S-ar putea să vă placă și
- Community-Acquired Pneumonia: Strategies for ManagementDe la EverandCommunity-Acquired Pneumonia: Strategies for ManagementAntoni TorresEvaluare: 4.5 din 5 stele4.5/5 (2)
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesDe la EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodÎncă nu există evaluări
- Light Pulmo Cap Hcap DR LeeDocument12 paginiLight Pulmo Cap Hcap DR LeeMiguel Cuevas DolotÎncă nu există evaluări
- LIGHT Bronchiectasis Dr. ConstantinoDocument5 paginiLIGHT Bronchiectasis Dr. ConstantinoMiguel Cuevas DolotÎncă nu există evaluări
- LIGHT Pulmo Ventilation Sleep Apnea DR ConstantinoDocument6 paginiLIGHT Pulmo Ventilation Sleep Apnea DR ConstantinoMiguel Cuevas DolotÎncă nu există evaluări
- IM - CAP High Risk Concept MapDocument1 paginăIM - CAP High Risk Concept MapTrisÎncă nu există evaluări
- Laboratory Examinations: Allen's Test Normal Finding: Hand Quickly BecomesDocument9 paginiLaboratory Examinations: Allen's Test Normal Finding: Hand Quickly BecomesShane GumaponÎncă nu există evaluări
- IM-Module B Summarized Notes (IBD)Document69 paginiIM-Module B Summarized Notes (IBD)DeepbluexÎncă nu există evaluări
- RT 220 B C AirwaystudyguideDocument25 paginiRT 220 B C Airwaystudyguiderpebdani0% (2)
- Registry Examination For Advanced Respiratory Therapists (RRT)Document6 paginiRegistry Examination For Advanced Respiratory Therapists (RRT)Sandy HartmanÎncă nu există evaluări
- ' PDFDocument1 pagină' PDFmp1757Încă nu există evaluări
- Asthma CopdDocument10 paginiAsthma CopdRem AlfelorÎncă nu există evaluări
- Breathing and Exchange of GasesDocument5 paginiBreathing and Exchange of Gaseslpc4944Încă nu există evaluări
- Pulmonary Function TestDocument77 paginiPulmonary Function TestMohammed Saad NabhanÎncă nu există evaluări
- ARDSDocument27 paginiARDSChloie Marie RosalejosÎncă nu există evaluări
- Hemoptysis 1Document27 paginiHemoptysis 1Aida SiregarÎncă nu există evaluări
- Exam 2 Study Guide 2018Document21 paginiExam 2 Study Guide 2018EvanÎncă nu există evaluări
- Mechanical Ventilation and Intracranial PressureDocument30 paginiMechanical Ventilation and Intracranial PressureFlavius AnghelÎncă nu există evaluări
- FMS Prospectus 2017 2021Document71 paginiFMS Prospectus 2017 2021Research Center for Health SciencesÎncă nu există evaluări
- Ventilator Associated Pneumonia (Vap)Document11 paginiVentilator Associated Pneumonia (Vap)Suresh KumarÎncă nu există evaluări
- Tuberculosis: Communicable DiseaseDocument6 paginiTuberculosis: Communicable DiseaseMiguel Cuevas DolotÎncă nu există evaluări
- Pulmo Case Simulation-TEAM Yellow-Blue - 01-04-21Document35 paginiPulmo Case Simulation-TEAM Yellow-Blue - 01-04-21Jolaine ValloÎncă nu există evaluări
- Lung Sounds: An Assessment of The Patient in Respiratory DistressDocument40 paginiLung Sounds: An Assessment of The Patient in Respiratory DistressJoseph Rodney de LeonÎncă nu există evaluări
- Pulmonary Function Test, JARA CSUDocument73 paginiPulmonary Function Test, JARA CSUJohn NicoleÎncă nu există evaluări
- Bronchiectasis NishaDocument44 paginiBronchiectasis NishaKaarthigan RamaiahÎncă nu există evaluări
- Pilbeam - Mechanical Ventilation Physiological and Clinical Applications-59-73.en - EsDocument15 paginiPilbeam - Mechanical Ventilation Physiological and Clinical Applications-59-73.en - EsAdriana MartinezÎncă nu există evaluări
- Mechvent Review (Topnotcher)Document284 paginiMechvent Review (Topnotcher)Gleo Matthew100% (1)
- Revised PCCP Spiro Consensus PDFDocument93 paginiRevised PCCP Spiro Consensus PDFJC ValenciaÎncă nu există evaluări
- Pneumonia: DefinitionDocument5 paginiPneumonia: DefinitionhemaanandhyÎncă nu există evaluări
- Empyema 2Document31 paginiEmpyema 2Michelle SalimÎncă nu există evaluări
