Documente Academic
Documente Profesional
Documente Cultură
Nephrolithiasis: in The Clinic
Încărcat de
JohnTitlu original
Drepturi de autor
Formate disponibile
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentDrepturi de autor:
Formate disponibile
Nephrolithiasis: in The Clinic
Încărcat de
JohnDrepturi de autor:
Formate disponibile
acp-clinic0908 7/20/09 3:28 PM Page 1
in the clinic
in the clinic
Nephrolithiasis
Screening and Prevention page ITC2-2
Diagnosis page ITC2-3
Acute Treatment page ITC2-6
Preventive Treatment page ITC2-8
Practice Improvement page ITC2-14
CME Questions page ITC2-16
Section Editors The content of In the Clinic is drawn from the clinical information and
Christine Laine, MD, MPH education resources of the American College of Physicians (ACP), including
Sankey V. Williams, MD PIER (Physicians’ Information and Education Resource) and MKSAP (Medical
Knowledge and Self-Assessment Program). Annals of Internal Medicine
Physician Writer editors develop In the Clinic from these primary sources in collaboration with
David S. Goldfarb, MD the ACP’s Medical Education and Publishing Division and with the assistance
of science writers and physician writers. Editorial consultants from PIER and
MKSAP provide expert review of the content. Readers who are interested in these
primary resources for more detail can consult http://pier.acponline.org and other
resources referenced in each issue of In the Clinic.
The information contained herein should never be used as a substitute for clinical
judgment.
CME objective: To review the screening and prevention, diagnosis, acute and
preventive treatment, and practice improvement for nephrolithiasis.
© 2009 American College of Physicians
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 2
s many as 13% of men and 7% of women in the United States will
A have at least 1 kidney stone. Recent evidence suggests that the preva-
lence of kidney stones is increasing (1), perhaps because they are as-
sociated with hypertension, diabetes, obesity, chronic kidney disease, and the
metabolic syndrome (2, 3). Between 1994 and 2000, outpatient visits for
stone disease increased by 40%, and office visits increased by 43%. Stones re-
cur frequently, with 50% of patients having a second stone within 5 years of
the first one, and 80% having a second stone within 20 years. Kidney stones
are expensive because urologic interventions are required for as many as 20%
of episodes of renal colic. In addition, about 1% of the working population
will be affected by stones in a given year, causing substantial indirect expense
to employers through lost productivity (4). Stones can and should be pre-
vented. Yet many urologists and nephrologists believe that most patients are
not evaluated and not given appropriate advice or therapy, although data on
this issue are lacking.
Screening and
Prevention What factors increase the risk for
nephrolithiasis?
implicated in altering urine com-
position to favor stone formation.
Genetic and environmental influ- Decreased dietary calcium content
ences cause kidney stones. More has been associated with the risk
than 50% of patients in kidney for stones, probably because di-
stone clinics have a first-degree etary calcium can precipitate in-
relative with stones. The most testinal oxalate and prevent its ab-
common urinary phenotype in pa- sorption from the intestine, thus
tients with stones and with family reducing oxalate excretion in the
1. Stamatelou KK, Fran-
cis ME, Jones CA, et histories of stones is hypercalci- urine. Low urine volume leads to
al. Time trends in re-
ported prevalence of uria. Kidney stones in both mem- increased concentration of stone-
kidney stones in the bers of a twin pair occur at twice forming calcium salts and uric
United States: 1976-
1994. Kidney Int. the rate in monozygotic twins ver- acid, so lifeguards, athletes, sol-
2003;63:1817-23.
[PMID: 12675858]
sus dizygotic twins (5). Calcula- diers (especially those deployed to
2. Taylor EN, Stampfer tions based on twin studies hot climates), and others with in-
MJ, Curhan GC. Obe-
sity, weight gain, and estimate that 56% of the stone creased sweating have reduced
the risk of kidney phenotype is accounted for by ge- urine volume and increased rates
stones. JAMA.
2005;293:455-62. netic factors and the rest is envi- of stones. Drivers and teachers
[PMID: 15671430]
3. Daudon M, Traxer O, ronmental. The genes responsible have lower fluid intake and ex-
Conort P, et al. Type 2 for these genetic effects, however, crete more concentrated urine.
diabetes increases
the risk for uric acid have not been identified. Oxalobacter formigenes is an intes-
stones. J Am Soc
Nephrol.
tinal bacterium that metabolizes
2006;17:2026-33. Environmental factors or acquired oxalate. Colonization with Ox-
[PMID: 16775030]
4. Saigal CS, Joyce G,
traits are presumably responsible alobacter may reduce oxalate ab-
Timilsina AR; Urologic for the increase in stone preva- sorption from the colon, reduce
Diseases in America
Project. Direct and in- lence observed in the past 20 urinary oxalate, and protect
direct costs of
nephrolithiasis in an
years. For example, stones are against stones. Antibiotics may
employed popula- strongly associated with weight eliminate this organism, thus in-
tion: opportunity for
disease manage- gain, diabetes, obesity, and the creasing oxalate absorption from
ment? Kidney Int.
2005;68:1808-14.
metabolic syndrome, which are the intestine and oxalate excretion
[PMID: 16164658] occurring more frequently. Dia- into the urine (6). However, it is
5. Goldfarb DS, Fischer
ME, Keich Y, et al. A betes is a strong risk factor for not clear if Oxalobacter prepara-
twin study of genetic both calcium and uric acid stones. tions, which are not yet available
and dietary influ-
ences on nephrolithi- Whether, hypertension is a risk commercially, can prevent kidney
asis: a report from the
Vietnam Era Twin
factor for stones is unclear. In- stones by reducing urinary oxalate
(VET) Registry. Kidney creases in dietary salt, oxalate, and levels. Urinary tract infections as-
Int. 2005;67:1053-61.
[PMID: 15698445] animal protein have been sociated with high urine pH,
© 2009 American College of Physicians ITC2-2 In the Clinic Annals of Internal Medicine 4 August 2009
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 3
particularly with urease-producing stones unresponsive to usual
organisms, such as Proteus species, therapy.
are important risk factors for stru-
vite stones. Bowel disorders, such What measures should clinicians
as inflammatory bowel disease or recommend to prevent
nephrolithiasis in patients at
the short-bowel syndrome, are
increased risk?
associated with enteric hyperox-
Increased fluid intake dilutes the
aluria and calcium oxalate stones, urine and decreases urinary super-
and low urine pH due to bowel saturation of poorly soluble salts,
fluid loss is associated with uric such as calcium oxalate and uric
acid stones. Bariatric surgery caus- acid. Increased fluid intake is safe
es hyperoxaluria and stones (7). and inexpensive and can be recom-
Some medications can cause mended to patients at increased
stones, including calcium supple- risk. Although no trials of primary
ments (8) (as opposed to increased prevention have been performed,
dietary calcium [9]); high-dose increased fluid intake has been
vitamin C; and poorly soluble shown effective in 1 trial of second-
drugs, such as triamterene or fel- ary prevention.
bamate. Carbonic anhydrase in-
Higher fluid intake with higher urine vol-
hibitors like acetazolamide, which
ume as secondary prevention was associ-
is used for glaucoma, or topira- ated with a lower rate of stone recurrence
mate, which is used for epilepsy in calcium oxalate stone–forming pa-
and migraine, also cause kidney tients. Patients with calcium stones were
stones by increasing urine pH and advised to increase fluid intake, whereas a
decreasing citrate excretion. control group was not given this advice.
After 5 years, the group with high fluid in-
Should clinicians screen patients take had a mean daily urine volume of 2.6 L
for asymptomatic stones if they compared with 1.0 L in the control group,
and 12% of the group with high fluid in-
are at increased risk for
take had a recurrent stone compared with
nephrolithiasis? 27% of the control group (8).
No evidence supports the screen-
ing of patients for asymptomatic Changes in diet are best reserved 6. Kaufman DW, Kelly JP,
Curhan GC, et al. Ox-
stones unless they have recurrent for secondary prevention. alobacter formigenes
may reduce the risk
of calcium oxalate
kidney stones. J Am
Screening and Prevention... Genetic factors increase the risk for stones, but Soc Nephrol.
2008;19:1197-203.
most stones cannot be linked to a specific genetic defect. Increased dietary salt, [PMID: 18322162]
oxalate, and animal protein are associated with stone formation, as are specific 7. Lieske JC, Kumar R,
medical conditions and some drugs. Patients should not be screened for asympto- Collazo-Clavell ML.
Nephrolithiasis after
matic stones even if they are at increased risk. Patients at increased risk for bariatric surgery for
stones should be encouraged to increase fluid intake to more than 2 to 2.5 L/d obesity. Semin
Nephrol. 2008;28:163-
(68 to 85 oz/d) to maintain urine volume greater than 2 L/d. 73. [PMID: 18359397]
8. Borghi L, Meschi T,
Amato F, et al. Urinary
CLINICAL BOTTOM LINE volume, water and
recurrences in idio-
pathic calcium
nephrolithiasis: a 5-
Diagnosis year randomized
prospective study. J
Urol. 1996;155:839-43.
[PMID: 8583588]
What is the spectrum of lodged at the ureteropelvic junction 9. Lauderdale DS, Thist-
presentation for patients with (10.6%) produce flank pain, stones ed RA, Wen M, et al.
Bone mineral densi-
nephrolithiasis? lodged between the ureteropelvic ty and fracture
Most patients have flank pain that junction and the iliac vessels among prevalent
kidney stone cases
radiates downward and anteriorly (23.4%) produce flank pain with in the Third National
Health and Nutrition
into the abdomen and then into radiation to the genitals, and stones Examination Survey.
the pelvis and genitals as stones lodged at the ureterovesical junc- J Bone Miner Res.
2001;16:1893-8.
progress down the ureter. Stones tion (60.6%) produce voiding [PMID: 11585355]
4 August 2009 Annals of Internal Medicine In the Clinic ITC2-3 © 2009 American College of Physicians
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 4
urgency and suprapubic discomfort flank pain, but fever is expected.
(10). Stones may less frequently Pyelonephritis and stones some-
lodge at the bladder neck and cause times coexist, however. In women,
suprapubic discomfort and anuria. a pelvic examination may suggest
Patients with a history of renal col- ovarian torsion, cysts, or ectopic
ic usually make the diagnosis cor- pregnancy. In men, a rectal exami-
rectly themselves. The pain often nation may identify prostatic hy-
starts rapidly and waxes and wanes. pertrophy, prostatitis, or prostate
Nausea and vomiting are often cancer with lower urinary tract
present, and fever is absent. Gross symptoms that may be mistaken
or microhematuria may be present. for obstructing stones.
