S-ar putea să vă placă și
- Online Hospital Management SystemDocument2 paginiOnline Hospital Management Systemyay guruÎncă nu există evaluări
- Open Source Hospital Management Information SystemDocument14 paginiOpen Source Hospital Management Information SystemMorapitiya Hewa Buddhika AriyaratneÎncă nu există evaluări
- Hospital Management System: Labaid by Simon (BUBT)Document28 paginiHospital Management System: Labaid by Simon (BUBT)Simon HaqueÎncă nu există evaluări
- Order Management A Complete Guide - 2021 EditionDe la EverandOrder Management A Complete Guide - 2021 EditionÎncă nu există evaluări
- DD 3600 3500 3000 Parts CatalogDocument46 paginiDD 3600 3500 3000 Parts CatalogAndres Fdo Mora D100% (2)
- Best Practices in Selecting A Contracted Regulated Medical Waste Disposal ProviderDocument12 paginiBest Practices in Selecting A Contracted Regulated Medical Waste Disposal ProviderStericycleÎncă nu există evaluări
- Dental Accreditation StandardsDocument66 paginiDental Accreditation Standardsdhir.ankurÎncă nu există evaluări
- 9241561998Document280 pagini9241561998Varun Mohanakumaran RajambikaÎncă nu există evaluări
- Marketing Dept QuestionnaireDocument2 paginiMarketing Dept QuestionnaireSrinivas PolikepatiÎncă nu există evaluări
- Pharma Supply Chain For Domestic DistributionDocument4 paginiPharma Supply Chain For Domestic DistributiondineshnutiÎncă nu există evaluări
- District Hospital Report For Digital PublicationDocument234 paginiDistrict Hospital Report For Digital Publicationjayanth.raghavan4441Încă nu există evaluări
- Medical Development PowerPoint TemplateDocument16 paginiMedical Development PowerPoint TemplatesugamÎncă nu există evaluări
- Policies & Procedures For Assessment, Surveillance and Re-Assessment of HcoDocument16 paginiPolicies & Procedures For Assessment, Surveillance and Re-Assessment of HcoSubiVictorÎncă nu există evaluări
- HMIS Project Report PDFDocument25 paginiHMIS Project Report PDFAther100% (1)
- Hospital Management System Software in Quanta HisDocument31 paginiHospital Management System Software in Quanta HisBirlamedisoftÎncă nu există evaluări
- An Overview To Healthcare OperationsDocument24 paginiAn Overview To Healthcare OperationsQuality Saket100% (1)
- Quantification of Health Commodities 2017 PDFDocument88 paginiQuantification of Health Commodities 2017 PDFLalaÎncă nu există evaluări
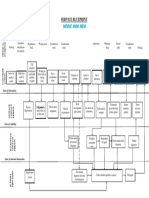
- Service Blueprint Medical CenterDocument1 paginăService Blueprint Medical CenterNguyen Le Hoang KimÎncă nu există evaluări
- On WHO Standards and RecommendationsDocument62 paginiOn WHO Standards and Recommendationspoonam@ims0% (1)
- Advantech Digital Healthcare Catalog-2010Document11 paginiAdvantech Digital Healthcare Catalog-2010László NémethÎncă nu există evaluări
- Financial Management PDFDocument132 paginiFinancial Management PDFsumit mishraÎncă nu există evaluări
- PURCHASE - MANAGEMENT - IN - HOSPITALS MirageDocument20 paginiPURCHASE - MANAGEMENT - IN - HOSPITALS MirageDoc Sandy100% (1)
- APIC RSM Auditing - 201802 PDFDocument23 paginiAPIC RSM Auditing - 201802 PDFAl RammohanÎncă nu există evaluări
- Project On Hospital ManagementDocument21 paginiProject On Hospital ManagementAshishNamdeoÎncă nu există evaluări
- Quality Management in HealthcareDocument7 paginiQuality Management in Healthcareselinasimpson0101Încă nu există evaluări
- ISBM PROJECT FinalDocument23 paginiISBM PROJECT Finalkunal NeelayÎncă nu există evaluări
- Uml Patient Information SystemDocument5 paginiUml Patient Information SystemSathyaPriya RamasamyÎncă nu există evaluări
- System Administrator at Our Organization, Based in HyderabadDocument3 paginiSystem Administrator at Our Organization, Based in Hyderabadyogesh chowdary100% (1)
- 8 Nasscom-Eri-Rpa Market Opportunity - NasscomDocument61 pagini8 Nasscom-Eri-Rpa Market Opportunity - Nasscomnoestoypanadie2000Încă nu există evaluări
- SRS On Hospital ManagementDocument21 paginiSRS On Hospital ManagementDevKumar MahatoÎncă nu există evaluări
