarrhea. significant reaction
Acid mild to with known -Indigestion. -Assess patients (eg, wheezing;
not
moderate pain hypersensitiv -Gas. who develop severe chest tightness;
Brand name: completely from various ity to -Gross diarrhea and fever; itching; bad
Ponstel understood conditions. mefenamic bleeding/perforation. vomiting for cough; blue skin
but involves acid. -Heartburn. dehydration and color; seizures; or
Classification: inhibition of -It is also used -Nausea. electrolyte swelling of face,
Nonsteroidal cyclooxygen to decrease - imbalance. lips, tongue, or
Anti- ase (COX-1 pain and blood Contraindicat throat).
inflammatory ed to patients -Discontinue drug
and COX- loss from
Drug with kidney promptly if - Instruct patient to
(NSAIDs) 2). It is also menstrual disease. diarrhea, dark report immediately
a potent periods. Start stools and if they experience
Route: inhibitor of this -Should not hematemesis occur. heartburn, nausea,
P.O prostaglandi medication be given to Contact physician. vomiting, diarrhea,
n synthesis when you’re patients who constipation, or
Dose: in vitro. bleeding and -Monitor blood flatulence.
have
1 tab q6 as glucose for loss of
symptoms experienced
needed for glycemic control if
start. asthma, diabetic.
pain
urticaria, or
allergic-type
reactions
after taking
aspirin or
other
NSAIDs.
24 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
DRUG ACTION INDICATIO CONTRAIN SIDE EFFECTS NURSING PATIENT
NS & DICATION CONSIDERATIO TEACHING
DOSAGE NS
Generic name: -Produces -Postpartum Contraindicat CNS: dizziness, - Contractions - Advise patient to
Methylergon vasoconstric hemorrhage ed to patients headache, seizures, begin 5 to 15 stop smoking
ovine maleate tion to and uterine with CVA (with I.V. use), minutes after P.O. during therapy.
Hypertension hallucinations. administration;
increase atony,
Brand name: , heart CV: hypertension, They continue 3 - Warn patient of
Methergine strength, subinvolution. disease, hours or more after adverse reactions.
duration, & transient chest pain,
toxemia, palpitations, P.O. or I.M.
Classification: frequency of pregnancy, administration.
hypotension, bradyc
uterine hypersensitiv
ardia.
semi-synthetic contraction ity, mitral -Monitor patient’s
ergot alkaloid valve EENT: tinnitus, blood pressure,
which in nasal congestion.
stenosis pulse rate, and
turn GI: nausea,
Route: uterine response.
P.O impedes -Cases of vomiting,
uterine threatened diarrhea, foul taste. -Watch for sudden
Dose: blood flow spontaneous GU: hematuria. change in vital
125mg/tab 3x abortion Musculoskeletal: le signs or frequent
a day for 3 g cramps. periods of uterine
days -Must avoid Respiratory: dyspn relaxation.
during ea.
breastfeeding Skin: diaphoresis. -Assess vaginal
Other: thrombophle bleeding.
bitis.
-Store tablets in
tightly closed,
light-resistant
containers. Discard
if discolored.
Breast-feeding
patients
• Ergot alkaloids
inhibit lactation.
• Drug appears in
breast milk, and
ergotism has been
reported in breast-
fed infants.
25 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
DISCHARGE PLANNING
Medications:
Cefuroxime 500mg/cap q8 hours
Methylergometrine maleate 125 mg/ tab q8 hours for 3 days
Ferrous sulfate 325mg/tab OD
Ascorbic Acid 5oo mg/tab q6 hours as needed for pain
Exercise:
1. Encourage the patient to take it easy.
2. Take a stroll frequently as a form of exercise.
3. Avoid places that are stress provoking to facilitate fast recovery of the patient.
4. Advised the patient to gradually return to exercise whenever she feels comfortable
Treatment:
Continue oral medications
Health Teaching:
1. Encourage the patient is to maintain proper hygiene of genital and perineal area
2. Inform the patient to have a follow-up check-up.
3. Encourage the patient to get adequate rest and sleep for fast recovery
4. Encourage the patient to continue breastfeeding .Explain the significant of breastfeeding
and explain how oxytocin assists to keeping the uterus contracted to prevent re
occurrence of post-natal hemorrhage.