Smaller stones that only partially
obstruct the ureter may present What imaging studies and
with mild discomfort. Stone pas- laboratory tests should clinicians
sage is associated with dramatic use to confirm the diagnosis of
and sudden cessation of pain. Stru- nephrolithiasis?
vite stones often do not cause flank Computed tomography (CT) is the
pain, because they remain intra- gold standard for the diagnosis of
renal and may not cause obstruc- renal colic. It has superior sensitiv-
tion, and a struvite stone can ity and specificity to ultrasonogra-
remain asymptomatic until the phy and intravenous pyelography
urinary tract infection that caused (IVP). Calcium stones are radio-
it becomes symptomatic. Asympto- opaque, cystine and struvite stones
matic stones are often detected are often but not always radio-
during imaging studies for unre- opaque, and uric acid stones are
lated indications. never opaque unless they include a
calcium component. Therefore,
How should clinicians use history noncalcium stones may be missed
and physical examination to by plain radiography and visualized
evaluate patients with suspected by CT. Computed tomography is
10. Eisner BH, Reese A, nephrolithiasis? also better at making alternative
Sheth S, et al. Ureter-
al stone location at
The history should concentrate on diagnoses when ureteral stones are
emergency room establishing risk factors for stones, not present. Because CT does not
presentation with
colic. J Urol. including the family history, occu- require contrast, it is faster and
2009;182:165-8.
[PMID: 19450856]
pational status, diet, medications, safer than IVP. Although the price
11. Longo J, Akbar SA, supplements, and other medical has fallen in recent years, CT is
Schaff T, et al. A
prospective compar- conditions. A history of other kid- still more expensive than other
ative study of non- ney or urologic conditions, such as modalities, particularly because
contrast helical com-
puted tomography polycystic kidney disease or urinary pelvic and abdominal studies are
and intravenous uro-
gram for the assess-
tract infection, should be elicited. usually billed separately. Plain radi-
ment of renal colic. Past bowel disease, sarcoidosis, and ography of the abdomen is inex-
Emerg Radiol.
2001;8:285-92. hyperparathyroidism are also risk pensive, usually detects calcium
12. Ferrandino MN,
Bagrodia A, Pierre
factors. stones 5 mm or bigger, identifies
SA, et al. Radiation
exposure in the The physical examination is most some nonstone diagnoses, and has
acute and short-
important for ruling out other con- a low dose of radiation. Magnetic
term management
of urolithiasis at 2
ditions. Kidney stones have no spe- resonance imaging is a poor tool
academic centers. J
Urol. 2009;181:668- cific manifestations on examination. for visualizing stones.
72; discussion 673.
[PMID: 19100573] In a prospective evaluation of radiologic im-
13. Poletti PA, Platon A, What other disorders should
Rutschmann OT, et aging in renal colic, 168 patients had both
al. Low-dose versus clinicians consider in patients noncontrast helical CT and IVP (11). Com-
standard-dose CT with suspected nephrolithiasis? parison of CT findings with the final diagno-
protocol in patients
with clinically sus- Patients with conditions associated sis of stone showed 98% sensitivity, 95%
pected renal colic.
AJR Am J
with peritonitis have fever, abdomi- specificity, 98% positive predictive value, and
Roentgenol. nal tenderness, guarding, and re- 95% negative predictive value. Intravenous
2007;188:927-33.
[PMID: 17377025] bound. Pyelonephritis may cause pyelography had inferior results, with 83%
© 2009 American College of Physicians ITC2-4 In the Clinic Annals of Internal Medicine 4 August 2009
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 5
sensitivity, 95% specificity, 97% positive pre- chest radiography and measurement
dictive value, and 67% negative predictive of parathyroid hormone may be ap-
value. Computed tomography was also su- propriate. A low serum bicarbonate
perior in detecting nonstone causes of pain. concentration with a urine pH of 6.0
Some stone-forming patients receive or more suggests renal tubular acido-
repeated doses of radiation. In 1 ret- sis (RTA). Hypophosphatemia is seen
rospective study, 108 patients with a in some patients with a renal phos-
primary acute stone episode under- phate leak and calcium stones. High
went an average of 4 radiographic urine pH or pyuria should lead to
examinations during a 1-year period. urine cultures and consideration of
Studies included a mean of 1.2 plain struvite stones.
abdominal films, 1.7 abdominal and How and when should clinicians
pelvic CTs (range 0 to 6), and use specialized laboratory testing
1 IVP (range 0 to 3) during the to determine the cause of
first year of follow-up (12). In an nephrolithiasis?
attempt to minimize radiation expo- More detailed analyses, such as 24-
sure for these patients, new proto- hour urine collections for measure-
cols and imaging techniques for ment of chemistries, are usually
low-dose CT are being developed reserved for patients with recurrent
and have become the standard of stones, children with stones, and
care at many institutions. Low-dose perhaps patients whose first stones
stone-protocol CT seems nearly as are larger and require urologic
effective as standard helical CT for inter vention. Clinicians can use
detection of stones and abdominal these 24-hour urine collections to
pathology in patients who are not identify risk factors for recurrent
morbidly obese (13, 14). stone formation that are then used
When evaluating acute renal colic, to prescribe specific diet and phar-
14. Zagoria RJ, Dixon RL.
obtain a complete blood count, a macologic interventions, although Radiology of urolithi-
asis: implications of
urinalysis, and serum chemistries. no randomized, controlled trials radiation exposure
Complete blood count and urinalysis (RCTs) have shown that this ap- and new imaging
modalities. Adv
are useful for detecting concomitant proach is superior to others (17). Chronic Kidney Dis.
2009;16:48-51.
infection, but hematuria may be ab- Use a laboratory that calculates su- [PMID: 19095205]
sent in acute stone disease. Serum persaturation, which is a ratio of 15. National Institutes of
Health Consensus
chemistries are important for detect- the patient’s ion activity product to Development Con-
ference on Preven-
ing underlying renal dysfunction as- the known solubility product for tion and Treatment
sociated with urinary tract obstruc- the crystal-forming solute in ques- of Kidney Stones.
Bethesda, Maryland,
tion or alterations in extracellular tion. Higher values are associated March 28-30, 1988. J
volume associated with vomiting. with greater stone-forming tenden- Urol. 1989;141:705-
808. [PMID: 2645426]
cy. Supersaturation combines urine 16. Tiselius HG, Acker-
mann D, Alken P, et
Although not recently updated, the volume with concentrations of al; Working Party on
National Institutes of Health consen- calcium, oxalate, citrate, and other Lithiasis, European
Association of Urolo-
sus statement suggested routine labo- variables into a single value that gy. Guidelines on
urolithiasis. Eur Urol.
ratory analyses for first-time stone- suggests the likelihood of recur- 2001;40:362-71.
forming patients to identify risk rence, correlates well with stone [PMID: 11713390]
17. Parks JH, Asplin JR,
factors for recurrent stones (15). More composition (18) and is intuitively Coe FL. Patient ad-
herence to long-
recent guidelines from the European understandable by patients. Deter- term medical treat-
Association of Urology are not sub- mining stone composition by in- ment of kidney
stones. J Urol.
stantially different (16). In the elective frared spectroscopy or X-ray crystal- 2001;166:2057-60.
[PMID: 11696706]
office-based setting, this evaluation lography is inexpensive, aids in 18. Asplin J, Parks J,
should include serum electrolytes, understanding the pathophysiology Lingeman J, et al.
Supersaturation and
blood urea nitrogen, creatinine, calci- of the stone formation, and helps stone composition
in a network of dis-
um, phosphorus, and uric acid. Hy- plan prevention. About 80% of persed treatment
percalcemia suggests sarcoidosis or stones contain calcium, and about sites. J Urol.
1998;159:1821-5.
primary hyperparathyroidism, and 80% of calcium stones are composed [PMID: 9598467]
4 August 2009 Annals of Internal Medicine In the Clinic ITC2-5 © 2009 American College of Physicians
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 6
mostly of calcium oxalate. The rest Patients should have a screen to
are calcium phosphate. Uric acid urinate through in the hospital or
stones account for up to 10%, with at home to capture stones or frag-
a higher proportion in obese pa- ments for analysis. Instruct patients
tients and patients with diabetes, to urinate into a cup with a 4 × 4
and struvite stones are more com- gauze pad if a screen designed for
mon in women. Cystine stones the purpose of capturing stones or
account for about 1% of stones. fragments is not available.
Diagnosis... Computed tomography without contrast is the best method for di-
agnosing the cause of renal colic. Repeated episodes lead to repetitive expo-
sure of patients to radiation, and ultrasonography is preferred for serial follow-
up. Many stones can be diagnosed by plain radiography, and ultrasonography is
good for demonstrating hydronephrosis, although ureteral stones below the
kidney are often missed. When evaluating acute renal colic, obtain a complete
blood count; urinalysis; and levels of serum electrolytes, blood urea nitrogen,
creatinine, calcium, phosphorus, and uric acid to manage the acute episode
and to evaluate the patient for preventive therapy. To guide the choice of pre-
ventive therapy, measure stone composition in all patients and measure urine
supersaturation in 24-hour urine collections of patients with recurrent stones,
children with stones, and perhaps patients whose first stones are large and
require urologic intervention.
CLINICAL BOTTOM LINE
Acute
Treatment How should clinicians treat pain
in patients with renal colic?
required less “rescue analgesia,” and had few-
er adverse effects (20).
Opiates or nonsteroidal anti-
Which drugs aid the passage of
inflammatory drugs are used alone
renal stones?
or in combination for moderate-to-
Patients with distal ureteral
severe pain. Ketorolac provides ef-
stones less than 10 mm in diame-
fective pain relief with less sedation ter can be treated with tamsu-
than opiates and, therefore, is pre- losin, an α 1-adrenergic antagonist
ferred for patients who are dis- usually used for benign prostatic
charged from the emergency de- hypertrophy, to aid stone passage.
partment before a stone has passed. Tamsulosin is well-tolerated but
Among opiates, meperidine causes infrequently lowers blood pres-
more nausea and vomiting and is sure, leading to lightheadedness
contraindicated in the presence of or dizziness. A second choice is
decreased kidney function. nifedipine, a calcium-channel
19. Larkin GL, Peacock blocker that presumably causes
WF 4th, Pearl SM, et In a double-blind RCT of ketorolac, 60 mg
al. Efficacy of ketoro- ureteral dilatation and relaxation,
lac tromethamine intramuscular, versus meperidine, 100 to
versus meperidine in
although this drug is more often
150 mg intramuscular based on weight, in 70
the ED treatment of associated with undesirable low-
acute renal colic. Am patients with renal colic, ketorolac gave bet-
J Emerg Med. ter pain relief and led to slightly quicker dis-
ering of blood pressure. These 2
1999;17:6-10.
