S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- 10 11648 J Ajpn 20180604 12 PDFDocument5 pagini10 11648 J Ajpn 20180604 12 PDFAsti DwiningsihÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Aapm 08 06 81688Document6 paginiAapm 08 06 81688Asti DwiningsihÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Non-Pharmacological Methods and Post-Operative Pain Relief: An Observational StudyDocument7 paginiNon-Pharmacological Methods and Post-Operative Pain Relief: An Observational StudyAsti DwiningsihÎncă nu există evaluări
- Aripiprazol Versus Quetiapine in Treatment of Non-Affective Acute Psychosis: A Double-Blind, Randomized - Controlled Clinical TrialDocument4 paginiAripiprazol Versus Quetiapine in Treatment of Non-Affective Acute Psychosis: A Double-Blind, Randomized - Controlled Clinical TrialAsti DwiningsihÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Cognition of Schizophrenic Inpatients and Healthy Individuals: Casual-Comparative StudyDocument6 paginiCognition of Schizophrenic Inpatients and Healthy Individuals: Casual-Comparative StudyAsti DwiningsihÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- 10 11648 J Ajpn 20170504 11 PDFDocument5 pagini10 11648 J Ajpn 20170504 11 PDFAsti DwiningsihÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Psychoactive Substance Use Among Nigerian Students Patterns and Sociodemographic CorrelatesDocument4 paginiPsychoactive Substance Use Among Nigerian Students Patterns and Sociodemographic CorrelatesAsti DwiningsihÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Research ArticleDocument8 paginiResearch ArticleAsti DwiningsihÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- 1 s2.0 S0002939419300625 Main PDFDocument9 pagini1 s2.0 S0002939419300625 Main PDFAsti DwiningsihÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Pain Ladder - Acute Pain: Preferred and Alternative OptionsDocument1 paginăPain Ladder - Acute Pain: Preferred and Alternative OptionsAsti DwiningsihÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Research ArticleDocument7 paginiResearch ArticleAsti DwiningsihÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Anatomy and Physiology of Pain: Basic ScienceDocument5 paginiThe Anatomy and Physiology of Pain: Basic ScienceAsti DwiningsihÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Small Fatal Choroidal Melanoma Study. A Survey by The European Ophthalmic Oncology GroupDocument9 paginiThe Small Fatal Choroidal Melanoma Study. A Survey by The European Ophthalmic Oncology GroupAsti DwiningsihÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Clinical Study: Extreme Oncoplastic Surgery For Multifocal/Multicentric and Locally Advanced Breast CancerDocument9 paginiClinical Study: Extreme Oncoplastic Surgery For Multifocal/Multicentric and Locally Advanced Breast CancerAsti DwiningsihÎncă nu există evaluări
- Planning: Determine Patient's Clinical StatusDocument17 paginiPlanning: Determine Patient's Clinical StatusAsti DwiningsihÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Prevalence of Refractive Error Among School-Going Children of Imphal, ManipurDocument5 paginiPrevalence of Refractive Error Among School-Going Children of Imphal, ManipurAsti DwiningsihÎncă nu există evaluări
- Prevalence and Risk Factors of Refractive Errors Among Schoolchildren in Mashhad, 2006-2007Document7 paginiPrevalence and Risk Factors of Refractive Errors Among Schoolchildren in Mashhad, 2006-2007Asti DwiningsihÎncă nu există evaluări
- Osteoporosis, Konsumsi Susu, Jenis Kelamin, Umur, Dan Daerah, Di Dki Jakarta, Jawa Barat, Jawa Tengah, Dan Jawa TimurDocument7 paginiOsteoporosis, Konsumsi Susu, Jenis Kelamin, Umur, Dan Daerah, Di Dki Jakarta, Jawa Barat, Jawa Tengah, Dan Jawa TimurAsti DwiningsihÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Refractive Error, Visual Acuity and Causes of Vision Loss in Children in Shandong, China. The Shandong Children Eye StudyDocument12 paginiRefractive Error, Visual Acuity and Causes of Vision Loss in Children in Shandong, China. The Shandong Children Eye StudyAsti DwiningsihÎncă nu există evaluări
- Epidemiology of Vasomotor Rhinitis: Nar C P P, P 1Document4 paginiEpidemiology of Vasomotor Rhinitis: Nar C P P, P 1Asti DwiningsihÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Role of Anxiety, Depression and Anger in Eating Disorders-Structural ModelDocument5 paginiRole of Anxiety, Depression and Anger in Eating Disorders-Structural ModelAsti DwiningsihÎncă nu există evaluări