Out Patient:
Advise the patient that if she feels any discomfort, pain or encounter any problems during
her recovery period, feel free to come back for a follow up check-up.
Diet:
1. Advised the patient to eat healthy food such as fruits and vegetables and low intake of
fatty food. Salt is okay for patient to add in her food as long as it is not that salty.
2. Advised client to eat food rich in protein to acid in tissue repair since she had post
operation for fast recovery
3. Encourage patient to increase fluid intake to stay hydrated and prevent constipation. 8 to
10 glasses or more of water, milk and juices each day are good choices.
26 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
Spiritual
Encourage the patient to have a family day once a week.
This is a time for them to spend more time with the family and they can also go to the
church together.
27 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
Bibliography
Berghella. (2018, May 17). Mayo Clinic. Retrieved from C-section: https://www.mayoclinic.org/tests-
procedures/c-section/about/pac-
20393655?fbclid=IwAR3TID96kyVamsCTfuioosv1CaSO8NAba8FUCznK2dILxkZsWU12ksL5HS0
Chinweuba. (2018, April 13). Normal Vaginal Delivery: Process, Benefits & Risks. Retrieved from Practo:
https://www.practo.com/health-wiki/normal-vaginal-delivery/152/article
Jessica E. McLaughlin, & Jennifer Knudtson. (2019, April). Female External Genital Organs. Retrieved
from MSD MANUAL: https://www.msdmanuals.com/home/women-s-health-issues/biology-of-
the-female-reproductive-system/female-external-genital-
organs?fbclid=IwAR2z9ZHc8ptBQ4d3XnYmtU8LTw3ZsVrvkYEgi1vpcTxGcO4vFQtQWSPsjN4
NICHD. (2016, May 20). Stages of pregnancy. Retrieved from Office on Women's Health:
https://www.womenshealth.gov/pregnancy/youre-pregnant-now-what/stages-pregnancy
Shiel, W. C. (2018, December 11). Medical Definition of Pregnancy. Retrieved from MedicineNet:
https://www.medicinenet.com/script/main/art.asp?articlekey=11893&fbclid=IwAR1eMKfWsrjh
xD0txlFdqxHF3ijqO5q22D1GrswYdLeUI77tJEgmYWhx9fo
28 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
Irish Lyn D.C. Relado
63 Makabayan St. Brgy. Obrero, QC
09266758246
Irishlynd@gmail.com
Cyrine Mae G. Romero
#10 Macaneneng St. Bagong Barrio, Caloocan City
09275628730
cyrineromerojibang@gmail.com
Alexandra Francesca V. Ruga
Unit 8 Sumapa Bata, Malolos, Bulacan
09673827394
frances.ruga10@gmail.com
Jannela Paula R. Sabuero
15B Policarpio St., San Jose, Navotas City
09053150480
sabjannela@gmail.com
Patricia Mae N. Sanpedro
313 MRH building Balonbato Quezon City
09667239868
sanpedropatricia15@gmail.com
Ethan Troy S. Santos
#17t Mendoza St. Saog Marilou City
09219451263
Ethantroysaints@gmail.com
Mythelene O. Sausa
4 Burgos St. Concepcion, Malabon City
09664715496
sausa.mythelene.o@gmail.com
29 normal spontaneous delivery (5D)
Our Lady of Fatima University
Mac Arthur Highway, Marulas, Valenzuela City
Tel# 291-6538
Rheichelle Anne M. Sta. Ana
Blk 34 Lt 4 Villa Corazon Subd., Guyong, Sta. Maria, Bulacan 3022
09271836176
chengchengm.cm@gmail.com
Andrea C. Tresvalles
4105 Francisco Comp. Gen. T. De leon, Valenzuela City
09257420180
Andreatresvalles21@gmail.com
James Edward A. Villarojo
09360592074
Wahab, Naiem B.