- Respiratory Care ModalitiesDocument63 paginiRespiratory Care ModalitiesErica Clerigo LandichoÎncă nu există evaluări
- Respiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDocument12 paginiRespiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDoc JacqueÎncă nu există evaluări
- Disorders of The PleuraDocument7 paginiDisorders of The PleuraMaikka IlaganÎncă nu există evaluări
- Case Studies: Restrictive and Obstructive Respiratory Conditions Case Study # 1Document5 paginiCase Studies: Restrictive and Obstructive Respiratory Conditions Case Study # 1psyarjavierÎncă nu există evaluări
- Resp Bronch N LaDocument56 paginiResp Bronch N LaMansi GandhiÎncă nu există evaluări
- Suppurative Lung Diseases: DR Faisal Moidunny Mammu Department of PaediatricsDocument39 paginiSuppurative Lung Diseases: DR Faisal Moidunny Mammu Department of PaediatricsFaisal MoidunnyÎncă nu există evaluări
- Respiratory Failure PresentationDocument13 paginiRespiratory Failure PresentationHusnain Irshad AlviÎncă nu există evaluări
- Pulmonary Sarcoidosis Presenting With Cannonball Pattern Mimicking Lung MetastasesDocument5 paginiPulmonary Sarcoidosis Presenting With Cannonball Pattern Mimicking Lung MetastasesIJAR JOURNALÎncă nu există evaluări
- Mechanical Ventilation TherapyDocument17 paginiMechanical Ventilation TherapyFaizal FlÎncă nu există evaluări
- Asthma Lancet 23febDocument18 paginiAsthma Lancet 23febMr. LÎncă nu există evaluări
- Registered Respiratory TherapistDocument3 paginiRegistered Respiratory Therapistapi-76909521Încă nu există evaluări
- Suctioning Artificial Airways - AdultsDocument27 paginiSuctioning Artificial Airways - AdultssdaÎncă nu există evaluări
- Bronchiectasis: Prepared By: Michelle TamorDocument17 paginiBronchiectasis: Prepared By: Michelle TamorMichelle TamorÎncă nu există evaluări
- Infectious Disease MedicationsDocument8 paginiInfectious Disease MedicationsSheril MarekÎncă nu există evaluări
- Meaning of Different Types of SputumDocument10 paginiMeaning of Different Types of SputumCharlotte's WebÎncă nu există evaluări
- Case Discussion - CopdDocument63 paginiCase Discussion - CopdrajeshÎncă nu există evaluări
- Cor PulmonaleDocument8 paginiCor PulmonaleAymen OmerÎncă nu există evaluări
- Evaluation of Dyspneic PatientDocument15 paginiEvaluation of Dyspneic Patientcamila perillaÎncă nu există evaluări
- Respiratory EmergenciesDocument34 paginiRespiratory EmergenciesRoshana MallawaarachchiÎncă nu există evaluări
- Respiratory PhysiologyDocument16 paginiRespiratory PhysiologyYsabel Salvador DychincoÎncă nu există evaluări
- PEEP Positive End Expiratory Pressure and Its ConsequencesDocument2 paginiPEEP Positive End Expiratory Pressure and Its ConsequencesSadiq ZakariaÎncă nu există evaluări
- Acute Bronchiolitis EditedDocument19 paginiAcute Bronchiolitis EditedSurgicalgownÎncă nu există evaluări
- COPD Acute Management ABCDEDocument11 paginiCOPD Acute Management ABCDESSÎncă nu există evaluări
- ARDS LectureDocument58 paginiARDS LecturedrjaikrishÎncă nu există evaluări
- Lung AuscultationDocument62 paginiLung AuscultationOlea CroitorÎncă nu există evaluări
- Cpap and Bipap: "A CPAP A Day Helps Keep The ET Tube Away!"Document15 paginiCpap and Bipap: "A CPAP A Day Helps Keep The ET Tube Away!"Muhammad Tayyab MadniÎncă nu există evaluări
- Bacteria List Exam 1 PDFDocument16 paginiBacteria List Exam 1 PDFJamesHowsonÎncă nu există evaluări
- Cardiovascular Complications of Respiratory DisordersDocument334 paginiCardiovascular Complications of Respiratory DisordersDani CapiÎncă nu există evaluări
- Imaging Pulmonary Infection, Classic Sign and Pattern PRESENTASIDocument84 paginiImaging Pulmonary Infection, Classic Sign and Pattern PRESENTASIMark Brown100% (1)