[PMID: 9928687] charge from the emergency department (19). drugs have not been compared
20. Safdar B, Degutis LC,
In another RCT of 130 patients with renal col- with each other. The trials that
Landry K, et al. Intra-
venous morphine ic, patients received either intravenous mor- used nifedipine for this indica-
plus ketorolac is su-
phine, 5 mg and then another 5 mg after 20 tion also used concomitant gluco-
perior to either drug
alone for treatment minutes; intravenous ketorolac, 15 mg and corticosteroids, such as methyl-
of acute renal colic.
Ann Emerg Med. then another 15 mg after 20 minutes; or a prednisolone. Steroids and
2006;48:173-81, combination of both. The combination was non-steroidal anti-inflammatory
181.e1.
[PMID: 16953530] superior to either drug alone for pain relief, drugs may reduce stone-induced
© 2009 American College of Physicians ITC2-6 In the Clinic Annals of Internal Medicine 4 August 2009
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 7
ureteral edema to aid stone pas- occur. Urinary tract infection with
sage. Whether nifedipine and obstruction is the most urgent in-
steroids are effective separately dication for hospitalization and
or only together has not been urologic consultation.
established.
When should clinicians consider
When should clinicians hospitalize lithotripsy, surgery, or other
patients with nephrolithiasis? interventions in the acute
Consider hospitalization for pa- management of patients with
tients with stones larger than nephrolithiasis?
5 mm if parenteral therapy is re- Usually, urologists will decide
quired to manage pain. Admit pa- whether a procedure will be done
tients with stones of any size if and which procedure will be used.
pain or nausea and vomiting can- The choice often depends on the
not be managed in the outpatient urologist’s assessment and skills and
setting. Smaller stones (<5 mm) the patient’s preference. The AUA’s
are likely to pass without surgical Ureteral Stones Clinical Guidelines
intervention, whereas larger stones Panel and the European Association
are more likely to be associated of Urology (22) recommend extra-
with a prolonged course, more corporeal shock wave lithotripsy
pain, and a lower likelihood of (ESWL) as first-line treatment for
spontaneous passage. stones no larger than 1 cm in diam-
A meta-analysis of 327 studies by the Ureter-
eter in the proximal ureter;
al Stones Clinical Guidelines Panel convened ureteroscopy and percutaneous
by the American Urologic Association (AUA) nephrolithotomy are acceptable al-
found that 98% of smaller stones (<5 mm) ternatives, especially if ESWL is
passed spontaneously. Distal ureteral stones inappropriate or fails. For stones
passed more frequently than proximal larger than 1 cm in diameter in the
ureteral stones (21). proximal ureter, consider percuta-
neous nephrolithotomy or
An obstructed and infected uri-
ureteroscopy. For distal ureteral
nary tract is an absolute indication
stones no larger than 1 cm in diam-
for emergent intervention, because
eter, choose ESWL or ureteroscopy
this condition can lead to urosep-
instead of blind basketing without
sis and irreversible renal parenchy-
fluoroscopy. For distal ureteral
mal damage. Concomitant urinary
stones greater than 1 cm, perform
tract infection is suggested by
ESWL or ureteroscopy; although
fever or pyuria (>5 to 20 leuko-
for larger stones, ureteroscopy may
cytes per high-powered field) or
be more appropriate because ESWL
substantial leukocytosis. Also, ad-
must fragment stones into smaller
mit patients with bilateral ob-
struction or obstruction in a soli- pieces to be successful. Ureteroscopy
tary kidney if decreased kidney may lead to better clearance of stone 21. Segura JW, Pre-
function is evident. Administer fragments, which minimizes stone minger GM, Assimos
DG, et al. Ureteral
antibiotics promptly on the basis recurrence. For patients with stones Stones Clinical
of local sensitivity patterns. who are undergoing ESWL, consid- Guidelines Panel
summary report on
er subsequent treatment with tam- the management of
ureteral calculi. The
When should clinicians consult a sulosin to aid passage of stone American Urological
urologist or other specialist? fragments. The AUA recommenda- Association. J Urol.
1997;158:1915-21.
Consult a urologist for stones tions regarding the management of [PMID: 9334635]
22. Preminger GM,
larger than 5 mm or those that staghorn calculi suggest that percu- Tiselius HG, Assimos
prevent patients from conducting taneous nephrolithotomy should be DG, et al; EAU/AUA
Nephrolithiasis
their normal activities. Consult a the first treatment used for most Guideline Panel.
2007 guideline for
urologist for stone removal when patients, and that ESWL mono- the management of
the likelihood of spontaneous pas- therapy should not be used for most ureteral calculi. J
Urol. 2007;178:2418-
sage is low or when complications patients. 34. [PMID: 17993340]
4 August 2009 Annals of Internal Medicine In the Clinic ITC2-7 © 2009 American College of Physicians
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 8
Acute Treatment... Use opiates or nonsteroidal anti-inflammatory drugs alone or
in combination for moderate-to-severe pain. Patients with distal ureteral stones
less than 10 mm in diameter can be treated with tamsulosin or nifedipine to aid
stone passage. Consider hospitalization for patients with stones larger than 5 mm
if parenteral therapy is required to manage pain. Admit patients with stones of
any size if pain or nausea and vomiting cannot be managed in the outpatient set-
ting. Consult a urologist for stones larger than 5 mm or stones that prevent pa-
tients from conducting their normal activities. Consult a urologist for stone re-
moval when the likelihood of spontaneous passage is low or when complications
occur. Urinary tract infection with obstruction is the most urgent indication for
hospitalization and urologic consultation.
CLINICAL BOTTOM LINE
Preventive
Treatment What is the role of fluid intake
and diet in the preventive
episodic condition that is not usually
life-threatening. Despite ample epi-
treatment of patients with demiologic data linking diet and
nephrolithiasis? stones, only 1 RCT with positive re-
Advise patients at high risk for re- sults has been published. Few data
current stone disease to drink at are available regarding the willing-
least 2 to 2.5 L/d (68 to 85 oz) to ness and ability of stone-forming pa-
maintain urine volume of at least tients to adhere to a diet. Epidemio-
2 L. Emphasize higher intake to logic evidence demonstrates that
achieve the same urine output in men and women with greater calci-
people who are physically active um intake have fewer stones (23,
(for example, athletes), work in hot 24). This effect is most likely due to
climates (for example, lifeguards), the ability of dietary calcium to bind
have diseases associated with stone oxalate in the intestine and prevent
formation (for example, distal its absorption.
RTA, medullary sponge kidney, These observational data were supported
polycystic kidney disease), or have by 1 RCT. Italian men (n = 120) with hyper-
increased bowel fluid losses (for ex- calciuria and recurrent calcium oxalate
ample, from ileostomy or other stones were randomly assigned to 1 of 2
bowel disorders). Increased fluid regimens. One regimen restricted calcium
intake leads to urine dilution and a intake to 400 mg/d, and the other recom-
decrease in urine supersaturation of mended a “normal” calcium intake of 1200
23. Curhan GC, Willett
mg/d and restricted animal protein (52 g)
WC, Rimm EB, et al. poorly soluble salts, such as calcium
A prospective study and salt intake (50 mmol) (Table 1). In both
of dietary calcium oxalate, calcium phosphate, and groups, participants were counseled to re-
and other nutrients
and the risk of cystine. Urine volume may be less strict oxalate intake. At the end of 5 years,
symptomatic kidney important in uric acid stone– the group on the high-calcium, low-salt,
stones. N Engl J
Med. 1993;328:833- forming patients who successfully low–animal-protein diet had a 50% lower
8. [PMID: 8441427]
24. Curhan GC. Dietary alkalinize the urine. Increasing flu- rate of stone recurrence when compared
calcium, dietary pro- id intake may be especially difficult with the group on the low-calcium diet.
tein, and kidney
stone formation. for men with benign prostatic hy- The effect was attributed to increased cal-
Miner Electrolyte
pertrophy or for other persons with cium ingestion leading to reduced urinary
Metab. 1997;23:261-
oxalate excretion while sodium restriction
4. [PMID: 9387129] bladder disorders. These patients limited urinary calcium excretion. Protein
25. Borghi L, Schianchi
T, Meschi T, et al. may benefit from dietary alteration restriction may have also played a part by
Comparison of two
diets for the preven- and drug therapy. increasing citrate excretion and contribut-
tion of recurrent ing to the reduction of calcium excretion
stones in idiopathic
hypercalciuria. N
Diet is an attractive therapy to many (both of which may occur with less net
Engl J Med. patients with stones who may be re- acid excretion, suggested by the modest
2002;346:77-84.
[PMID: 11784873] luctant to take medications for an decrease in urine sulfate excretion) (9).
© 2009 American College of Physicians ITC2-8 In the Clinic Annals of Internal Medicine 4 August 2009
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 9
Although bone mineral density was several RCTs have demonstrated that
not measured, one would anticipate thiazides prevent recurrent calcium
that the group on the higher calcium stones. At 3 years, stones recurred in
intake would have had less deminer- 50% to 60% of patients receiving
alization than the other group. This placebo and 15% to 30% of patients
possibility is another reason not to receiving thiazide. Studies with less
restrict calcium in patients with hy- than 2 years of treatment did not
percalciuria, who have reductions in show benefit (26, 27). Thiazides in-
bone mineral density and more fre- clude chlorthalidone, indapamide,
quent bone fractures (25). and hydrochlorothiazide. The first 2
are usually taken once a day, whereas
Patients with uric acid stones should hydrochlorothiazide is best taken
limit animal protein intake, which twice a day. Thiazides reduce urinary
reduces the amount of alkali needed calcium by stimulating renal calcium
to increase urine pH, but diet alone reabsorption and may stimulate bone
has not been shown to prevent uric to incorporate calcium. Because hy-
acid stones. People with cystine percalciuria is linked to decreases in
stones should limit animal protein bone mineral density (BMD), it is
and salt intake to increase urine pH useful that thiazides are also associat-
and reduce cystine excretion. ed with increases in BMD (28).