37 Doña josefina village Malhacan Meycauayan Bulacan
09651101776
Bantuas.wahab@gmail.com
30 normal spontaneous delivery (5D)
S-ar putea să vă placă și
- Ovarian Reboot: A Personal Journey to Hormone & Fertility RenewalDe la EverandOvarian Reboot: A Personal Journey to Hormone & Fertility RenewalÎncă nu există evaluări
- Gcs Prolonged Labor 1Document58 paginiGcs Prolonged Labor 1Krishane JustaleroÎncă nu există evaluări
- Case Study (Placenta Previa) This Is It!!!Document68 paginiCase Study (Placenta Previa) This Is It!!!Joeren Gonzales86% (14)
- CP Obward Group 7Document137 paginiCP Obward Group 7janaquintela58Încă nu există evaluări
- Individual Case Study Delivery Room Exposure: (Agusan Del Norte Provincial Hospital, Butuan City)Document13 paginiIndividual Case Study Delivery Room Exposure: (Agusan Del Norte Provincial Hospital, Butuan City)pius troy macapazÎncă nu există evaluări
- GCP FinalDocument79 paginiGCP FinalVIDMENTON PHÎncă nu există evaluări
- Final NSVD Short PaperDocument90 paginiFinal NSVD Short PaperACOB, Jamil C.Încă nu există evaluări
- Final Ob Ward Case StudyDocument41 paginiFinal Ob Ward Case StudyJohn Edward EscoteÎncă nu există evaluări
- Ate MarsDocument30 paginiAte MarsMyla Rojas BalandraÎncă nu există evaluări
- Case Study Labor Room/delivery RoomDocument33 paginiCase Study Labor Room/delivery RoomRhajeeb Aennas Sugala67% (3)
- Incomplete Abortion: A Mini Case Study OnDocument22 paginiIncomplete Abortion: A Mini Case Study OnSunny MujmuleÎncă nu există evaluări
- Case Study, g6Document62 paginiCase Study, g6julie pearl peliyoÎncă nu există evaluări
- BSN 2B 2d CASE STUDY FinalDocument35 paginiBSN 2B 2d CASE STUDY Finalann camposÎncă nu există evaluări
- Maternal NSG ProceduresDocument18 paginiMaternal NSG ProceduresGARCIA, KYLA MAE A.Încă nu există evaluări
- Antenatal Care ProcedureDocument18 paginiAntenatal Care ProcedureNeha SinghÎncă nu există evaluări
- 2M RevisedDocument109 pagini2M RevisedRolland Ray MendozaÎncă nu există evaluări
- Case Study (NSD - Primi)Document29 paginiCase Study (NSD - Primi)Kimberly Anne SP Padilla82% (11)
- Final Obward CPDocument213 paginiFinal Obward CPjanaquintela58Încă nu există evaluări
- Local Media6538270613200334703Document60 paginiLocal Media6538270613200334703Lyca LuatonÎncă nu există evaluări
- Case Study For OB Skills DocxDocument14 paginiCase Study For OB Skills DocxMaica QuilangÎncă nu există evaluări
- Case Study NSVDDocument26 paginiCase Study NSVDFirenze Fil83% (48)
- Normal Spontaneous Delivery With Newborn Care: Nazarenus College and Hospital Foundation IncDocument6 paginiNormal Spontaneous Delivery With Newborn Care: Nazarenus College and Hospital Foundation IncJc GarciaÎncă nu există evaluări
- Final For Grandcaseg3b-2 Case Study-Or DR ComplexDocument34 paginiFinal For Grandcaseg3b-2 Case Study-Or DR ComplexJervy Emiel VALENCIAÎncă nu există evaluări
- Incomplete Abortion MINI CASE STUDY Group 3Document23 paginiIncomplete Abortion MINI CASE STUDY Group 3Katrina TinapianÎncă nu există evaluări
- Maternal and Child Health Nursing I: Pamantasan NG Lungsod NG MaynilaDocument39 paginiMaternal and Child Health Nursing I: Pamantasan NG Lungsod NG MaynilaFrAnz Angel Padera100% (1)
- Molina Sosa2004 PDFDocument4 paginiMolina Sosa2004 PDFKathyRamírezÎncă nu există evaluări
- Tagum Doctors CollegeDocument9 paginiTagum Doctors CollegeAya AringoyÎncă nu există evaluări
- Liceo de Cagayan UniversityDocument36 paginiLiceo de Cagayan Universitypkintanar78597Încă nu există evaluări