- Dementia Kuli A Hip DDocument4 paginiDementia Kuli A Hip DAsti DwiningsihÎncă nu există evaluări
- Main PDFDocument7 paginiMain PDFAsti DwiningsihÎncă nu există evaluări
- LP 20 Health Q3Document8 paginiLP 20 Health Q3Hazel Rubas SamsonÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Learning Plan Nursing PregradDocument3 paginiLearning Plan Nursing Pregradapi-25180064033% (3)
- TK Elevator 2020 21 Sustainability ReportDocument88 paginiTK Elevator 2020 21 Sustainability ReportmkyodaÎncă nu există evaluări
- Supw Project Medicinal PlantsDocument7 paginiSupw Project Medicinal Plantsmehal gupta75% (4)
- Meniere' S Disease: (Endolymphatic Hydrops)Document9 paginiMeniere' S Disease: (Endolymphatic Hydrops)WillieÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- YOUR Guide To Chest ClearanceDocument2 paginiYOUR Guide To Chest ClearanceDr Abdallah BahaaÎncă nu există evaluări
- Unit 01 OTHMDocument45 paginiUnit 01 OTHMsam100% (4)
- The Right To Die: Pre-ReadingDocument8 paginiThe Right To Die: Pre-ReadingGiovanni EscobarÎncă nu există evaluări
- Clinical Practice Guidelines: BY: Ma. Sylvia Emilie B. BeñalesDocument17 paginiClinical Practice Guidelines: BY: Ma. Sylvia Emilie B. Beñalespaulyn ramosÎncă nu există evaluări
- Mrs. Garima Chauhan - TechnostressDocument68 paginiMrs. Garima Chauhan - TechnostressMukesh ChauhanÎncă nu există evaluări
- Promotive and Preventive Health Aspect in CHN & Facts On Healthcare in PHDocument2 paginiPromotive and Preventive Health Aspect in CHN & Facts On Healthcare in PH2A - Nicole Marrie HonradoÎncă nu există evaluări
- Annotated BibliographyDocument20 paginiAnnotated Bibliographyapi-347153077Încă nu există evaluări
- QMDocument12 paginiQMGs AbhilashÎncă nu există evaluări
- Webinar Lung CancerDocument53 paginiWebinar Lung CancerJose Flores FernandezÎncă nu există evaluări
- Brochure ISDocument4 paginiBrochure ISJAYESH VIKRAM RastogiÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Clinical Applied Anatomy in Wound CareDocument18 paginiClinical Applied Anatomy in Wound CareKlinik Komuniti Perwira100% (2)
- The Role of Health-Related Behaviors in The Socioeconomic Disparities in Oral HealthDocument6 paginiThe Role of Health-Related Behaviors in The Socioeconomic Disparities in Oral HealthStephanyÎncă nu există evaluări
- IvabradineDocument30 paginiIvabradinepashaÎncă nu există evaluări
- Small Changes, Big Results, Revised and UpdatedDocument18 paginiSmall Changes, Big Results, Revised and UpdatedThe Recipe Club100% (1)
- School Facilities and Observation ChecklistDocument5 paginiSchool Facilities and Observation ChecklistMhadellaine JunatasÎncă nu există evaluări
- Chronic Renal Failure Nursing Care PlanDocument6 paginiChronic Renal Failure Nursing Care PlanRuva Oscass JimmyÎncă nu există evaluări
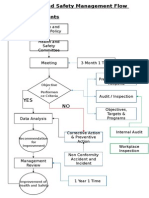
- Health and Safety FlowDocument6 paginiHealth and Safety Flowzaki0304Încă nu există evaluări
- Intradermal Delivery Vaccines Report 2009 SeptDocument94 paginiIntradermal Delivery Vaccines Report 2009 SeptSantoso CokroÎncă nu există evaluări
- Systemic Review On The Use of Diclofenacb Complex As An Antiinflammatorytreatment With Pain Relief Effect For Patients With Acute Lower Back Pain 2167 0846 1000216Document5 paginiSystemic Review On The Use of Diclofenacb Complex As An Antiinflammatorytreatment With Pain Relief Effect For Patients With Acute Lower Back Pain 2167 0846 1000216Dhea Yulia LubisÎncă nu există evaluări
- 002 - 1203 - Ni Wayan Ari Anindita Sari - GalleyDocument5 pagini002 - 1203 - Ni Wayan Ari Anindita Sari - GalleyHaningtyas IndahÎncă nu există evaluări
- The Gullah People of Souhth Carolina (Draft) (012914)Document20 paginiThe Gullah People of Souhth Carolina (Draft) (012914)Grissett Tony100% (2)
- Lect 3 Trauma CounsellingDocument28 paginiLect 3 Trauma Counsellingumibrahim75% (8)
- Lecture 5 First Aid and Antidotes Against Pesticides PoisoningDocument45 paginiLecture 5 First Aid and Antidotes Against Pesticides PoisoningMuhammad Shahrooz NaseerÎncă nu există evaluări
- I. Introduction To Special EducationDocument9 paginiI. Introduction To Special EducationJennylyn Boiser100% (1)
- Thesis About Quack DoctorsDocument22 paginiThesis About Quack DoctorsJervyn Guianan100% (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (29)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)