Because thiazides can cause hypo-
What drug therapy should kalemia, which lowers citrate excre-
clinicians consider to prevent tion, most patients receiving thiazides
recurrent nephrolithiasis, and how should be supplemented twice a day
does it differ in patients with with potassium citrate or given potas-
different types of stone disease? sium-sparing drugs, such as amiloride
Table 2 lists drug therapy for stone or spironolactone. Avoid triamterene,
prevention. The effectiveness of this because it is poorly soluble.
or other diets in patients with other
risk factors for stones, or other types Citrate is an inhibitor of the crystal-
of stones, has not been tested. Thi- lization of calcium oxalate and calci-
azides lower urinary calcium excretion um phosphate. Use citrate supple-
in patients with hypercalciuria, and mentation for secondary prevention
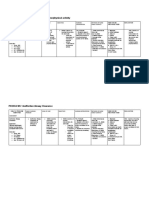
Table 1. Composition of the Normal-Calcium, Low-Protein, Low-Salt Diet*
Daily Intake Value
Total calories, kcal 2540
Total protein, g 93†
26. Pearle MS,
From meat or fish, g 21 Roehrborn CG, Pak
CY. Meta-analysis of
From milk and derivatives, g 31 randomized trials for
From bread, pasta, and vegetables, g 41 medical prevention
of calcium oxalate
Lipids, g 93 (837 kcal, or approximately 33% of total calories) nephrolithiasis. J En-
dourol. 1999;13:679-
Carbohydrates, g 333 (1332 kcal, or approximately 52% of total calories) 85. [PMID: 10608521]
Fiber, g 40 27. Ettinger B, Citron JT,
Livermore B, et al.
Sodium chloride, mmol 50 Chlorthalidone re-
duces calcium ox-
Potassium, mmol 120 alate calculous re-
Calcium, mmol 30 currence but
magnesium hydrox-
Phosphorus, mmol 48.8 ide does not. J Urol.
Magnesium, mmol 14.5 1988;139:679-84.
[PMID: 3280829]
Oxalate, mmol Approximately 2.2 28. Adams JS, Song CF,
Kantorovich V. Rapid
Water in foods, mL 1550 recovery of bone
mass in hypercalci-
* The data were obtained from the composition tables issued in 1989 by the Italian National Institute for Nutrition. The uric, osteoporotic
values are based on direct chemical analyses of the foods available in Italian markets. Reprinted with permission from men treated with
reference 24. Copyright 2002 Massachusetts Medical Society. All rights reserved. hydrochlorothiazide.
Ann Intern Med.
† 1999;130:658-60.
372 kcal, or approximately 15% of total calories.
[PMID: 10215562]
4 August 2009 Annals of Internal Medicine In the Clinic ITC2-9 © 2009 American College of Physicians
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 10
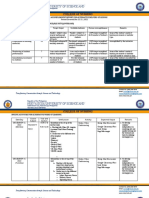
Table 2. Drug Treatment of Stone Prevention
Agent Mechanism of Action Dosage Benefits Side Effects and Notes
Hydrochlorothiazide Stimulates renal 25 to 50 mg qd Prevents stones, Most patients require potassium citrate supplemen-
calcium reabsorption; to bid lowers blood tation in conjunction with thiazides, either for hypo-
may inhibit bone pressure, increases kalemia or decreased citrate excretion. The latter
resorption bone density loccurs with potassium depletion even with normal
serum potassium concentration. Hypokalemia is also
associated with hypocitraturia. Hypotension is occa-
sionally a problem in young, normotensive persons. For
secondary prevention of kidney stones, chlorthalidone
may be slightly more potent in reducing calciuria but
may also cause more potassium loss. Indapamide is
also effective. Concomitant sodium restriction maxi-
mizes effect on calciuria. Avoid poorly soluble tri-
amterene as potassium-sparing combination. Amiloride
is preferable as a potassium-sparing agent. Sodium
restriction also minimizes potassium losses.
Potassium citrate Citrate forms soluble 20 to 30 mEq bid to Increases urinary GI intolerance, especially in elderly patients or patients
complexes with tid. Once-daily citrate excretion and with GERD (heartburn, nausea). Potential for hyper-
calcium; inhibits crystal dosing may be prevents calcium kalemia in patients with renal insufficiency or taking
growth and aggregation. effective for some stone recurrence. ACE inhibitors. For secondary prevention of kidney
For uric acid and cystine patients if citrate Increased urine pH stones. Comes in longer-acting tablets or dissolvable
stones, citrate increases excretion or urine dissolves uric acid crystal forms. Sodium citrate preparations may have
urine pH after pH increases crystals and better GI tolerance for some but are not clearly
metabolism to adequately. Dosing solubilizes cystine. effective in preventing stone recurrence.
bicarbonate by liver tid may be appro- At urine pH values
priate for dissolution >7.0, solubility of
of uric acid or cystine in urine in-
cystine stones. creases dramatically.
Allopurinol Xanthine oxidase 300 mg qd, reduce Prevents stone Rare allergy, eosinophilia, interstitial nephritis, the
inhibitor reduces with decreased GFR recurrence in Stevens–Johnson syndrome. For secondary prevention
urinary uric acid patients with of kidney stones. For uric acid stones, urinary
excretion hyperuricosuria and alkalinization with citrate supplementation is
normocalciuria. usually more important than reducing uricosuria.
Prevents gout.
Adjunctive to
potassium citrate
for uric acid stones.
Organic marine Seaweed-derived 9 tablets per day Well-tolerated Only anecdotal reports exist of efficacy for reducing
hydrocolloid hydrocolloid binds nutraceutical agent urinary oxalate excretion.* Decreased urinary oxalate
(Ox-Absorb) oxalate in intestinal for treatment of in patients with bowel disorders. No trials
lumen and prevents hyperoxaluria. demonstrating decreased stone recurrence. Both
absorption Useful for enteric or calcium citrate and cholestyramine may have
dietary hyperoxaluria. some effect to reduce intestinal oxalate absorption.
Sodium cellulose Ion-exchange resin 10 g/d in divided Reduction of Causes negative calcium balance and decreased
phosphate which binds dietary doses hypercalciuria bone mineral density, similar to dietary calcium
calcium in intestinal restriction. Can reduce urinary magnesium excretion
lumen and reduces and increase urinary oxalate. No randomized trials
urinary calcium excretion have been performed with stone formation as an
outcome, and questions about long-term safety be-
cause of risk for osteoporosis have led to very infre-
quent use of this preparation.†
Orthophosphate Reduces serum 4 tablets bid. Each Neutral potassium Associated acid and sodium loads limit efficacy in
1,25-dihydroxyvitamin D tablet contains phosphate may reducing calciuria and protecting bone density.
concentration and phosphate, 155 mg, directly inhibit bone Rapid-release forms are associated with abdominal
intestinal calcium and potassium, resorption while cramping and diarrhea. Slow-release potassium
absorption; increases 8 mEq. reducing calcium phosphate may be better tolerated. A randomized,
urinary excretion of absorption and controlled trial of phosphate acid did not prevent
pyrophosphate, an urinary excretion stones‡. A slow-release preparation of neutral
inhibitor of calcium potassium phosphate was safe and effective in
oxalate crystal formation improving urinary chemistries and preventing bone re-
sorption in a short randomized trial, although efficacy
in preventing stones was not studied. It may overcome
the disadvantages of acid and sodium phosphate
preparations, but is not yet commercially available.§
(continued on next page)
© 2009 American College of Physicians ITC2-10 In the Clinic Annals of Internal Medicine 4 August 2009
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 11
Table 2. Drug Treatment of Stone Prevention (continued )
Agent Mechanism of Action Dosage Benefits Side Effects and Notes
Magnesium Magnesium inhibits Patients with bowel Diarrhea. Efficacy of magnesium supplementation in
supplementation calcium oxalate crystal disease often have randomized, controlled trials is lacking. It should
formation and growth decreased urinary probably be reserved for patients with low urinary
in vitro. Hypomagne- magnesium magnesium excretion.||
semia may reduce excretion, which
urinary citrate excretion. might contribute
to stone formation
Acetohydroxamic Inhibits activity of 250 mg bid for 3 to Inhibition of urease Headache is a frequent side effect to limit long-term
acid urease, the bacterial 4 weeks; if tolerated, decreases urinary use. 20% to 30% of patients are unable to tolerate
enzyme responsible for increase dose to alkalinization and use of the drug. Other side effects include mild
causing struvite stones 250 mg tid precipitation of hemolytic anemia, GI upset, tremulousness, dysgeusia,
struvite anxiety. Surgical removal of all struvite stone frag-
ments is the most effective therapy and preferable to
this drug. Acetohydroxamic acid does reduce stone
growth but not necessarily stone events. Adequate uri-
nary levels of the drug are not achieved if serum crea-
tinine is >176.8 mmol/L (2 mg/dL).¶
Tiopronin Thiol drug reduces the 500 to 1000 mg/d, Solubilizes cystine Rash, proteinuria, GI intolerance, pruritus, intrahepatic
(α-mercapto disulfhydryl bridge of occasionally up to cholestasis, wrinkling and friability of the skin,
propionylglycine) cystine to form the 3000 mg/d hypogeusia, vitamin B6 deficiency. Limited sources
more soluble suggest a somewhat better side effect profile than
drug–cysteine complex D-penicillamine. Administer vitamin B6, 50 mg/d.
Check LFTs and CBC every mo when initiating therapy,
then every 3 mo.**
D-penicillamine Thiol drug reduces the 1000 to 2000 mg/d Solubilizes cystine Bone marrow depression with leukopenia,
disulfhydryl bridge of thrombocytopenia. Agranulocytosis, aplastic anemia,
cystine to form the pancytopenia, and sideroblastic anemia can be fatal.
more soluble Proteinuria, dysgeusia, fever, rash, vitamin B6
drug–cysteine complex deficiency, aphthous stomatitis. Give vitamin B6,
50 mg/d. Check LFTs and CBC every mo when initiating
therapy, then every 3 mo.
ACE = angiotensin-converting enzyme; bid = twice daily; BID = twice daily; CBC = complete blood count; GERD = gastroesophageal reflux disease; GFR =
glomerular filtration rate; GI = gastrointestinal; LFT = liver function tests; qd = once daily; tid = three times daily.
* Lindsjö M, Fellström B, Ljunghall S, et al. Treatment of enteric hyperoxaluria with calcium-containing organic marine hydrocolloid. Lancet. 1989;2:701-
4. [PMID: 2570957]
†
Breslau NA. Pathogenesis and management of hypercalciuric nephrolithiasis. Miner Electrolyte Metab. 1994;20:328-39. [PMID: 7783695]
Pak CY. A cautious use of sodium cellulose phosphate in the management of calcium nephrolithiasis. Invest Urol. 1981;19:187-90. [PMID: 7298289]
‡
Ettinger B. Recurrent nephrolithiasis: natural history and effect of phosphate therapy. A double-blind controlled study. Am J Med. 1976;61:200-6.