- From A MILLION HITS To A Webby Honoree BackgroundDocument4 paginiFrom A MILLION HITS To A Webby Honoree BackgroundTanmoy ChakrabortyÎncă nu există evaluări
- ABDM - ApprovalDocument23 paginiABDM - ApprovalNavya BhandaruÎncă nu există evaluări
- Internal Communication AuditDocument33 paginiInternal Communication AuditAtish GoolaupÎncă nu există evaluări
- Advence Hospital Management System PDFDocument6 paginiAdvence Hospital Management System PDFMd Nazmul IslamÎncă nu există evaluări
- Hospital Information System High Level Work Flow Diagram & Modules DescriptionDocument17 paginiHospital Information System High Level Work Flow Diagram & Modules DescriptionkarimmamunÎncă nu există evaluări
- Enterprise Resource PlanningDocument9 paginiEnterprise Resource PlanningRobbin HaidenÎncă nu există evaluări
- The New Trends of Drug R&D Outsourcing in China and IndiaDocument20 paginiThe New Trends of Drug R&D Outsourcing in China and Indiajz9826Încă nu există evaluări
- 3Q14 Roadmap To ValuationDocument30 pagini3Q14 Roadmap To ValuationRyan BrookmanÎncă nu există evaluări
- Wearable, Implantable, and Interventional Medical DevicesDocument18 paginiWearable, Implantable, and Interventional Medical DevicesMysha RahmanÎncă nu există evaluări
- Dispute System ProposalDocument21 paginiDispute System ProposalM. A. HaqueÎncă nu există evaluări
- Ehr Chapter 1 CarterDocument17 paginiEhr Chapter 1 Carterapi-298340093Încă nu există evaluări
- Guidebook - Entry LevelDocument42 paginiGuidebook - Entry Levelrahul8390Încă nu există evaluări
- Adeeba Balance Smu Project SampleDocument81 paginiAdeeba Balance Smu Project SampleDEEPAKÎncă nu există evaluări
- PortfolioDocument15 paginiPortfolioKanak YadavÎncă nu există evaluări
- Electronic Logistics Management Information System (eLMIS) Supplementary in PDFDocument19 paginiElectronic Logistics Management Information System (eLMIS) Supplementary in PDFNaveen KaranÎncă nu există evaluări
- 2015 Health Care Providers Outlook: United StatesDocument5 pagini2015 Health Care Providers Outlook: United StatesEmma Hinchliffe100% (1)
- Internal TCS Infosys, WiproDocument14 paginiInternal TCS Infosys, WiproAnesh SthapitÎncă nu există evaluări
- Developing Operational Review Programmes For Managerial and Audit UseDocument38 paginiDeveloping Operational Review Programmes For Managerial and Audit UseRoxanne CerioÎncă nu există evaluări
- Medical Appointment Application: Acta Electronica Malaysia (AEM)Document5 paginiMedical Appointment Application: Acta Electronica Malaysia (AEM)Akansha SinghÎncă nu există evaluări
- Gantt ChartDocument19 paginiGantt ChartShahzaib AsifÎncă nu există evaluări
- Selection Checklist: Erp SoftwareDocument14 paginiSelection Checklist: Erp Softwareindhumathi boobalanÎncă nu există evaluări
- Human Resouce ManagementDocument5 paginiHuman Resouce ManagementnashÎncă nu există evaluări
- S.I.W.S. College OF Management StudiesDocument45 paginiS.I.W.S. College OF Management Studiesaquarianmansi2212100% (1)
- Process MapDocument7 paginiProcess Mapapi-535002543100% (1)
- Apollo Hospitals: Towards Touching A ..Billion LivesDocument22 paginiApollo Hospitals: Towards Touching A ..Billion LivesAtyukti PachauriÎncă nu există evaluări
- Project Reports For Start Up BusinessDocument17 paginiProject Reports For Start Up BusinessraviÎncă nu există evaluări
- Hospital Scorecard - DepartmentwiseDocument4 paginiHospital Scorecard - DepartmentwiseNatasha BhasinÎncă nu există evaluări
- Performance Metrics of RI D3780 RY 2017-18 To 2019-20Document9 paginiPerformance Metrics of RI D3780 RY 2017-18 To 2019-20rc_holyspiritÎncă nu există evaluări
- Synopsis On Patient Safety in OPDDocument6 paginiSynopsis On Patient Safety in OPDniceprachiÎncă nu există evaluări
- A Quick Guide On How To Achieve Gold / Silver Quality CertificateDocument101 paginiA Quick Guide On How To Achieve Gold / Silver Quality CertificateAnonymous 4WAq7tlÎncă nu există evaluări
- Guideline For How To Achieve Bronze Quality Certificate 2 in 1Document130 paginiGuideline For How To Achieve Bronze Quality Certificate 2 in 1Anonymous 4WAq7tlÎncă nu există evaluări
