S-ar putea să vă placă și
- The Everything Book for Child Care & Preschool, Ages 3 - 5De la EverandThe Everything Book for Child Care & Preschool, Ages 3 - 5Încă nu există evaluări
- 2009-SUPPORT Tools For Evidence-Informed Policymaking in Health 18-Planning Monitoring and Evaluation of PoliciesDocument8 pagini2009-SUPPORT Tools For Evidence-Informed Policymaking in Health 18-Planning Monitoring and Evaluation of PoliciesJULIO CESAR MATEUS SOLARTEÎncă nu există evaluări
- 2009-SUPPORT Tools For Evidence-Informed Policymaking in Health 11-Finding and Using Evidence About Local ConditionsDocument14 pagini2009-SUPPORT Tools For Evidence-Informed Policymaking in Health 11-Finding and Using Evidence About Local ConditionsJULIO CESAR MATEUS SOLARTEÎncă nu există evaluări
- Health Research Policy and Systems: SUPPORT Tools For Evidence-Informed Health Policymaking (STP)Document7 paginiHealth Research Policy and Systems: SUPPORT Tools For Evidence-Informed Health Policymaking (STP)BDOC2010Încă nu există evaluări
- 2009-SUPPORT Tools For Evidence-Informed Policymaking in Health 16-Using Research Evidence in Balancing The Pros and Cons of PoliciesDocument9 pagini2009-SUPPORT Tools For Evidence-Informed Policymaking in Health 16-Using Research Evidence in Balancing The Pros and Cons of PoliciesJULIO CESAR MATEUS SOLARTEÎncă nu există evaluări
- 2009-SUPPORT Tools For Evidence-Informed Health Policymaking (STP) 12-Finding and Using Research Evidence About Resource Use and CostsDocument9 pagini2009-SUPPORT Tools For Evidence-Informed Health Policymaking (STP) 12-Finding and Using Research Evidence About Resource Use and CostsJULIO CESAR MATEUS SOLARTEÎncă nu există evaluări
- 2009-SUPPORT Tools For Evidence-Informed Policymaking in Health 15-Engaging The Public in Evidence-Informed PolicymakingDocument9 pagini2009-SUPPORT Tools For Evidence-Informed Policymaking in Health 15-Engaging The Public in Evidence-Informed PolicymakingJULIO CESAR MATEUS SOLARTEÎncă nu există evaluări
- 2009-SUPPORT Tools For Evidence-Informed Health Policymaking (STP) 8 - Deciding How Much Confidence To Place in A Systematic ReviewDocument13 pagini2009-SUPPORT Tools For Evidence-Informed Health Policymaking (STP) 8 - Deciding How Much Confidence To Place in A Systematic ReviewJULIO CESAR MATEUS SOLARTEÎncă nu există evaluări
- 2009-SUPPORT Tools For Evidence-Informed Health Policymaking (STP) 14-Organising and Using Policy Dialogues To Support Evidence-Informed PolicymakingDocument8 pagini2009-SUPPORT Tools For Evidence-Informed Health Policymaking (STP) 14-Organising and Using Policy Dialogues To Support Evidence-Informed PolicymakingJULIO CESAR MATEUS SOLARTEÎncă nu există evaluări
- Prime Newsletter Issue 12Document16 paginiPrime Newsletter Issue 12javedperfusionistÎncă nu există evaluări
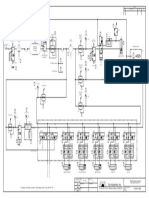
- References:: For Higher Level Shutdown Matrix See Document PCSE-100-ET-Y-600Document2 paginiReferences:: For Higher Level Shutdown Matrix See Document PCSE-100-ET-Y-600Carlos Aquino HanccoÎncă nu există evaluări
- How To Read A Value Line ReportDocument15 paginiHow To Read A Value Line ReportJamie GiannaÎncă nu există evaluări
- 00258-FOIA RequestDocument10 pagini00258-FOIA RequestlegalmattersÎncă nu există evaluări
- V0.1Document1 paginăV0.1Thea Marie M HernandezÎncă nu există evaluări
- Star Infratech Report - Nov 2020Document22 paginiStar Infratech Report - Nov 2020yashas sÎncă nu există evaluări
- Past Defect History 2021Document10 paginiPast Defect History 2021RahulÎncă nu există evaluări
- Competence Format ExampleDocument10 paginiCompetence Format ExampleAbraham GutierrezÎncă nu există evaluări