[PMID: 782240]
§
Breslau NA, Heller HJ, Reza-Albarrán AA, et al. Physiological effects of slow release potassium phosphate for absorptive hypercalciuria: a randomized
double-blind trial. J Urol. 1998;160:664-8. [PMID: 9720517]
||
Reungjui S, Prasongwatana V, Premgamone A, et al. Magnesium status of patients with renal stones and its effect on urinary citrate excretion. BJU Int.
2002;90:635-9. [PMID: 12410738]
¶
Wang LP, Wong HY, Griffith DP. Treatment options in struvite stones. Urol Clin North Am. 1997;24:149-62. [PMID: 9048858]
** Pak CY, Fuller C, Sakhaee K, et al. Management of cystine nephrolithiasis with alpha-mercaptopropionylglycine. J Urol. 1986;136:1003-8. [PMID:
3534301]
of calcium stones in patients with re- patient per year in the treated group
duced urinary citrate. Low urine compared with no change in the
citrate occurs with chronic metabolic placebo group (29). Potassium citrate
acidosis, which can be caused by supplementation might also be
bowel disease, RTA, and high pro- useful in “unselected” calcium stone–
tein intake but is often idiopathic. In forming patients regardless of uri-
29. Barcelo P, Wuhl O,
an RCT of potassium citrate in pa- nary citrate excretion. Citrate Servitge E, et al. Ran-
tients with calcium stones and low supplementation is associated with domized double-
blind study of potas-
urinary citrate, treatment with potas- an increase in urine pH. In calcium sium citrate in
idiopathic hypocitra-
sium citrate, 30 to 60 mEq/d in stone disease, this increase in urine turic calcium
divided doses, led to reduction of pH might lead to an increase in nephrolithiasis. J
Urol. 1993;150:1761-
stone formation from 1.2 to 0.1 per urine supersaturation of calcium 4. [PMID: 8230497]
4 August 2009 Annals of Internal Medicine In the Clinic ITC2-11 © 2009 American College of Physicians
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 12
phosphate with subsequent calcium Use potassium citrate to increase
phosphate stones (30). Adequate flu- urine pH and dissolve uric acid. Use
id intake is, therefore, more impor- allopurinol only in patients with
tant in this setting, and thiazide use hyperuricosuria in whom alkaliniza-
30. Parks JH, Coe FL, to lower urinary calcium excretion
Evan AP, et al. Urine
tion is difficult, poorly tolerated, or
pH in renal calcium may be indicated if urine pH is in- not completely effective.
stone formers who
do and do not in- creasing and calcium phosphate
crease stone phos- stone formation occurs. Orange juice Most patients with uric acid stones
phate content with
time. Nephrol Dial and lemonade increase urine citrate have a low urine pH as the major risk
Transplant.
excretion (31, 32), and drinking factor, rather than hyperuricosuria.
2009;24:130-6.
[PMID: 18662977] lemonade has been associated with
31. Seltzer MA, Low RK,
fewer stone recurrences in observa- Even intermittent urinary alkalin-
McDonald M, et al.
Dietary manipula-
tional studies (33). ization, once a day or every other
tion with lemonade
to treat hypocitra-
day, may suffice to prevent recur-
turic calcium In 1 placebo-controlled trial, at 3 years rent uric acid stones (37). In the
nephrolithiasis. J
Urol. 1996;156:907-9. stones formed in 63.6% of participants re- presence of low pH, reducing uri-
[PMID: 8709360] ceiving placebo and 12.9% of participants nary uric acid excretion with allop-
32. Odvina CV. Compar-
ative value of orange receiving a combination of potassium and urinol is relatively ineffective,
juice versus lemon- magnesium citrate (34). The drug was ef- whereas if pH is increased, uric acid
ade in reducing
stone-forming risk. fective regardless of whether urine citrate stones will not form even in patients
Clin J Am Soc was low.
Nephrol. with substantial hyperuricosuria
2006;1:1269-74.
[PMID: 17699358] The potassium–magnesium citrate (38). No randomized trials have
33. Kang DE, Sur RL,
preparation may be better tolerated been done on urinary alkalinization
Haleblian GE, et al.
Long-term lemon- than the potassium salt alone but is for uric acid stone prevention,
ade based dietary
manipulation in pa- currently not available. Magnesium because of the perceived efficacy of
tients with hypoci-
supplementation has not been shown potassium citrate therapy.
traturic nephrolithia-
sis. J Urol. to be effective in patients without
2007;177:1358-62; The low urine pH seen in patients
discussion 1362; bowel disease (35), so reserve it for
with uric acid stones may be due to
quiz 1591. patients with inflammatory bowel
[PMID: 17382731] an abnormality in renal ammonia-
34. Ettinger B, Pak CY, disease, diarrhea, or ileostomy.
Citron JT, et al. genesis associated with increased
Potassium-magne-
sium citrate is an ef- Calcium phosphate stones suggest body mass index and insulin resist-
fective prophylaxis
hyperparathyroidism or RTA. Treat ance (39).
against recurrent
calcium oxalate hyperparathyroidism with surgery,
nephrolithiasis. J
and treat RTA with potassium cit- For cystine stones, prevention starts
Urol. 1997;158:2069-
73. [PMID: 9366314] rate and thiazides if hypercalciuria with high fluid intake to maintain
35. Massey L. Magne-
sium therapy for is present. urinary cystine concentrations less
nephrolithiasis. than 250 mg/L. Dietary restriction
Magnes Res.
2005;18:123-6. Uric acid diminishes the solubility of of protein and salt limits cystine
[PMID: 16100850]
calcium oxalate, so use allopurinol to excretion (40). Citrate supplemen-
36. Ettinger B, Tang A,
Citron JT, et al. Ran- prevent calcium oxalate stones in tation to increase urine pH to 7.0
domized trial of al-
lopurinol in the pre- patients with hyperuricosuria when or more helps solubilize cystine, but
vention of calcium hypercalciuria or hypocitraturia are a urinary pH of 7.5 or higher may
oxalate calculi. N
Engl J Med. absent. In 1 randomized, double- be necessary to see clinical benefit.
1986;315:1386-9.
[PMID: 3534570] blind trial of allopurinol, 100 mg Thiol-binding drugs tiopronin and
37. Rodman JS. Inter- taken 3 times daily, in patients with D-penicillamine reduce urinary
mittent versus con-
tinuous alkaline normocalciuria the mean rate of cystine to the more soluble cys-
therapy for uric acid teine-drug complex (41).
stones and ureteral
stone events was 0.26 per patient per
stones of uncertain year in the placebo group and 0.12 in
composition. Urolo-
the allopurinol group (36). Restric- For struvite stones, successful treat-
gy. 2002;60:378-82.
[PMID: 12350465] tion of dietary animal protein intake ment requires stone removal, because
38. Maalouf NM,
Cameron MA, Moe will reduce uric acid excretion but, infected stones cannot be sterilized
OW, et al. Novel in-
unlike allopurinol, has not been test- with antibiotics. The AUA
sights into the
pathogenesis of uric ed in RCTs. Nephrolithiasis Clinical Guidelines
acid nephrolithiasis.
Curr Opin Nephrol
Panel has recommended that struvite
Hypertens. For uric acid stones, urinary alkalin- stones are best treated with percuta-
2004;13:181-9.
[PMID: 15202612] ization prevents stone recurrences. neous nephrolithotomy (21). Stone
© 2009 American College of Physicians ITC2-12 In the Clinic Annals of Internal Medicine 4 August 2009
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 13
removal is often followed by long initially and then less frequently
courses (4 to 6 months) of suppres- with serial ultrasonography, or in
sive low-dose antibiotics, such as the case of calcium stones, with
39. Maalouf NM,
nitrofurantoin or sulfamethoxazole– plain abdominal radiography. Com- Cameron MA, Moe
trimethoprim. If residual stone puted tomography is more sensi- OW, et al. Low urine
pH: a novel feature
material is left in place, use acetohy- tive, but the cumulative dose of of the metabolic
syndrome. Clin J Am
droxamic acid to inhibit bacterial radiation may not be acceptable. Soc Nephrol.
urease activity and decrease rates of The potential value of screening is 2007;2:883-8.
[PMID: 17702734]
stone growth. In 1 double-blind, that it may aid decisions about 40. Goldfarb DS, Coe FL,
Asplin JR. Urinary
placebo-controlled study, the drug intensifying preventive therapy, cystine excretion
was evaluated in 94 patients with motivate patients to adhere to rec- and capacity in pa-
tients with cystin-
chronic urinary tract infection. Stone ommendations, and allow elective uria. Kidney Int.
growth occurred in 17% of the ace- scheduling of urologic interventions 2006;69:1041-7.
[PMID: 16501494]
tohydroxamic acid group and in 46% instead of during or after episodes of 41. Mattoo A, Goldfarb
DS. Cystinuria. Semin
of the placebo group. “Intolerable” renal colic, but no data exist on the Nephrol.
side effects were experienced by effectiveness of screening. 2008;28:181-91.
[PMID: 18359399]
22.2% of patients in the acetohy- 42. Griffith DP, Gleeson
In 1 study of 107 patients with asympto- MJ, Lee H, et al.
droxamic acid group (42). Evaluate Randomized, dou-
matic stones with a mean follow-up of
patients with struvite stones for un- 31.6 months, 68.2% remained asympto-
ble-blind trial of
Lithostat (acetohy-
derlying metabolic abnormalities, matic. A symptomatic event developed in droxamic acid) in
the palliative treat-
such as low urine volume, hypercal- 31.8%. Of these, almost one half had spon- ment of infection-in-
ciuria, and hypocitraturia, which taneous passage, whereas the rest re- duced urinary cal-
culi. Eur Urol.
occur in as many as 40% of patients, quired urologic intervention. Cumulative 1991;20:243-7.
