S-ar putea să vă placă și
- Chinese Veterinary Herbal Handbook 3 RD EditionDocument19 paginiChinese Veterinary Herbal Handbook 3 RD EditionPerpetua Kamikadze0% (4)
- SS 6e Manager Sample-ChapterDocument32 paginiSS 6e Manager Sample-ChapterIrmita Prameswari Wijayanti100% (2)
- Calgevax BSG Bugarska EngDocument10 paginiCalgevax BSG Bugarska EngAnonymous idBsC1Încă nu există evaluări
- Project On MalnutritionDocument14 paginiProject On MalnutritionVijay M100% (2)
- CASE PRESENTATION ON UTI Case 3Document14 paginiCASE PRESENTATION ON UTI Case 3Safoora RafeeqÎncă nu există evaluări
- Chapter 28: Obstructive Pulmonary Diseases Harding: Lewis's Medical-Surgical Nursing, 11th EditionDocument15 paginiChapter 28: Obstructive Pulmonary Diseases Harding: Lewis's Medical-Surgical Nursing, 11th EditionKrishna RamaÎncă nu există evaluări
- HBVAXPRO LeafletDocument100 paginiHBVAXPRO LeafletEllaÎncă nu există evaluări
- Pentaxim-Pi-Sg Pen 0118 Spc0914Document10 paginiPentaxim-Pi-Sg Pen 0118 Spc0914walkrogÎncă nu există evaluări
- Drug Study Clindamycin, Ipatropium BromideDocument8 paginiDrug Study Clindamycin, Ipatropium Bromidepaupaulala100% (2)
- HiberixinjDocument10 paginiHiberixinjded02785Încă nu există evaluări
- Sinopharm Vaccine - Guidelines - 06 - 06 - 2021updateDocument18 paginiSinopharm Vaccine - Guidelines - 06 - 06 - 2021updateChinthana චින්තනÎncă nu există evaluări
- COvid 19 Vaccine JanssenDocument17 paginiCOvid 19 Vaccine JanssenAsperoÎncă nu există evaluări
- Annex I Summary of Product CharacteristicsDocument35 paginiAnnex I Summary of Product Characteristicsmihaela vlad100% (1)
- Covid 19 Vaccine Astra ZenecainjDocument17 paginiCovid 19 Vaccine Astra ZenecainjGlowstarÎncă nu există evaluări
- DrugsDocument2 paginiDrugsgailannreyesÎncă nu există evaluări
- DrugsDocument2 paginiDrugsgailannreyesÎncă nu există evaluări
- Annex I Summary of Product CharacteristicsDocument33 paginiAnnex I Summary of Product CharacteristicsEva DominguezÎncă nu există evaluări
- Annex I Summary of Product CharacteristicsDocument33 paginiAnnex I Summary of Product CharacteristicsMohamed AllamÎncă nu există evaluări
- 0 BatchDocument34 pagini0 BatchRahul MehtaÎncă nu există evaluări
- ZegenDocument9 paginiZegenJefferson ManasanÎncă nu există evaluări
- AIIMS Issues New Guidelines For Treatment of CovidDocument7 paginiAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarÎncă nu există evaluări
- Drug Study QiDocument7 paginiDrug Study QiJeremiah Mauricio100% (1)
- FAQs For Doctors-PEDIADocument11 paginiFAQs For Doctors-PEDIAzzÎncă nu există evaluări
- AIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)Document7 paginiAIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)senthil kumarÎncă nu există evaluări
- Drug StudyDocument4 paginiDrug StudyMariel Colminas100% (1)
- Pentavalent VaccineDocument18 paginiPentavalent VaccineSabita Paudel100% (1)
- Kiss Covid VaccinationsDocument4 paginiKiss Covid VaccinationsMohamed Ali KalathingalÎncă nu există evaluări
- Nclex 3 With RationaleDocument13 paginiNclex 3 With RationaleMsPocketbook HoarderÎncă nu există evaluări
- Name of The Medicinal Product: Short-Term TreatmentDocument10 paginiName of The Medicinal Product: Short-Term TreatmentasdwasdÎncă nu există evaluări
- Generic Name: Albuterol Brand Name: Salbutamol, Proventil, Ventolin, Accuneb, Airet, Novo-SalbutamolDocument26 paginiGeneric Name: Albuterol Brand Name: Salbutamol, Proventil, Ventolin, Accuneb, Airet, Novo-SalbutamolAnna Joy Antone100% (1)