- V1.1Document1 paginăV1.1Thea Marie M HernandezÎncă nu există evaluări
- 000-A-Pro-50075-001-R0 Hse Training PlanDocument22 pagini000-A-Pro-50075-001-R0 Hse Training PlansantoshÎncă nu există evaluări
- 2103-P-001-Of Rev0 - RolleChim FA ProcessDocument10 pagini2103-P-001-Of Rev0 - RolleChim FA ProcessfahminzÎncă nu există evaluări
- MSDS Biopuro Ammorbidente EngDocument7 paginiMSDS Biopuro Ammorbidente EngMarta LuzÎncă nu există evaluări
- 000 M TSP 50002 001 R0aDocument61 pagini000 M TSP 50002 001 R0aJoaquim FernandesÎncă nu există evaluări
- Sample: Audit Program For As/400 (Iseries, System I) and Os/400 (I5/Os, Ibm I)Document9 paginiSample: Audit Program For As/400 (Iseries, System I) and Os/400 (I5/Os, Ibm I)Chinh Lê ĐìnhÎncă nu există evaluări
- 11 PB 21-07-2017 STP Progress DashboardDocument4 pagini11 PB 21-07-2017 STP Progress DashboardEiriedÎncă nu există evaluări
- New Maps: From Tigran's Upcoming Album The Call Within'Document18 paginiNew Maps: From Tigran's Upcoming Album The Call Within'Anton Mikhailov100% (2)
- Aval Aase 2324 FinalDocument1 paginăAval Aase 2324 Finalguihermatador45Încă nu există evaluări
- Sun Industries, Inc.: For Foldover, Card Feeder, & Product Transfer Diagrams Refer To Dwg. #P/8-96-1001Document1 paginăSun Industries, Inc.: For Foldover, Card Feeder, & Product Transfer Diagrams Refer To Dwg. #P/8-96-1001Carl PotschÎncă nu există evaluări
- 2018 Instruments CatalogueDocument44 pagini2018 Instruments Cataloguevenkata.krishnanÎncă nu există evaluări
- Waterfall Large LC QuickRef v1.2Document1 paginăWaterfall Large LC QuickRef v1.2Swarup NakkaÎncă nu există evaluări
- Chapter 2 Formulation and Verification of Accounting TheoryDocument1 paginăChapter 2 Formulation and Verification of Accounting Theoryammar beatlesÎncă nu există evaluări
- NParks Org StructureDocument1 paginăNParks Org StructureNPAR09Încă nu există evaluări
- COCO P3 EXE TOYO PCE 000 STA GA 0002 AYBJ00120 - Rev.0 - APDocument5 paginiCOCO P3 EXE TOYO PCE 000 STA GA 0002 AYBJ00120 - Rev.0 - APNazrilMizarÎncă nu există evaluări
- Business Excellence AwardDocument18 paginiBusiness Excellence AwardKarthikeyan NatarajanÎncă nu există evaluări
- Pana DocsDocument3 paginiPana DocsRoberto ColtellacciÎncă nu există evaluări
- Value Stream Improvement Plan TemplateDocument4 paginiValue Stream Improvement Plan TemplatemilandivacÎncă nu există evaluări
- Hatch Jack - 1304 - ScannedDocument3 paginiHatch Jack - 1304 - ScannedZach EdwardsÎncă nu există evaluări
- Dangerous Substances: Handle With CareDocument39 paginiDangerous Substances: Handle With CareYacine.DaoudiÎncă nu există evaluări
- COCO P3 EXE TOYO PCE 000 STA GA 0001 AYBJ00120 - Rev.0 - APDocument3 paginiCOCO P3 EXE TOYO PCE 000 STA GA 0001 AYBJ00120 - Rev.0 - APNazrilMizarÎncă nu există evaluări
- 000-A-Pro-50106-001-R0 Grievance ProcedureDocument11 pagini000-A-Pro-50106-001-R0 Grievance ProceduresantoshÎncă nu există evaluări
- Shortlist 2Document1 paginăShortlist 2rahul dandonaÎncă nu există evaluări
- PM One Page FlowchartDocument1 paginăPM One Page FlowchartbenÎncă nu există evaluări
- PT Jawa Tirtamarin Form Keselamatan, Kesehatan Kerja Dan Perlindungan Lingkungan Statistik Keselamatan Dan Kesehatan KerjaDocument1 paginăPT Jawa Tirtamarin Form Keselamatan, Kesehatan Kerja Dan Perlindungan Lingkungan Statistik Keselamatan Dan Kesehatan Kerjaimam santosoÎncă nu există evaluări
- PT Jawa Tirtamarin Form Keselamatan, Kesehatan Kerja Dan Perlindungan Lingkungan Statistik Keselamatan Dan Kesehatan KerjaDocument1 paginăPT Jawa Tirtamarin Form Keselamatan, Kesehatan Kerja Dan Perlindungan Lingkungan Statistik Keselamatan Dan Kesehatan Kerjaimam santosoÎncă nu există evaluări