- CopdDocument14 paginiCopdMohd Farid Bin RosliÎncă nu există evaluări
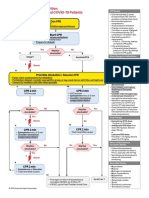
- ACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsDocument1 paginăACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsMariuxi Tatiana ChocoÎncă nu există evaluări
- Covid 19 CPR 7 RulesDocument21 paginiCovid 19 CPR 7 RulesMiguel Cuevas DolotÎncă nu există evaluări
- Effectiveness of Transdermal MagnesiumDocument2 paginiEffectiveness of Transdermal MagnesiumMiguel Cuevas Dolot100% (1)
- Covid 19 CPR 7 RulesDocument21 paginiCovid 19 CPR 7 RulesMiguel Cuevas DolotÎncă nu există evaluări
- How Can Patients Visitors Help - May18Document2 paginiHow Can Patients Visitors Help - May18Miguel Cuevas DolotÎncă nu există evaluări
- PSB 368Document6 paginiPSB 368Miguel Cuevas DolotÎncă nu există evaluări
- Covid 19 PDFDocument18 paginiCovid 19 PDFMiguel Cuevas DolotÎncă nu există evaluări
- Physical Examination in ENT: Ussana Promyothin, MDDocument60 paginiPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotÎncă nu există evaluări
- (MED) COVID-19 Trans V. 2.0Document6 pagini(MED) COVID-19 Trans V. 2.0Isabel VinasÎncă nu există evaluări
- Physical Examination in ENT: Ussana Promyothin, MDDocument60 paginiPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotÎncă nu există evaluări
- Vertigo Gail Ishiyama 1 13 10Document40 paginiVertigo Gail Ishiyama 1 13 10Myname Rama LienÎncă nu există evaluări
- Anesthesia Pocket Cards 7 18 18Document6 paginiAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotÎncă nu există evaluări
- Clinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Document30 paginiClinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Ekambaram TrmÎncă nu există evaluări
- Physical Assessment: Ear, Nose, Mouth, and ThroatDocument59 paginiPhysical Assessment: Ear, Nose, Mouth, and ThroatMiguel Cuevas DolotÎncă nu există evaluări
- Clinical AbstractDocument4 paginiClinical AbstractMiguel Cuevas DolotÎncă nu există evaluări
- Cook Book (Filipino) 13 PDFDocument23 paginiCook Book (Filipino) 13 PDFAdina AnghelÎncă nu există evaluări
- Pedia Tickler Update 2017Document2 paginiPedia Tickler Update 2017Tani BokÎncă nu există evaluări
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocument12 paginiA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotÎncă nu există evaluări
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocument12 paginiA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotÎncă nu există evaluări
- Active Listening HANDOUT PDFDocument26 paginiActive Listening HANDOUT PDFMiguel Cuevas DolotÎncă nu există evaluări
- Drug IndexDocument2 paginiDrug IndexMiguel Cuevas DolotÎncă nu există evaluări
- Neurologic ExamDocument1 paginăNeurologic ExamMiguel Cuevas DolotÎncă nu există evaluări
- HEMAreviewDocument3 paginiHEMAreviewMiguel Cuevas DolotÎncă nu există evaluări
- Benign Paroxysmal Positional Vertigo: Waseem WatadDocument37 paginiBenign Paroxysmal Positional Vertigo: Waseem WatadnoviÎncă nu există evaluări
- Nocturnals Physiology 2018Document14 paginiNocturnals Physiology 2018Miguel Cuevas DolotÎncă nu există evaluări
- History Taking ExaminationDocument7 paginiHistory Taking ExaminationIndunil AnuruddhikaÎncă nu există evaluări
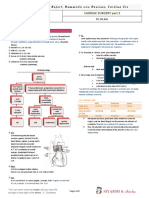
- TCVS - Cardiac Surgery Part 2 Dr. de AsisDocument8 paginiTCVS - Cardiac Surgery Part 2 Dr. de AsisMiguel Cuevas DolotÎncă nu există evaluări
- Kerosene PDFDocument31 paginiKerosene PDFRudyMLanaÎncă nu există evaluări
- Community-Acquired Pneumonia - CPG 2016Document26 paginiCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianÎncă nu există evaluări
- Jeopardy CPRDocument51 paginiJeopardy CPRapi-273870175Încă nu există evaluări