- Reg 174 Information For Uk Healthcare ProfessionalsDocument11 paginiReg 174 Information For Uk Healthcare ProfessionalsFranciscoÎncă nu există evaluări
- Qdenga Epar Product Information enDocument47 paginiQdenga Epar Product Information enNovrina Wahidah RestiÎncă nu există evaluări
- National Immunisation ScheduleDocument33 paginiNational Immunisation ScheduleVignesh ArumugamÎncă nu există evaluări
- Reg 174 Information For Uk Healthcare ProfessionalsDocument13 paginiReg 174 Information For Uk Healthcare ProfessionalsIce BallÎncă nu există evaluări
- Tetravac Suspension For Injection ENG SMPCDocument15 paginiTetravac Suspension For Injection ENG SMPCFelix Daniel ParvuÎncă nu există evaluări
- Reg 174 Information For Uk Healthcare ProfessionalsDocument11 paginiReg 174 Information For Uk Healthcare ProfessionalsSelenaÎncă nu există evaluări
- AbatacepteDocument5 paginiAbatacepteSuh TeixeiraÎncă nu există evaluări
- Name of DrugDocument17 paginiName of DrugAllan DiazÎncă nu există evaluări
- 14h30 26-Mar 21078 JanssenDocument6 pagini14h30 26-Mar 21078 JanssenSavu BogdanÎncă nu există evaluări
- Meropenem - Drug Information - UpToDate-3Document8 paginiMeropenem - Drug Information - UpToDate-3Vh TRÎncă nu există evaluări
- 2018 10 10 002356file1Document2 pagini2018 10 10 002356file1Одончимэг СайханбаярÎncă nu există evaluări
- Annex I Summary of Product CharacteristicsDocument33 paginiAnnex I Summary of Product CharacteristicsVimala BohoÎncă nu există evaluări
- TETAVAXDocument4 paginiTETAVAXAshraf Sabbir100% (1)
- 11adult Vaccination Dec03Document86 pagini11adult Vaccination Dec03Kokoland KukusÎncă nu există evaluări
- Imipenem, Cilastatin, and Relebactam - Drug Information - UpToDateDocument10 paginiImipenem, Cilastatin, and Relebactam - Drug Information - UpToDateMarius PapuricaÎncă nu există evaluări
- Influvac: New Zealand Data SheetDocument7 paginiInfluvac: New Zealand Data SheetAtthapu ThirupathaiahÎncă nu există evaluări
- Guidelines For Sinovac Vaccine - 6303Document6 paginiGuidelines For Sinovac Vaccine - 6303Wpress PressÎncă nu există evaluări
- The VaccinesDocument39 paginiThe Vaccinespaul arvie violetaÎncă nu există evaluări
- Summary of Product Characteristics: Composition Per Dose (0.5 ML) : Component I ContainsDocument9 paginiSummary of Product Characteristics: Composition Per Dose (0.5 ML) : Component I ContainsGayathiri GovindarajuÎncă nu există evaluări
- Guidelines For Sinovac Vaccine - 6304Document6 paginiGuidelines For Sinovac Vaccine - 6304Ali AsgharÎncă nu există evaluări
- Compilation Of Patie…: Установите Google Документы!Document1 paginăCompilation Of Patie…: Установите Google Документы!UpsetÎncă nu există evaluări
- Tetraxim APIDocument2 paginiTetraxim APIFinesse ClassesÎncă nu există evaluări
- Expanded Immunization Report 1Document54 paginiExpanded Immunization Report 1RIK HAROLD GATPANDAN100% (1)
- TetanusDocument2 paginiTetanusmegreen GamingÎncă nu există evaluări
- Miscellaneous DrugsDocument103 paginiMiscellaneous DrugsmidhunÎncă nu există evaluări
- ACC Qdenga SMPCDocument18 paginiACC Qdenga SMPCAngsamerahÎncă nu există evaluări
- COVID-19 MRNA Vaccine MRNA-1273 ModernaDocument4 paginiCOVID-19 MRNA Vaccine MRNA-1273 ModernawalkrogÎncă nu există evaluări
- COVID-19 Vaccine AstraZeneca ExplainerDocument6 paginiCOVID-19 Vaccine AstraZeneca ExplainerBakÎncă nu există evaluări