- Bronze Quality Certificate Standards - FinalDocument40 paginiBronze Quality Certificate Standards - FinalAnonymous 4WAq7tlÎncă nu există evaluări
- Guideline For Self-Assessment Quality - ChecklistDocument72 paginiGuideline For Self-Assessment Quality - ChecklistAnonymous 4WAq7tlÎncă nu există evaluări
- Van Daley - Leadership ResumeDocument1 paginăVan Daley - Leadership Resumeapi-352146181Încă nu există evaluări
- Arrhythmia - WikipediaDocument76 paginiArrhythmia - WikipediaJamesÎncă nu există evaluări
- Luyện nghe Tiếng Anh có đáp án: I/ Listen and complete the textDocument3 paginiLuyện nghe Tiếng Anh có đáp án: I/ Listen and complete the textVN LenaÎncă nu există evaluări
- Letter of Intent Date: 18-Feb-2019 Mr. Ravi Mishra,: For Multiplier Brand Solutions PVT LTDDocument2 paginiLetter of Intent Date: 18-Feb-2019 Mr. Ravi Mishra,: For Multiplier Brand Solutions PVT LTDRavi MishraÎncă nu există evaluări
- Quizlet Table 7Document1 paginăQuizlet Table 7JosielynÎncă nu există evaluări
- Why Do Kashmiris Need Self-Determination?: UncategorizedDocument16 paginiWhy Do Kashmiris Need Self-Determination?: UncategorizedFarooq SiddiqiÎncă nu există evaluări
- Audit Committee and Corporate Governance: CA Pragnesh Kanabar Sir's The Audit Academy-CA Final AuditDocument17 paginiAudit Committee and Corporate Governance: CA Pragnesh Kanabar Sir's The Audit Academy-CA Final AuditPULKIT MURARKAÎncă nu există evaluări
- p1632 eDocument4 paginip1632 ejohn saenzÎncă nu există evaluări
- Tema & Htri by Bert BoxmaDocument5 paginiTema & Htri by Bert Boxmabloodterry2284Încă nu există evaluări
- IPT .Quarter 2 (Grade 7-Mathematics, English &TLE)Document2 paginiIPT .Quarter 2 (Grade 7-Mathematics, English &TLE)ARRIANE JOY TOLEDOÎncă nu există evaluări
- NUFLO Low Power Pre-Amplifier: SpecificationsDocument2 paginiNUFLO Low Power Pre-Amplifier: SpecificationsJorge ParraÎncă nu există evaluări
- THE Ketofeed Diet Book v2Document43 paginiTHE Ketofeed Diet Book v2jacosta12100% (1)
- Writing Short StoriesDocument10 paginiWriting Short StoriesRodiatun YooÎncă nu există evaluări
- L15 PDFDocument15 paginiL15 PDFlesÎncă nu există evaluări
- Sharp Product-Catalogue 2019 enDocument48 paginiSharp Product-Catalogue 2019 enMiki di KaprioÎncă nu există evaluări
- Panel Hospital List IGIDocument6 paginiPanel Hospital List IGIAbdul RahmanÎncă nu există evaluări
- Teccrs 3800Document431 paginiTeccrs 3800Genus SumÎncă nu există evaluări
- Family History Timeline Rubric HonorsDocument1 paginăFamily History Timeline Rubric Honorsapi-291510568Încă nu există evaluări
- Thom22e ch03 FinalDocument44 paginiThom22e ch03 FinalDionisius AlvianÎncă nu există evaluări
- WHITE TOWN GROUP-4 FinalDocument112 paginiWHITE TOWN GROUP-4 Finalaswath manojÎncă nu există evaluări
- Loan Agreement: Acceleration ClauseDocument2 paginiLoan Agreement: Acceleration ClauseSomething SuspiciousÎncă nu există evaluări
- Engineering Mathematics Questions and AnswersDocument9 paginiEngineering Mathematics Questions and AnswersZaky Muzaffar100% (1)
- Biography of Anna HazareDocument4 paginiBiography of Anna HazareGenesis FirstÎncă nu există evaluări
- Lesson Plan Wid Awt Method 2Document7 paginiLesson Plan Wid Awt Method 2Yan LianÎncă nu există evaluări
- Cell Structure, Cellular Respiration, PhotosynthesisDocument14 paginiCell Structure, Cellular Respiration, PhotosynthesisAmr NasserÎncă nu există evaluări
- I - Pronunciation Choose The Word Whose Stress Pattern Is Different From The Other Three in The Following QuestionsDocument6 paginiI - Pronunciation Choose The Word Whose Stress Pattern Is Different From The Other Three in The Following QuestionsHaÎncă nu există evaluări
- Probecom 11.3M Antenna System Datasheet 2Document2 paginiProbecom 11.3M Antenna System Datasheet 2Hugo MateoÎncă nu există evaluări
- COSO DefinEDDocument21 paginiCOSO DefinEDRefdy AnugrahÎncă nu există evaluări
- Esp8285 Datasheet enDocument29 paginiEsp8285 Datasheet enJohn GreenÎncă nu există evaluări