- NCP FormDocument2 paginiNCP FormFranz goÎncă nu există evaluări
- Low Back Pain in Adolescents and Association With Sociodemographic Factors, Electronic Devices, Physical Activity and Mental HealthDocument8 paginiLow Back Pain in Adolescents and Association With Sociodemographic Factors, Electronic Devices, Physical Activity and Mental HealthluaÎncă nu există evaluări
- Hepatitis B in PregnancyDocument17 paginiHepatitis B in PregnancysnazzyÎncă nu există evaluări
- Introduction To Microbial Pathogenicity: Presented byDocument11 paginiIntroduction To Microbial Pathogenicity: Presented byAy GlassesÎncă nu există evaluări
- Vasculitis SyndromesDocument56 paginiVasculitis SyndromesHengki Permana PutraÎncă nu există evaluări
- Pathogens 10 00013 v2Document25 paginiPathogens 10 00013 v2Mega KapitanÎncă nu există evaluări
- The Concept of MiasmDocument4 paginiThe Concept of MiasmRamesh ShahÎncă nu există evaluări
- How Big Is The Problem?: Incontinence in NumbersDocument14 paginiHow Big Is The Problem?: Incontinence in NumbersSumit MalhotraÎncă nu există evaluări
- Neurological Update: MOG Antibody Disease: Ray Wynford Thomas Anu Jacob Valentina TomassiniDocument7 paginiNeurological Update: MOG Antibody Disease: Ray Wynford Thomas Anu Jacob Valentina TomassiniValentina Cortes MoralesÎncă nu există evaluări
- Cerebrovascular Complications of COVID-19: Brief ReportDocument5 paginiCerebrovascular Complications of COVID-19: Brief ReportAmandaÎncă nu există evaluări
- CHN MCQ Set 3Document14 paginiCHN MCQ Set 3Neenu RajputÎncă nu există evaluări
- Fowl CholeraDocument34 paginiFowl Choleramazher aliÎncă nu există evaluări
- Outer Ear Infection (Swimmer's Ear)Document2 paginiOuter Ear Infection (Swimmer's Ear)ScraaaaÎncă nu există evaluări
- Fish ReportDocument3 paginiFish ReportjolatiÎncă nu există evaluări
- Eastern Visayas Regional Covid-19 Testing Center: Laboratory Test Request FormDocument1 paginăEastern Visayas Regional Covid-19 Testing Center: Laboratory Test Request FormLouieÎncă nu există evaluări
- Conjunctivitis Hordeolum ChalazionDocument52 paginiConjunctivitis Hordeolum ChalazionPatricia May CruzÎncă nu există evaluări
- Quick GuideDocument4 paginiQuick GuidevigurÎncă nu există evaluări
- Bacterial ConjunctivitisDocument32 paginiBacterial ConjunctivitisYouhengÎncă nu există evaluări
- History of Biostatistics: Correspondence ToDocument5 paginiHistory of Biostatistics: Correspondence ToHenrique MartinsÎncă nu există evaluări
- Perioperative Thrombocytopenia.98643Document10 paginiPerioperative Thrombocytopenia.98643Andreea MitranÎncă nu există evaluări
- Diseases of The Digestive SystemDocument5 paginiDiseases of The Digestive SystemG1N0G4M3Încă nu există evaluări
- Ricketsiae BacteriaDocument2 paginiRicketsiae BacteriaErnie G. Bautista II, RN, MDÎncă nu există evaluări
- Covid-19 - PreventionDocument1 paginăCovid-19 - PreventionKristel LavalleÎncă nu există evaluări
- Biologyinvestigatoryproject 170725165743 PDFDocument18 paginiBiologyinvestigatoryproject 170725165743 PDFrounakÎncă nu există evaluări
- Prognosis and Discharge PlanDocument6 paginiPrognosis and Discharge Planjanelee2824Încă nu există evaluări
- Causes of DepressionDocument6 paginiCauses of DepressionJeanikka DolotinaÎncă nu există evaluări
- Stewardship Booklet Practical Guide To Antimicrobial Stewardship in HospitalsDocument23 paginiStewardship Booklet Practical Guide To Antimicrobial Stewardship in HospitalsZunisa Rizki100% (4)
- Biology Project File Alzheimer: Akshita AgrawalDocument15 paginiBiology Project File Alzheimer: Akshita AgrawalAkshita100% (1)
- Best Exam Preparation Tips Marlene Pearce PDFDocument32 paginiBest Exam Preparation Tips Marlene Pearce PDFZH. omg sarÎncă nu există evaluări