S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- CXC - Past - Paper - 2022 Solutions PDFDocument17 paginiCXC - Past - Paper - 2022 Solutions PDFDarren Fraser100% (1)
- The Emom Manual: 25 Kettlebell Conditioning WorkoutsDocument14 paginiThe Emom Manual: 25 Kettlebell Conditioning WorkoutsguilleÎncă nu există evaluări
- Maxillofacial Notes DR - Mahmoud RamadanDocument83 paginiMaxillofacial Notes DR - Mahmoud Ramadanaziz200775% (4)
- Project Management A Technicians Guide Staples TOCDocument5 paginiProject Management A Technicians Guide Staples TOCAnonymous NwnJNO0% (3)
- Isolation Guidelines PDFDocument209 paginiIsolation Guidelines PDFlimiya vargheseÎncă nu există evaluări
- Adsorbents and Adsorption Processes For Pollution ControlDocument30 paginiAdsorbents and Adsorption Processes For Pollution ControlJoao MinhoÎncă nu există evaluări
- Bhert - EoDocument2 paginiBhert - EoRose Mae LambanecioÎncă nu există evaluări
- Dr. Nastiti K - Manajemen Asma Pada Anak 2018 PDFDocument72 paginiDr. Nastiti K - Manajemen Asma Pada Anak 2018 PDFagnesspratiwiÎncă nu există evaluări
- jmf.2018.0160 EndometriosisDocument8 paginijmf.2018.0160 EndometriosisRominaÎncă nu există evaluări
- jmf.2018.0160 EndometriosisDocument8 paginijmf.2018.0160 EndometriosisRominaÎncă nu există evaluări
- Journal - Pone.0227695 EndometriosisDocument13 paginiJournal - Pone.0227695 EndometriosisRominaÎncă nu există evaluări
- Meta-Analysis of Social Cognition in Amyotrophic Lateral SclerosisDocument7 paginiMeta-Analysis of Social Cognition in Amyotrophic Lateral SclerosisRominaÎncă nu există evaluări
- Verbos Regulares en InglésDocument7 paginiVerbos Regulares en InglésAlyson MoralesÎncă nu există evaluări
- Verbos Irregulares en InglésDocument4 paginiVerbos Irregulares en InglésAlyson MoralesÎncă nu există evaluări
- Biopolymers: Overview of Several Properties and Consequences On Their ApplicationsDocument10 paginiBiopolymers: Overview of Several Properties and Consequences On Their ApplicationsrafacpereiraÎncă nu există evaluări
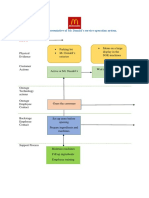
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDocument2 paginiBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênÎncă nu există evaluări
- United States v. Victor Vallin-Jauregui, 4th Cir. (2013)Document4 paginiUnited States v. Victor Vallin-Jauregui, 4th Cir. (2013)Scribd Government DocsÎncă nu există evaluări
- Advances of Family Apocynaceae A Review - 2017Document30 paginiAdvances of Family Apocynaceae A Review - 2017Владимир ДружининÎncă nu există evaluări
- IPG Or-01 - PTC Train Infrastructure Electrical Safety RulesDocument50 paginiIPG Or-01 - PTC Train Infrastructure Electrical Safety Rules4493464Încă nu există evaluări
- Oil ShaleDocument13 paginiOil Shalergopi_83Încă nu există evaluări
- 41 Assignment Worksheets For SchoolDocument26 pagini41 Assignment Worksheets For Schoolsoinarana456Încă nu există evaluări
- 3 Activities For Adults To Practice Modeling SELDocument10 pagini3 Activities For Adults To Practice Modeling SELDavid Garcia PerezÎncă nu există evaluări
- FINAL PAPER Marketing Plan For Rainbow Air PurifierDocument12 paginiFINAL PAPER Marketing Plan For Rainbow Air PurifierMohola Tebello Griffith100% (1)
- READING 4 UNIT 8 Crime-Nurse Jorge MonarDocument3 paginiREADING 4 UNIT 8 Crime-Nurse Jorge MonarJORGE ALEXANDER MONAR BARRAGANÎncă nu există evaluări
- Dressmaking - Q1 TASK-SHEET v1 - Schalemar OmbionDocument2 paginiDressmaking - Q1 TASK-SHEET v1 - Schalemar OmbionAlvaCatalinaÎncă nu există evaluări
- Ventricular Septal DefectDocument8 paginiVentricular Septal DefectWidelmark FarrelÎncă nu există evaluări
- Soal UAS Bahasa Inggris 2015/2016: Read The Text Carefully! Cold Comfort TeaDocument5 paginiSoal UAS Bahasa Inggris 2015/2016: Read The Text Carefully! Cold Comfort TeaAstrid AlifkalailaÎncă nu există evaluări
- PEOPLE V JAURIGUE - Art 14 Aggravating CircumstancesDocument2 paginiPEOPLE V JAURIGUE - Art 14 Aggravating CircumstancesLady Diana TiangcoÎncă nu există evaluări
- CrewmgtDocument36 paginiCrewmgtDoddy HarwignyoÎncă nu există evaluări
- Epo-Fix Plus: High-Performance Epoxy Chemical AnchorDocument3 paginiEpo-Fix Plus: High-Performance Epoxy Chemical Anchormilivoj ilibasicÎncă nu există evaluări
- Crime Data Analysis 1Document2 paginiCrime Data Analysis 1kenny laroseÎncă nu există evaluări
- Food Processing NC II - SAGDocument4 paginiFood Processing NC II - SAGNylmazdahr Sañeud DammahomÎncă nu există evaluări
- PPR Soft Copy Ayurvedic OkDocument168 paginiPPR Soft Copy Ayurvedic OkKetan KathaneÎncă nu există evaluări
- Fill The Gaps With The Correct WordsDocument2 paginiFill The Gaps With The Correct WordsAlayza ChangÎncă nu există evaluări
- Chapter Three Liquid Piping SystemDocument51 paginiChapter Three Liquid Piping SystemMelaku TamiratÎncă nu există evaluări
- ZJZJP Roots Vauum PumpDocument8 paginiZJZJP Roots Vauum PumpAnonymous Tj3ApePIrÎncă nu există evaluări
- Heat Transfer ExampleDocument4 paginiHeat Transfer Examplekero_the_heroÎncă nu există evaluări