[PMID: 1726639]
and treat these abnormalities. 5-year probability of a symptomatic event 43. Asplin JR, Bauer KA,
was 48.5% (45). Kinder J, et al. Bone
What are the complications of mineral density and
urine calcium excre-
nephrolithiasis and how should In a retrospective study of 76 patients with tion among subjects
clinicians treat them? asymptomatic stones, the cumulative prob- with and without
nephrolithiasis. Kid-
ability of an episode of renal colic was 39%
Patients with calcium stones and hy- ney Int. 2003;63:662-
at 5 years and 51% at 10 years. Fourteen pa- 9. [PMID: 12631132]
percalciuria have been shown to have tients (18.4%) required ESWL or other uro- 44. Rule AD, Bergstralh
EJ, Melton LJ 3rd, et
decreased bone density (43) and a logic interventions (46). al. Kidney stones
higher rate of bone fracture (25). and the risk for
chronic kidney dis-
Thiazides put patients with hypercal- One study suggested that a policy of ob- ease. Clin J Am Soc
ciuria into positive calcium balance servation was associated with a greater Nephrol. 2009;4:804-
11. [PMID: 19339425]
and increase bone mineral density risk for requiring more invasive procedures. 45. Glowacki LS,
(BMD) (28). Stones are associated In 1 RCT, 228 patients with small (<15 mm Beecroft ML, Cook
RJ, et al. The natural
with chronic kidney disease, although total diameter) asymptomatic calyceal history of asympto-
stones were randomly assigned to ESWL or matic urolithiasis. J
the nature of this relationship is not observation. With a mean follow-up of 2.2
Urol. 1992;147:319-
21. [PMID: 1732583]
clearly understood (44). years, 28% of the patients in the ESWL 46. Cupisti A, Vagelli G,
Morelli E, et al. Out-
group were stone-free, compared with come of asympto-
How should clinicians follow 17% in the observation group. Ten patients matic caliceal calci-
patients with nephrolithiasis? in the observation group required invasive
um nephrolithiasis. J
Nephrol. 1996;9:144-
Consider screening patients with procedures, compared with none in the 6.
multiple episodes of symptomatic ESWL group. Prophylactic ESWL, therefore, 47. Keeley FX Jr, Tilling
K, Elves A, et al. Pre-
stone disease every 6 to 12 months had a slight advantage (47). liminary results of a
randomized con-
trolled trial of pro-
phylactic shock
wave lithotripsy for
Preventive Treatment... Prevent recurrent stones with a stepped approach. In- small asymptomatic
renal calyceal stones.
creased fluid intake is always appropriate because it is effective, safe, and inex- BJU Int. 2001;87:1-8.
pensive. Dietary changes may be added if recurrence continues. Pharmacologic [PMID: 11121982]
therapy is appropriate for patients unable to adhere to dietary changes or if 48. Goldfarb DS. Recon-
sideration of the
dietary therapy is ineffective. If recurrence continues, consider screening for 1988 NIH Consensus
asymptomatic stones with ultrasonography or plain radiography for calcium Statement on Pre-
vention and Treat-
stones, recognizing that little evidence supports the value of screening. ment of Kidney
Stones: Are the Rec-
ommendations Out
of Date? Rev Urol.
CLINICAL BOTTOM LINE 2002;4:53-60.
[PMID: 16985656]
4 August 2009 Annals of Internal Medicine In the Clinic ITC2-13 © 2009 American College of Physicians
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 14
Practice
Improvement What do professional
organizations recommend
How should clinicians educate
patients with nephrolithiasis?
regarding the care of patients Patients can be referred to the Web
with nephrolithiasis? resources listed in the Toolkit. A
The National Institutes of Health useful book about preventing
49. Segura JW, Pre-
minger GM, Assimos last published a consensus docu- stones, written for lay people and
DG, et al. ment in 1980 (14). The recommen- co-authored by a nephrologist,
Nephrolithiasis Clini-
cal Guidelines Panel dations made at that time have not a urologist and a dietician, is
summary report on
the management of
evolved substantially (48). Surgical available (51).
staghorn calculi. The therapy has improved dramatically,
American Urological
Association radiologic imaging is vastly superi-
Nephrolithiasis Clini-
cal Guidelines Panel.
or, but medical therapy has not
J Urol. advanced very much, with the ex-
1994;151:1648-51.
[PMID: 8189589]
ception of not restricting calcium
50. Preminger GM, intake in calcium stone–forming
Tiselius HG, Assimos
DG, et al; American patients. The AUA guidelines ad-
Urological Associa-
tion Education and
dress surgical management rather
Research, Inc. 2007 than preventive therapy (20, 49). In
Guideline for the
management of 2007, the American Urological As-
ureteral calculi. Eur sociation and the European Associ-
Urol. 2007;52:1610-
31. [PMID: 18074433] ation of Urology cooperated to
51. Rodman JS, Sosa RE,
Seidman C, et al. No
create joint recommendations for
More Kidney Stones. managing patients with suspected
Hoboken, NJ: J Wi-
ley; 2007. kidney stones (21, 50).
in the clinic
in the clinic PIER Modules
www.pier.acponline.org
Tool Kit
Access the PIER module on Nephrolithiasis.
Patient Information
www.urologyhealth.org/adult/index.cfm?cat=12&topic=105
American Urological Association: Management of Ureteral Stones
www.urologyhealth.org/adult/index.cfm?cat=12&topic=102
Nephrolithiasis American Urological Association: Medical Management of Stone Disease
www.urologyhealth.org/adult/index.cfm?cat=12&topic=132
American Urological Association: Surgical Management of Stones
kidney.niddk.nih.gov/kudiseases/pubs/stonesadults/index.htm
National Institute of Diabetes and Digestive and Kidney Diseases:
Kidney Stones in Adults
kidney.niddk.nih.gov/kudiseases/pubs/stones_ez/index.htm
National Institute of Diabetes and Digestive and Kidney Diseases:
What I Need to Know About Kidney Stones
kidney.niddk.nih.gov/spanish/pubs/stones_ez/index.htm
National Institute of Diabetes and Digestive and Kidney Diseases:
What I Need to Know About Kidney Stones (Spanish)
www.kidney.org/Atoz/atozItem.cfm?id=84
National Kidney Foundation
Clinical Guidelines
www.auanet.org/content/guidelines-and-quality-care/clinical-guidelines.cfm?sub=uc
Access the American Urological Association guidelines on ureteral calculi.
www.uroweb.org/fileadmin/tx_eauguidelines/2008/Full/17%20Urolithiasis.pdf
Access the European Association of Urology guidelines on urolithiasis.
© 2009 American College of Physicians ITC2-14 In the Clinic Annals of Internal Medicine 4 August 2009
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 15
WHAT YOU SHOULD In the Clinic
Annals of Internal Medicine
KNOW ABOUT KIDNEY
STONES
What is a kidney stone?
• A kidney stone is a solid piece of material that forms
in a kidney from substances in the urine.
• A stone may stay in the kidney or break loose and
move down the urinary tract. A small stone may pass
all the way out of the body without too much pain.
• A larger stone may get stuck. It can block the flow of
urine and cause great pain.
What can my doctor do about a
large stone?
• If you have a stone that does not pass by itself, your
doctor may need to remove it. Your doctor may
choose one of the following ways to do this.
Shock Waves
• A machine sends shock waves to the kidney stone. This
breaks the stone into small pieces that pass out of your
body with your urine. This method is called extracorpo-
real shock wave lithotripsy (ESWL). Lithotripsy is a Greek
word that means stone crushing.
• With one type of shock machine, you sit in a tub of
water. With the other type, you lie on a table. A tech-
nician directs the sound waves to the stone.
Tunnel Surgery
Patient Information
• The doctor makes a small cut on your back. A special
instrument passes through a narrow tunnel to the Points to Remember
stone and removes it. This method is called percuta-
neous nephrolithotomy. • Most stones pass out of the body without a doctor’s
help.
Ureteroscope • See your doctor if you have severe pain in your back
or side that will not go away.
• A ureteroscope looks like a long wire. The doctor puts
it into the patient’s urethra through the bladder and • See your doctor if you have blood in your urine—the
up the ureter, and directs it to the stone. This is done urine will look pink.
using a camera that lets the doctor see the stone. A • In the future, after the stone is gone, drink lots of wa-
tiny cage catches the stone and pulls it out, or the ter to prevent more kidney stones from forming.
doctor may be able to destroy it with a laser. • Talk with your doctor about other ways to keep from
• Ask your doctor which method is right for you. getting more stones.
For More Information
kidney.niddk.nih.gov/kudiseases/pubs/stones_ez/index.htm
National Institute of Diabetes and Digestive and Kidney Diseases:
What I Need to Know About Kidney Stones
kidney.niddk.nih.gov/spanish/pubs/stones_ez/index.htm
National Institute of Diabetes and Digestive and Kidney Diseases:
What I Need to Know About Kidney Stones (Spanish)
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
acp-clinic0908 7/20/09 3:28 PM Page 16
CME Questions
1. In a patient with hypercalciuric several years, she has had dry eyes and formed in the past 6 months; however,
nephrolithiasis, which of the following dry mouth. She also describes symptoms hypokalemia has developed (serum
is associated with increased risk for of Raynaud’s phenomenon. Crohn dis- potassium level, 2.9 mmol/L).
stone formation? ease was diagnosed 10 years ago; the Taking the hypokalemia into account,
A. Low-sodium diet patient is currently asymptomatic and what therapy should the patient receive
passes 1 formed stool daily. She takes for hypercalciuric stone disease?
B. Low-calcium diet
no medications. There is no family histo-
C. Low-oxalate diet A. High-potassium diet plus
ry of renal stone disease.