- Human Papillomavirus Bivalent Vaccin1Document8 paginiHuman Papillomavirus Bivalent Vaccin1alejandro fernandezÎncă nu există evaluări
- DexamethasoneDocument4 paginiDexamethasoneMits Valencia Karlsson0% (2)
- CPG On Immunization For WomenDocument28 paginiCPG On Immunization For WomenYnoli DiosomitoÎncă nu există evaluări
- Guidelines and Standard Operating Procedures (Sops) Sinovac Vaccine (Coronavac)Document6 paginiGuidelines and Standard Operating Procedures (Sops) Sinovac Vaccine (Coronavac)Rico MaligayaÎncă nu există evaluări
- Uk Recipients Covid 19 Vaccine Astrazeneca Reg174 Proposed 14 April 2021Document7 paginiUk Recipients Covid 19 Vaccine Astrazeneca Reg174 Proposed 14 April 2021SelenaÎncă nu există evaluări
- Health Advice and Immunizations for TravelersDe la EverandHealth Advice and Immunizations for TravelersÎncă nu există evaluări
- Ministry of Health Price List For Ambulatory and Hospitalization ServicesDocument49 paginiMinistry of Health Price List For Ambulatory and Hospitalization ServicesHåíthãm KhãtïßÎncă nu există evaluări
- Ministry of Health Price List For Ambulatory and Hospitalization ServicesDocument40 paginiMinistry of Health Price List For Ambulatory and Hospitalization ServicesHåíthãm KhãtïßÎncă nu există evaluări
- Surgery 3 White Part 1Document87 paginiSurgery 3 White Part 1Håíthãm KhãtïßÎncă nu există evaluări
- Surgery 1 PDFDocument183 paginiSurgery 1 PDFHåíthãm KhãtïßÎncă nu există evaluări
- Zarif Qaraqra English Section, Seria A, 6 Group 1, 2020 - 2021Document3 paginiZarif Qaraqra English Section, Seria A, 6 Group 1, 2020 - 2021Håíthãm KhãtïßÎncă nu există evaluări
- YY תרגול כיתתי- גדילה, תזונה ומטבוליזם PDFDocument125 paginiYY תרגול כיתתי- גדילה, תזונה ומטבוליזם PDFHåíthãm KhãtïßÎncă nu există evaluări
- Surgery 2 PDFDocument176 paginiSurgery 2 PDFHåíthãm KhãtïßÎncă nu există evaluări
- 3 Tier Drug List: CaliforniaDocument154 pagini3 Tier Drug List: CaliforniaHåíthãm KhãtïßÎncă nu există evaluări
- Abc of Drug 1Document130 paginiAbc of Drug 1Håíthãm KhãtïßÎncă nu există evaluări
- Goal:: Practical Activity in Clinic (Oncalls)Document60 paginiGoal:: Practical Activity in Clinic (Oncalls)Håíthãm KhãtïßÎncă nu există evaluări
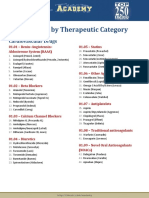
- Drug List by Therapeutic Category: Cardiovascular DrugsDocument7 paginiDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346Încă nu există evaluări
- Neisseria Genus EnglDocument127 paginiNeisseria Genus EnglHåíthãm KhãtïßÎncă nu există evaluări
- Hepatitis B Vaccine: Dosage Forms & StrengthsDocument3 paginiHepatitis B Vaccine: Dosage Forms & StrengthsHåíthãm KhãtïßÎncă nu există evaluări
- Curs Epitelii EnglezaDocument50 paginiCurs Epitelii EnglezaHåíthãm KhãtïßÎncă nu există evaluări
- 5 DR Farhat MoazamDocument9 pagini5 DR Farhat MoazamHåíthãm KhãtïßÎncă nu există evaluări
- Genetic DiseasesDocument43 paginiGenetic DiseasesAisha BirdÎncă nu există evaluări
- Curs 3 Lecture Nutrition and Bacteria CultivationDocument74 paginiCurs 3 Lecture Nutrition and Bacteria CultivationHåíthãm KhãtïßÎncă nu există evaluări
- Connective Tissue HistologyDocument12 paginiConnective Tissue HistologyHåíthãm KhãtïßÎncă nu există evaluări
- Breast CancerDocument53 paginiBreast Cancersmbala100% (1)
- Corynebacterium Listeria EnlgDocument97 paginiCorynebacterium Listeria EnlgHåíthãm KhãtïßÎncă nu există evaluări