- New Zealand Aid Programme Strategic Plan 2015 19Document13 paginiNew Zealand Aid Programme Strategic Plan 2015 19Djamnur AgnessiaÎncă nu există evaluări
- Poster I Icep 2019Document1 paginăPoster I Icep 2019Eduardo OliveiraÎncă nu există evaluări
- G-102-01 (790DBBC) Al-Shahaniya: Qatar Armed ForcesDocument1 paginăG-102-01 (790DBBC) Al-Shahaniya: Qatar Armed ForcesAslamÎncă nu există evaluări
- Report On Issues Observed in Waterproofing Apllication at B6 L07 Cleaning Room and Disable BathroomDocument4 paginiReport On Issues Observed in Waterproofing Apllication at B6 L07 Cleaning Room and Disable BathroomYasith AbeywickramaÎncă nu există evaluări
- Middle School Mystery Genre UnitDocument57 paginiMiddle School Mystery Genre Unitmjgayles75% (12)
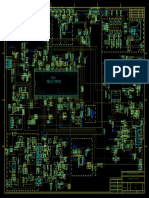
- npm6 Schematics v1 0Document10 pagininpm6 Schematics v1 0Владимир КлюевÎncă nu există evaluări
- BGFBFGBDocument1 paginăBGFBFGBDarren ValienteÎncă nu există evaluări
- LBP A3 Example Office Case StudyDocument1 paginăLBP A3 Example Office Case StudyOsvaldo ColinÎncă nu există evaluări
- Schematic VenusDocument1 paginăSchematic VenusDebjeet ChakrabortyÎncă nu există evaluări
- Assessment Packages Electrician Level IIDocument22 paginiAssessment Packages Electrician Level IISheela AliÎncă nu există evaluări
- Resume File: Health Care Cert. Full-Time Part-Time Remote Worker Future HireDocument1 paginăResume File: Health Care Cert. Full-Time Part-Time Remote Worker Future HireAbdullah FasehÎncă nu există evaluări
- Risk Management Tools (CAMO-TAM-ASOG - WSOG)Document1 paginăRisk Management Tools (CAMO-TAM-ASOG - WSOG)AndriyÎncă nu există evaluări
- Central Finance 1709Document38 paginiCentral Finance 1709Romain DepÎncă nu există evaluări
- IONIX ModelDocument6 paginiIONIX ModelTrường Bửu TrầnÎncă nu există evaluări
- 7.2. Form Rencana Pelatihan Dan Pembinaan Karyawan - 071020Document1 pagină7.2. Form Rencana Pelatihan Dan Pembinaan Karyawan - 071020Wage KarsanaÎncă nu există evaluări
- Pe 5Document5 paginiPe 5Santhosh Hero SantoÎncă nu există evaluări
- Description: Tags: 08progcompDocument5 paginiDescription: Tags: 08progcompanon-416085Încă nu există evaluări
- Rapidly Progressive Dementias - Aetiologies, Diagnosis and ManagementDocument14 paginiRapidly Progressive Dementias - Aetiologies, Diagnosis and ManagementFelipe González RodríguezÎncă nu există evaluări
- Antibiotic Therapy: What Factors Influence Antibiotic Choice in Critically Ill Patients?Document5 paginiAntibiotic Therapy: What Factors Influence Antibiotic Choice in Critically Ill Patients?Felipe González RodríguezÎncă nu există evaluări
- Genetics of Coenzyme Q 10 DeficiencyDocument7 paginiGenetics of Coenzyme Q 10 DeficiencyFelipe González RodríguezÎncă nu există evaluări
- No Surprises - RadioheadDocument1 paginăNo Surprises - RadioheadFelipe González RodríguezÎncă nu există evaluări
- National Policy For Person With Disabilities, 2006Document7 paginiNational Policy For Person With Disabilities, 2006Vijay100% (2)
- PAK-301 Assignment 1 Solution Spring 2021Document4 paginiPAK-301 Assignment 1 Solution Spring 2021Muhammad Ali HussainÎncă nu există evaluări
- Global Interstate SystemDocument4 paginiGlobal Interstate SystemKAYERAVEN MORANTEÎncă nu există evaluări
- mgmt3081 Course OutlineDocument4 paginimgmt3081 Course OutlineStephen M. NeilÎncă nu există evaluări
- Moot CourtDocument7 paginiMoot CourtHimanshu GoenkaÎncă nu există evaluări
- Vanesssa Nyoni Dissertation First Draft SubmitionDocument73 paginiVanesssa Nyoni Dissertation First Draft SubmitionBELIEVE EDSON TENGEMHAREÎncă nu există evaluări