- Final Case Presentation Group 9 2nd RotationDocument105 paginiFinal Case Presentation Group 9 2nd Rotationjanaquintela58Încă nu există evaluări
- NSVD Case Study FinalDocument60 paginiNSVD Case Study Finaljints poterÎncă nu există evaluări
- The Best Childbirth Method Is Normal Birth and Water BirthDocument24 paginiThe Best Childbirth Method Is Normal Birth and Water Birthimesha pereraÎncă nu există evaluări
- Incomplete Abortion MINI CASE STUDY (Group 3)Document22 paginiIncomplete Abortion MINI CASE STUDY (Group 3)Twobee Evelyn Claire62% (21)
- Prolonged Labor Incidences: Passage-Passenger Factors Analyzed (Descriptive Study in RSUD Dr. Koesma Tuban)Document5 paginiProlonged Labor Incidences: Passage-Passenger Factors Analyzed (Descriptive Study in RSUD Dr. Koesma Tuban)siska tiaraÎncă nu există evaluări
- Incomplete Abortion Case StudyDocument40 paginiIncomplete Abortion Case StudyLani Michelle BelloÎncă nu există evaluări
- Case AnalysisDocument19 paginiCase Analysisbaka esh toÎncă nu există evaluări
- CS - PP Final..Document30 paginiCS - PP Final..Nicole ArandingÎncă nu există evaluări
- MCN Case Study-2pDocument76 paginiMCN Case Study-2pAngeline ShackletonÎncă nu există evaluări
- Sample Case StudyDocument31 paginiSample Case StudyMary Grace Mas50% (2)
- 2M RevisedDocument109 pagini2M RevisedRolland Ray MendozaÎncă nu există evaluări
- Wesleyan University-Philippines College of Nursing A.Y. 2022-2023Document30 paginiWesleyan University-Philippines College of Nursing A.Y. 2022-2023Jasmin DaclagÎncă nu există evaluări
- DR Write UpDocument29 paginiDR Write UpmaryprincessuyÎncă nu există evaluări
- CS - PP FinalDocument30 paginiCS - PP FinalNicole ArandingÎncă nu există evaluări
- 2222final - Manuscript Group 1Document58 pagini2222final - Manuscript Group 1Jim clarence palmaÎncă nu există evaluări
- A Care Study On Normal Spontaneous Vaginal Delivery Submitted To: Ms. Maria Lowela V. ElopreDocument8 paginiA Care Study On Normal Spontaneous Vaginal Delivery Submitted To: Ms. Maria Lowela V. ElopreJhoi CastroÎncă nu există evaluări
- Ward2 Ppa - CSDocument41 paginiWard2 Ppa - CSfebie pachecoÎncă nu există evaluări
- Ob Ward Case ConDocument14 paginiOb Ward Case ConAnthony Arcenal TarnateÎncă nu există evaluări
- Progression of First Stage LaourDocument14 paginiProgression of First Stage LaourAlmira Dyah PuspitariniÎncă nu există evaluări
- Institute of Nursing Intrapartum Care Handouts: Labor and Delivery Theories of Labor OnsetDocument7 paginiInstitute of Nursing Intrapartum Care Handouts: Labor and Delivery Theories of Labor OnsetTimi BCÎncă nu există evaluări
- Ojog 2023012915234980Document10 paginiOjog 2023012915234980MICHAEL KEPSEUÎncă nu există evaluări
- MS GCS Cornual Ectopic PregnancyDocument57 paginiMS GCS Cornual Ectopic PregnancyCarelle Faith Serrano AsuncionÎncă nu există evaluări
- Placenta AbruptionDocument86 paginiPlacenta AbruptionXena IngalÎncă nu există evaluări
- Group 3 Hyperemesis Gravidarum FinalDocument75 paginiGroup 3 Hyperemesis Gravidarum FinalJulhanie K. MatalamÎncă nu există evaluări
- Obc - L D JournalDocument4 paginiObc - L D Journalapi-546488467Încă nu există evaluări
- Pity for Evil: Suffrage, Abortion, and Women’s Empowerment in Reconstruction AmericaDe la EverandPity for Evil: Suffrage, Abortion, and Women’s Empowerment in Reconstruction AmericaÎncă nu există evaluări
- Untitled DocumentDocument2 paginiUntitled DocumentEthan NamoÎncă nu există evaluări
- Health ProblemDocument3 paginiHealth ProblemEthan NamoÎncă nu există evaluări