D. Low-protein diet hydrochlorothiazide
E. Low-purine diet On examination, the patient is alert and
B. Acetazolamide plus
healthy. Blood pressure is 115/74 mm
hydrochlorothiazide
2. A 39-year-old male carpenter presents Hg, pulse rate is 72/min, and tempera-
C. Magnesium oxide plus
to the emergency department with a ture is 37°C (98.6°F). The skin is clear,
and the joints are normal. The lungs are hydrochlorothiazide
4-hour history of gradually worsening
right flank and right upper quadrant clear. Cardiac examination shows regu- D. Amiloride plus
pain radiating to the right lower quad- lar sinus rhythm and no murmur. The hydrochlorothiazide
rant and into the right testicle. He vom- liver and spleen are not palpable, and
5. A 64-year-old woman comes for a fol-
its once shortly after arrival. He does the abdomen is not tender.
low-up visit after an episode of kidney
not have fever or chills but has mild Plain abdominal radiography shows stones 2 weeks ago. During the episode,
dysuria. multiple calcifications overlying both she went to the emergency department
On examination, the patient is restless renal shadows. and was treated with nonsteroidal anti-
because of pain. Blood pressure is Laboratory study results are as follows: inflammatory drugs and fluids. Spiral
145/89 mm Hg, pulse rate is 92/min, hemoglobin, 13.2 g/dL; hematocrit, abdominal CT performed at that time
and temperature is 37°C (98.6°F). Ab- 39%; leukocyte count, 7.4 × 109 revealed a 3-mm nonobstructing calcu-
dominal examination reveals mild right cells/µL; blood urea nitrogen, 6.4 lus in the midleft ureter. She also has
costovertebral angle tenderness, but no mmol/L (18 mg/dL); serum creatinine, osteoporosis.
abdominal guarding. Genitalia are nor- 79.56 µmol/L (0.9 mg/dL); serum sodi- Laboratory study results are as follows:
mal. The serum creatinine concentration um, 138 mmol/L; serum potassium, blood urea nitrogen, 7.5 mmol/L
is 79.56 µmol/L (0.9 mg/dL). Urinalysis 2.8 mmol/L; serum chloride, (21 mg/dL); uric acid, 0.3 mmol/L;
shows a specific gravity of 1.025, 3+ 109 mmol/L; serum bicarbonate, creatinine, 141.47 µmol/L (1.6 mg/dL);
hematuria, and no proteinuria. Urine 19 mmol/L; serum calcium, 2.3 mmol/L sodium, 137 mmol/L; potassium,
microscopy reveals more than 50 ery- (9.1 mg/dL); serum phosphorus, 3.2 3.8 mmol/L; chloride, 105 mmol/L;
throcytes/hpf, 3 to 5 leukocytes/hpf, mg/dL; urinalysis: pH, 6.0, specific gravi- bicarbonate, 24 mmol/L; albumin,
and occasional calcium oxalate crystals. ty, 1.020, trace hematuria, no protein- 4.1 g/L; calcium, 2.87 mmol/L
You suspect that a uria; arterial blood: pH, 7.29. (11.5 mg/dL); phosphorus, 0.39 mmol/L
renal stone is causing the colicky pain
What is the most likely cause of this pa- (1.2 mg/dL); urinalysis: pH, 5.5,
and hematuria.
tient’s renal stone disease? 1+ blood.
What radiologic procedure will best
A. Idiopathic hypercalciuria Which of the following is the most
confirm the diagnosis?
B. Primary hyperthyroidism appropriate management for this pa-
A. Plain radiography of the abdomen C. Distal renal tubular acidosis tient’s kidney stones?
B. Intravenous pyelography D. Enteric hyperoxaluria A. Decrease dietary calcium to
C. Renal ultrasonography <1 g/d
D. Noncontrast spiral computed 4. A 40-year-old man has recurrent B. Refer for parathyroidectomy
tomography nephrolithiasis due to idiopathic hyper- C. Refer for stone removal
calciuria. He has had more than 40 cal-
3. A 28-year-old woman presents for eval- D. Initiate potassium citrate therapy
cium oxalate stones in the past 5 years.
uation of recurrent kidney stones that E. Observe
He starts taking hydrochlorothiazide
she says “contain calcium.” She esti- therapy and a low-sodium diet. During
mates that she has passed four stones treatment, his 24-hour urinary calcium
during the past 4 years. She currently concentration decreases from 385 mg/d
has no symptoms of renal colic. For to 180 mg/d. No new stones have
Questions are largely from the ACP’s Medical Knowledge Self-Assessment Program (MKSAP). Go to www.annals.org/intheclinic/
to obtain up to 1.5 CME credits, to view explanations for correct answers, or to purchase the complete MKSAP program.
© 2009 American College of Physicians ITC2-16 In the Clinic Annals of Internal Medicine 4 August 2009
Downloaded From: http://annals.org/ by a McGill University User on 10/04/2016
S-ar putea să vă placă și
- Situational Analysis of Public Health Nursing Personnel in IndiaDocument60 paginiSituational Analysis of Public Health Nursing Personnel in IndiaTamilNurse.com100% (1)
- MB451X PSDocument2 paginiMB451X PSMalik AzizÎncă nu există evaluări
- COPD Secondaryto PTBDocument142 paginiCOPD Secondaryto PTBallexiscampaner100% (2)
- 6-Health Problems Common in PreschoolerDocument36 pagini6-Health Problems Common in PreschoolerPam Lala100% (2)
- Bronchitis Vs EmphysemaDocument1 paginăBronchitis Vs Emphysemaal-obinay shereenÎncă nu există evaluări
- Case Study On GlomerulonephritisDocument20 paginiCase Study On GlomerulonephritisJosh AquinoÎncă nu există evaluări
- Pregnancy Induced Hypertension (PIH) : Case Scenario 4Document4 paginiPregnancy Induced Hypertension (PIH) : Case Scenario 4Mae Arra Lecobu-anÎncă nu există evaluări
- Revised BPHDocument2 paginiRevised BPHCyril Jane Caanyagan AcutÎncă nu există evaluări
- Idiopathic Thrombocytopenic Purpura (ITP)Document7 paginiIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiÎncă nu există evaluări
- Necrotising Enterocolitis (NEC) : Clinical Practice Guideline Guideline Coverage Includes NICU KEMH, NICU PMH and NETS WADocument3 paginiNecrotising Enterocolitis (NEC) : Clinical Practice Guideline Guideline Coverage Includes NICU KEMH, NICU PMH and NETS WAemilly vidyaÎncă nu există evaluări
- Bioterrorism: BY: - Bijay Kumar Mahato BPH 2 Semester Padmashree School of Public HealthDocument26 paginiBioterrorism: BY: - Bijay Kumar Mahato BPH 2 Semester Padmashree School of Public HealthBijay Kumar MahatoÎncă nu există evaluări
- OB2 - Renal and Urinary Tract Disorders in Pregnancy - Dr. TanDocument6 paginiOB2 - Renal and Urinary Tract Disorders in Pregnancy - Dr. TanHazel Fernandez VillarÎncă nu există evaluări
- 6100c73a72e89 3na Grand Case PresentationDocument208 pagini6100c73a72e89 3na Grand Case PresentationKim100% (1)
- Tetralogy of Fallot: Arianna Jasminemabunga Bsn-2BDocument30 paginiTetralogy of Fallot: Arianna Jasminemabunga Bsn-2BArianna Jasmine MabungaÎncă nu există evaluări
- UNIT IX - Application of Nursing Informatics (Clinical)Document201 paginiUNIT IX - Application of Nursing Informatics (Clinical)hoohooÎncă nu există evaluări
- Rheumatic Heart DiseaseDocument13 paginiRheumatic Heart Diseasedy15Încă nu există evaluări
- Family Health AssessmentDocument23 paginiFamily Health AssessmentPatrick Poculan100% (1)
- Volume ImpairmentDocument32 paginiVolume ImpairmentAcohCChaoÎncă nu există evaluări
- Ramos-2bn NCP Delivery RoomDocument2 paginiRamos-2bn NCP Delivery RoomLouwella RamosÎncă nu există evaluări
- FNCP CHN Day4 (Autosaved)Document106 paginiFNCP CHN Day4 (Autosaved)Shaira Ann CalambaÎncă nu există evaluări
- VKDBDocument11 paginiVKDBLucky PuspitasariÎncă nu există evaluări
- Prenatal Diagnosis JyDocument33 paginiPrenatal Diagnosis Jyjien_yeenÎncă nu există evaluări
- TLG IV TherapyDocument10 paginiTLG IV TherapyStephanie Joy EscalaÎncă nu există evaluări
- Hepatitis VirusDocument37 paginiHepatitis Virusapi-19916399Încă nu există evaluări
- Personal Data of Patient: Intensive Nursing Practicum - Pediatric Ward (BMC) CASE STUDY 5: Pediatric OncologyDocument12 paginiPersonal Data of Patient: Intensive Nursing Practicum - Pediatric Ward (BMC) CASE STUDY 5: Pediatric OncologyromelynÎncă nu există evaluări
- Ventricular Septal DefectDocument8 paginiVentricular Septal DefectMarina RotaruÎncă nu există evaluări
- Gestational HypertensionDocument5 paginiGestational HypertensionJason Jimmy Lee PillayÎncă nu există evaluări
- Amniotic Fluid EmbolismDocument34 paginiAmniotic Fluid EmbolismReygie MataÎncă nu există evaluări
- HemodialysisDocument11 paginiHemodialysisjuan_sioÎncă nu există evaluări
- CHN Rle Topic CompileDocument65 paginiCHN Rle Topic CompileYuuki Chitose (tai-kun)Încă nu există evaluări
- Prepared By: Sarah Diana Rise S. Manalili, RNDocument38 paginiPrepared By: Sarah Diana Rise S. Manalili, RNSARAH DIANA ROSE S. MANALILI100% (1)
- NCM 107-A Lecture 2012Document241 paginiNCM 107-A Lecture 2012Michael Anthony Ermita50% (2)
- 5 Maternal Adaptations To Pregnancy by Dr. Catherine Torres-JisonDocument75 pagini5 Maternal Adaptations To Pregnancy by Dr. Catherine Torres-JisonKevin AgbonesÎncă nu există evaluări
- Patient SafetyDocument102 paginiPatient SafetyAlain CheryÎncă nu există evaluări
- Fluid and Elctrolyte Balance.... Power PointDocument40 paginiFluid and Elctrolyte Balance.... Power PointMarwan M.100% (1)
- Abruptio PlacentaDocument5 paginiAbruptio PlacentaJuan Carlo Z. SolidumÎncă nu există evaluări
- PancreatitisDocument12 paginiPancreatitismardsz100% (5)
- Pamantasan NG Cabuyao: College of NursingDocument73 paginiPamantasan NG Cabuyao: College of NursingTrisha SuazoÎncă nu există evaluări
- Reflective ExemplarDocument2 paginiReflective Exemplarapi-531834240Încă nu există evaluări
- Pathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsDocument2 paginiPathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsAb Staholic Boii100% (1)
- GIT DiSEASES Dumping SyndromeDocument3 paginiGIT DiSEASES Dumping SyndromeLheidaniel MMM.Încă nu există evaluări
- Group 1 Family Case Study 1Document15 paginiGroup 1 Family Case Study 1Monique LeonardoÎncă nu există evaluări
- Normal Vital Signs Guidelines For EmsDocument2 paginiNormal Vital Signs Guidelines For Emsisabelo_laguraÎncă nu există evaluări
- Addison's Disease: Adrenal Insufficiency and Adrenal CrisisDocument15 paginiAddison's Disease: Adrenal Insufficiency and Adrenal CrisisMaryOÎncă nu există evaluări
- IMCI LectureDocument161 paginiIMCI LectureNaveen PandeyÎncă nu există evaluări
- 5 Diversity and Maternal Child NursingDocument50 pagini5 Diversity and Maternal Child NursingBryan Lloyd Ballestar RayatÎncă nu există evaluări
- Anaphylactic ReactionDocument9 paginiAnaphylactic ReactionZahir Jayvee Gayak IIÎncă nu există evaluări
- Nursing Informatics: Bachelor of Science in NursingDocument4 paginiNursing Informatics: Bachelor of Science in NursingMichelle MallareÎncă nu există evaluări
- Labor Watch DiscussionDocument28 paginiLabor Watch Discussioncoosa liquorsÎncă nu există evaluări
- Puerperal InfectionDocument11 paginiPuerperal InfectionceceyusenaÎncă nu există evaluări
- Maternal and Child Nursing 1 Skills Lab Modele s1Document3 paginiMaternal and Child Nursing 1 Skills Lab Modele s1Crystal MaidenÎncă nu există evaluări
- Patient ChartDocument2 paginiPatient ChartHydieÎncă nu există evaluări
- Maternal Midterm Reviewer Common ProblemsDocument58 paginiMaternal Midterm Reviewer Common ProblemsEya BaldostamonÎncă nu există evaluări
- FNCP Figueroa and de GuzmanDocument3 paginiFNCP Figueroa and de GuzmanDANIELA DE GUZMANÎncă nu există evaluări
- Accomplishment NICU-decDocument6 paginiAccomplishment NICU-decCecille AldayÎncă nu există evaluări
- PERSONAL REFLECTION and TEST YOURSELF - VHINCE PISCO IIIADocument3 paginiPERSONAL REFLECTION and TEST YOURSELF - VHINCE PISCO IIIAVhince Norben PiscoÎncă nu există evaluări
- Health Teaching PlanDocument9 paginiHealth Teaching PlanJeyser T. GamutiaÎncă nu există evaluări
- About Rubella: VaccineDocument5 paginiAbout Rubella: VaccinejudssalangsangÎncă nu există evaluări
- Chemical Injection OcrDocument4 paginiChemical Injection OcrJohnÎncă nu există evaluări
- Unable To Adapt TotDocument3 paginiUnable To Adapt TotJohnÎncă nu există evaluări
- Organize To InnovateDocument3 paginiOrganize To InnovateJohnÎncă nu există evaluări
- Insensitive To OthersprovementDocument3 paginiInsensitive To OthersprovementJohnÎncă nu există evaluări
- Lack of ComposuresDocument3 paginiLack of ComposuresJohnÎncă nu există evaluări
- Failure To Staff EffectivelymentDocument3 paginiFailure To Staff EffectivelymentJohnÎncă nu există evaluări
- Failure To Build A TeamementDocument3 paginiFailure To Build A TeamementJohnÎncă nu există evaluări
- Betrayal of TrusttDocument3 paginiBetrayal of TrusttJohnÎncă nu există evaluări
- SIAM Report On Mathematics in Industry (MII 2012)Document48 paginiSIAM Report On Mathematics in Industry (MII 2012)Madd MathsÎncă nu există evaluări
- Efficient Estimation Parameters NBDDocument23 paginiEfficient Estimation Parameters NBDJohnÎncă nu există evaluări
- Es9b03891 Si 001Document13 paginiEs9b03891 Si 001JohnÎncă nu există evaluări
- Lack of Ethics and ValuesntDocument3 paginiLack of Ethics and ValuesntJohnÎncă nu există evaluări
- Negative Binomial RegressionDocument36 paginiNegative Binomial RegressionJohnÎncă nu există evaluări
- Beta and Gamma FunctionsDocument32 paginiBeta and Gamma FunctionsSa'ad Abd Ar RafieÎncă nu există evaluări
- Beta and Gamma FunctionsDocument32 paginiBeta and Gamma FunctionsSa'ad Abd Ar RafieÎncă nu există evaluări
- LIT2007 Temp - Compensation - W - PH PDFDocument1 paginăLIT2007 Temp - Compensation - W - PH PDFJohnÎncă nu există evaluări
- Cryptography TheoryDocument76 paginiCryptography TheoryVickyÎncă nu există evaluări
- Table of Contents: PurgingDocument11 paginiTable of Contents: PurgingJohnÎncă nu există evaluări
- EAU Guidelines On Urolithiasis - 2017 - 10 05V2 PDFDocument84 paginiEAU Guidelines On Urolithiasis - 2017 - 10 05V2 PDFMelanie SalimÎncă nu există evaluări
- Exmax - Revolution: Compact - Easy Installation - Universal - Cost Effective - SafeDocument4 paginiExmax - Revolution: Compact - Easy Installation - Universal - Cost Effective - SafeJohnÎncă nu există evaluări
- Deposit Control Polymers For Stressed Phosphate-Based Cooling Water SystemsDocument15 paginiDeposit Control Polymers For Stressed Phosphate-Based Cooling Water SystemsJohnÎncă nu există evaluări
- Silica Analyzer - HACHDocument136 paginiSilica Analyzer - HACHSheikh ZakirÎncă nu există evaluări
- Cooling Water Analysis: by Ashutosh Mehndiratta Kribhco Shyam Fertilizers Limited Shahjahanpur Uttar Pradesh IndiaDocument39 paginiCooling Water Analysis: by Ashutosh Mehndiratta Kribhco Shyam Fertilizers Limited Shahjahanpur Uttar Pradesh IndiaJohnÎncă nu există evaluări
- Paper 8Document8 paginiPaper 8Veky PamintuÎncă nu există evaluări
- SIAM Report On Mathematics in Industry (MII 2012)Document48 paginiSIAM Report On Mathematics in Industry (MII 2012)Madd MathsÎncă nu există evaluări
- 475 Using Asme Performance Test Codes in TheDocument18 pagini475 Using Asme Performance Test Codes in Theaaa206Încă nu există evaluări
- TrigggonommeterDocument467 paginiTrigggonommeterJohnÎncă nu există evaluări
- Table of Contents: PurgingDocument11 paginiTable of Contents: PurgingJohnÎncă nu există evaluări
- EAU Guidelines On Urolithiasis - 2017 - 10 05V2 PDFDocument84 paginiEAU Guidelines On Urolithiasis - 2017 - 10 05V2 PDFMelanie SalimÎncă nu există evaluări
- Mfine CardiologistsDocument7 paginiMfine Cardiologistsmfine healthÎncă nu există evaluări
- Locked-In SyndromeDocument3 paginiLocked-In SyndromeBlogos CarlaÎncă nu există evaluări
- Mini Case Study 1Document14 paginiMini Case Study 1Casas, Jo-an Pauline A.Încă nu există evaluări
- MRCP Part 2 Sample Questions PDFDocument83 paginiMRCP Part 2 Sample Questions PDFamesbÎncă nu există evaluări
- Chapt 39Document7 paginiChapt 39Hakesh PratikÎncă nu există evaluări
- Paediatric Guidelines TorticollisDocument4 paginiPaediatric Guidelines TorticollisCatalin ChiriloiÎncă nu există evaluări
- Drugs For Congestive Heart FailureDocument46 paginiDrugs For Congestive Heart Failuresultan khabeeb100% (1)
- The Frequency of Dental Caries in Adult Patients With Gastroesophageal Reflux DiseaseDocument4 paginiThe Frequency of Dental Caries in Adult Patients With Gastroesophageal Reflux DiseasefdhfuwhuÎncă nu există evaluări
- Acute GlomerulonephritisDocument4 paginiAcute GlomerulonephritisJulliza Joy PandiÎncă nu există evaluări
- Benefits of Colostrum: The Missing Link in GI Health: Dr. Albert Snow Holistic GastroenterologistDocument25 paginiBenefits of Colostrum: The Missing Link in GI Health: Dr. Albert Snow Holistic GastroenterologistJayant SagadeÎncă nu există evaluări
- Acute AppendicitisDocument23 paginiAcute AppendicitisPrashant SinghÎncă nu există evaluări
- GPHC Pre-Registration Complete Exam Question List JUNE 2017 - NOV 2021Document50 paginiGPHC Pre-Registration Complete Exam Question List JUNE 2017 - NOV 2021Summer Sunshine TVÎncă nu există evaluări
- Document WPS OfficeDocument3 paginiDocument WPS OfficeWenalyn Grace Abella LlavanÎncă nu există evaluări
- Bulletproof MindDocument7 paginiBulletproof MindAdrian StanÎncă nu există evaluări
- O and G Notes Notebank NumberedDocument173 paginiO and G Notes Notebank NumberedPerscitus Ali القحطانيÎncă nu există evaluări
- Hemodialysis Nursing ConsiderationsDocument23 paginiHemodialysis Nursing ConsiderationsAR cerezaÎncă nu există evaluări
- Pages From MAF Nextcare 2Document1 paginăPages From MAF Nextcare 2Fahad ThahaÎncă nu există evaluări
- CerebellumDocument28 paginiCerebellumZoya MoraniÎncă nu există evaluări
- TUGAS 5 B.INGGRIS TigaDocument3 paginiTUGAS 5 B.INGGRIS TigaMesya FauziahÎncă nu există evaluări
- XIJU5502Document3 paginiXIJU5502Praveen ReddyÎncă nu există evaluări
- CM Handouts Clinical MicrosDocument33 paginiCM Handouts Clinical Microsrenato renato100% (1)
- Uro DynamicsDocument64 paginiUro DynamicsSri HariÎncă nu există evaluări
- Neurology Nursing Study GuideDocument19 paginiNeurology Nursing Study GuideHayleyLangley100% (5)
- RujukanDocument178 paginiRujukanPuskesmasBahagiaÎncă nu există evaluări
- Derma OSCEDocument3 paginiDerma OSCEUsama El BazÎncă nu există evaluări
- 4 6030444038488853198 PDFDocument110 pagini4 6030444038488853198 PDFSyeda Seri RazaÎncă nu există evaluări
- UNIT III GastrointestinalagentsAntacidDocument9 paginiUNIT III GastrointestinalagentsAntacidgalihÎncă nu există evaluări
- Hepatitis 10Document28 paginiHepatitis 10Matto RajputÎncă nu există evaluări
- Differential Diagnosis and Treatment of Gout and PseudogoutDocument18 paginiDifferential Diagnosis and Treatment of Gout and PseudogoutOlga GoryachevaÎncă nu există evaluări
- Part - 1 (Self Declaration) : Personal DetailsDocument2 paginiPart - 1 (Self Declaration) : Personal DetailsRitesh kumarÎncă nu există evaluări