- Immune System Has Two Lines of Defense:: A. Innate (Non Specific) ImmunityDocument105 paginiImmune System Has Two Lines of Defense:: A. Innate (Non Specific) ImmunityHåíthãm KhãtïßÎncă nu există evaluări
- Genetic DiseasesDocument43 paginiGenetic DiseasesAisha BirdÎncă nu există evaluări
- Breast Slide DeckDocument34 paginiBreast Slide DeckJane ViÎncă nu există evaluări
- Goal:: Practical Activity in Clinic (Oncalls)Document60 paginiGoal:: Practical Activity in Clinic (Oncalls)Håíthãm KhãtïßÎncă nu există evaluări
- Curs 1 - 2 EnglDocument213 paginiCurs 1 - 2 EnglHåíthãm KhãtïßÎncă nu există evaluări
- Automated External Defibrillation - A0Document1 paginăAutomated External Defibrillation - A0Håíthãm KhãtïßÎncă nu există evaluări
- VaksinasiDocument54 paginiVaksinasinikeÎncă nu există evaluări
- Abiliti 2Document68 paginiAbiliti 2Håíthãm KhãtïßÎncă nu există evaluări
- Breast CancerDocument52 paginiBreast CancerazharyekaputraÎncă nu există evaluări
- Neonatal Sepsis 2020, BMJDocument4 paginiNeonatal Sepsis 2020, BMJlaura gomezÎncă nu există evaluări
- CDT Aditya Dhala. Od-19-Sd-A-304-325. The Role of NCC in Covid-19Document3 paginiCDT Aditya Dhala. Od-19-Sd-A-304-325. The Role of NCC in Covid-19Ē Vì LÎncă nu există evaluări
- Q A 1Document48 paginiQ A 1ChannelGÎncă nu există evaluări
- Iaso Tea IngredientDocument7 paginiIaso Tea Ingredientsizzla7Încă nu există evaluări
- Espiratory System AutopsyDocument80 paginiEspiratory System AutopsyAbu ArshadÎncă nu există evaluări
- FresofolDocument4 paginiFresofolvedorangeliaÎncă nu există evaluări
- Final TouchDocument49 paginiFinal TouchmalathiÎncă nu există evaluări
- Diagnosa Non SpesialistikDocument23 paginiDiagnosa Non SpesialistikAziz FandoliÎncă nu există evaluări
- The 4th Dimension of FitnessDocument6 paginiThe 4th Dimension of FitnessalmaformaÎncă nu există evaluări
- Formulario UtepsaDocument120 paginiFormulario UtepsaAldo JoaquinÎncă nu există evaluări
- Report 1 - History of Medical TechnologyDocument1 paginăReport 1 - History of Medical TechnologyMaxine TaeyeonÎncă nu există evaluări
- Dozois 5e Chapter01 TIFDocument32 paginiDozois 5e Chapter01 TIFrebeccaÎncă nu există evaluări
- August 20, 2019Document2 paginiAugust 20, 2019Clarissa TaytayonÎncă nu există evaluări
- Introduction To Clinical ExaminationDocument153 paginiIntroduction To Clinical ExaminationBnB UsmleÎncă nu există evaluări
- Itroduction To Crim - FinalDocument27 paginiItroduction To Crim - Finalayanokouji050Încă nu există evaluări
- Diagnosing and Managing Tubercular MeningitisDocument23 paginiDiagnosing and Managing Tubercular MeningitisAstie NomleniÎncă nu există evaluări
- Pathophysiology of Myocardial InfarctionDocument4 paginiPathophysiology of Myocardial InfarctionYhr YhÎncă nu există evaluări
- Emergency Room Drug ListDocument28 paginiEmergency Room Drug Listiscariot02Încă nu există evaluări
- Construction Ergonomics KneesDocument2 paginiConstruction Ergonomics KneesZeeshan BajwaÎncă nu există evaluări
- Neral PractitionersDocument216 paginiNeral PractitionersSudhir Tyagi100% (1)
- Blood Transfusion ConsentDocument2 paginiBlood Transfusion ConsentShejil BalakrishnanÎncă nu există evaluări
- Esophageal CancerDocument42 paginiEsophageal Cancerapi-1964133750% (2)
- SCE GeriatricsDocument434 paginiSCE GeriatricsFaris FirasÎncă nu există evaluări
- Complete Health HistoryDocument22 paginiComplete Health HistorykhalidÎncă nu există evaluări
- Risk Managemnt ReviewerDocument4 paginiRisk Managemnt ReviewerHaru CutieÎncă nu există evaluări