- Health ProblemDocument3 paginiHealth ProblemEthan NamoÎncă nu există evaluări
- Drug Study..Document2 paginiDrug Study..Ethan NamoÎncă nu există evaluări
- Survey Form (Baja, Joan R. BSN Ii-G)Document32 paginiSurvey Form (Baja, Joan R. BSN Ii-G)Beverly DatuÎncă nu există evaluări
- MCHN - NCM 109 A First Assignment For Midterm Coverage Section Ii-BDocument9 paginiMCHN - NCM 109 A First Assignment For Midterm Coverage Section Ii-BRoshin TejeroÎncă nu există evaluări
- RUQYAH AND MEDICINE by Sheilkabdul RaoufDocument3 paginiRUQYAH AND MEDICINE by Sheilkabdul RaoufAhmed MagajiÎncă nu există evaluări
- BSN 2 7 - Group DDocument8 paginiBSN 2 7 - Group DCrystal MiranaÎncă nu există evaluări
- Antenatal CareDocument3 paginiAntenatal CareSimranÎncă nu există evaluări
- Cesárea CerdosDocument6 paginiCesárea CerdosViviana RuedaÎncă nu există evaluări
- Training Curriculum For Traditional Birth Attendants-528Document53 paginiTraining Curriculum For Traditional Birth Attendants-528National Child Health Resource Centre (NCHRC)86% (7)
- EmbrionageDocument15 paginiEmbrionageJohana S. Villegas BuenoÎncă nu există evaluări
- Quiz 1 AntepardumDocument2 paginiQuiz 1 Antepardumchase nicholsÎncă nu există evaluări
- The Midwifery ProfessionDocument23 paginiThe Midwifery ProfessionFpj TarrobalÎncă nu există evaluări
- Digital CABNEI International Conference AbstractbookDocument110 paginiDigital CABNEI International Conference AbstractbookWardiati Yusuf100% (1)
- Module No. 3 Discomforts of Pregnancy (Midterm Period)Document11 paginiModule No. 3 Discomforts of Pregnancy (Midterm Period)maryann uncianoÎncă nu există evaluări
- Maternal Health FrameworkDocument6 paginiMaternal Health FrameworkTrisha Faye OrtegaÎncă nu există evaluări
- Why Abortion Should Be LegalizedDocument1 paginăWhy Abortion Should Be LegalizedKilles SmileÎncă nu există evaluări
- Implementing Rules and Regulations ofDocument96 paginiImplementing Rules and Regulations ofruzsi07Încă nu există evaluări
- Miso Fact Sheet ENG-2016Document4 paginiMiso Fact Sheet ENG-2016Hoplar DoreenÎncă nu există evaluări
- University of The Cordilleras College of NursingDocument1 paginăUniversity of The Cordilleras College of NursingRaniel Zachary CastaÎncă nu există evaluări
- Causes of Mental RetardationDocument6 paginiCauses of Mental RetardationflaxulinationÎncă nu există evaluări
- Anemia 2021Document40 paginiAnemia 2021Gwyneth FisherÎncă nu există evaluări
- Study Guide CP PHC IDocument4 paginiStudy Guide CP PHC IChristopher BañezÎncă nu există evaluări
- Module 2 OB Ward CLMMRHDocument5 paginiModule 2 OB Ward CLMMRHKristil ChavezÎncă nu există evaluări
- EctopicDocument41 paginiEctopicVillanueva Ameera MaeÎncă nu există evaluări
- Iron Deficiency AnemiaDocument16 paginiIron Deficiency AnemiaBibin Panicker100% (1)
- ANC Guideline PresentationDocument42 paginiANC Guideline PresentationDeepak BamÎncă nu există evaluări
- Maternal and Child NursingDocument30 paginiMaternal and Child NursingJack Bisarra Sanchez0% (1)
- Pro Choice SpeechDocument2 paginiPro Choice Speechme_el_st100% (1)
- Answer Key Intraboard BDocument14 paginiAnswer Key Intraboard BJonas Marvin Anaque100% (3)
- IUGRDocument10 paginiIUGRAiman ArifinÎncă nu există evaluări
- Hyperthyroidism During Pregnancy: Etiology, Diagnosis and ManagementDocument9 paginiHyperthyroidism During Pregnancy: Etiology, Diagnosis and ManagementAdi PratamaÎncă nu există evaluări
- Krok!!2023 JanDocument33 paginiKrok!!2023 JanhussainÎncă nu există evaluări