- Legal Notes - Module Two: 1. Your Rights and ResponsibilitiesDocument9 paginiLegal Notes - Module Two: 1. Your Rights and Responsibilitiesabudy2147Încă nu există evaluări
- Globalisation PDFDocument4 paginiGlobalisation PDFHiviÎncă nu există evaluări
- Political Culture - A Pattern of Shared Values, Moral, Norms, Beliefs, Expectations and Attitudes That RelateDocument5 paginiPolitical Culture - A Pattern of Shared Values, Moral, Norms, Beliefs, Expectations and Attitudes That RelateDexterJohnN.BambalanÎncă nu există evaluări
- Brics New Development Bank: Perbandingan Sistem Pinjaman IMF Dan Serta Potensi Dominasi Sistem Moneter InternasionalDocument17 paginiBrics New Development Bank: Perbandingan Sistem Pinjaman IMF Dan Serta Potensi Dominasi Sistem Moneter InternasionalMuhammad Fiqri MajitÎncă nu există evaluări
- LLDA Vs CA - Case DigestDocument1 paginăLLDA Vs CA - Case DigestOM MolinsÎncă nu există evaluări
- Republic of The Philippines Department of Social and DevelopmentDocument41 paginiRepublic of The Philippines Department of Social and DevelopmentEden Gel MacawileÎncă nu există evaluări
- A Systems Theory of GovernanceDocument35 paginiA Systems Theory of GovernanceCyrusKayani75% (4)
- Social Responsibilities Are A Part of All ProfessionsDocument2 paginiSocial Responsibilities Are A Part of All ProfessionsMuhammad Danish FahimÎncă nu există evaluări
- Rural Institutions in The Philippine SettingsDocument2 paginiRural Institutions in The Philippine SettingsVitas VitalyÎncă nu există evaluări
- Rts Medicines 7778-1Document79 paginiRts Medicines 7778-1sam yadavÎncă nu există evaluări
- Taxation and Fiscal Policy: First Semester 2020/2021Document33 paginiTaxation and Fiscal Policy: First Semester 2020/2021emeraldÎncă nu există evaluări
- She Strategy DocumentDocument30 paginiShe Strategy DocumentEarnest A. Bartlett100% (2)
- Testing of All Equipment Components and Parts Imported For Use in TheDocument2 paginiTesting of All Equipment Components and Parts Imported For Use in Thesarita kumariÎncă nu există evaluări
- ScienceDirect 1-S2.0-S1389934123000461-MainDocument8 paginiScienceDirect 1-S2.0-S1389934123000461-Mainsaritadewi03Încă nu există evaluări
- Assignment On Bangladesh Studies Topic: Course Code: Submitted ToDocument9 paginiAssignment On Bangladesh Studies Topic: Course Code: Submitted Tozeorna StoreÎncă nu există evaluări
- Samuels - Proposal Writing For Business Research Projects-Routledge 2022Document136 paginiSamuels - Proposal Writing For Business Research Projects-Routledge 2022juanÎncă nu există evaluări
- Public International Law Atty. Ganchoon: Traditional DefinitionDocument2 paginiPublic International Law Atty. Ganchoon: Traditional DefinitionJajang Mimid100% (1)
- Labor Law MQ1Document10 paginiLabor Law MQ1shaneÎncă nu există evaluări
- Marcos v. Manglapus, G.R. No. 88211, 15 September 1989Document6 paginiMarcos v. Manglapus, G.R. No. 88211, 15 September 1989Ming YaoÎncă nu există evaluări
- Session 1 Introduction To The Nature of CbaDocument51 paginiSession 1 Introduction To The Nature of CbaMohamed MustefaÎncă nu există evaluări
- GP Past Paper 2020 Varient 2 InsertDocument5 paginiGP Past Paper 2020 Varient 2 InsertetryoiÎncă nu există evaluări
- Brokenshire Memorial Hospital, Inc. vs. Minister of Labor and EmploymentDocument8 paginiBrokenshire Memorial Hospital, Inc. vs. Minister of Labor and EmploymentJoanne CamacamÎncă nu există evaluări
- W8 Policy Diffusion Seven LessonsDocument10 paginiW8 Policy Diffusion Seven LessonsLucia Charlón GonzálezÎncă nu există evaluări
- Policies and ProgrammesDocument1 paginăPolicies and ProgrammesKhushiÎncă nu există evaluări