S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- GUIDELINES ON SURGICAL MANAGEMENT OF SUSPECTED OR CONFIRMED COVID-19 Annex 22Document10 paginiGUIDELINES ON SURGICAL MANAGEMENT OF SUSPECTED OR CONFIRMED COVID-19 Annex 22nurul fatma diyanaÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Garis Panduan Audit Dokumentasi Klinikal Dan Kod KlasifikasiDocument33 paginiGaris Panduan Audit Dokumentasi Klinikal Dan Kod Klasifikasinurul fatma diyanaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- InfluenzaDocument24 paginiInfluenzanurul fatma diyanaÎncă nu există evaluări
- Improving Outpatient Clinic Operations: An Exploratory Case StudyDocument6 paginiImproving Outpatient Clinic Operations: An Exploratory Case Studynurul fatma diyanaÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Ahmad, Nurul Fatma - Referral SystemDocument30 paginiAhmad, Nurul Fatma - Referral Systemnurul fatma diyanaÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- National Ehealth: "Moving Towards Efficient Healthcare"Document30 paginiNational Ehealth: "Moving Towards Efficient Healthcare"nurul fatma diyanaÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
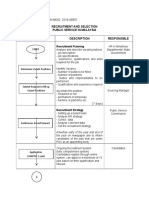
- Recruitment and Selection Public Service in Malaysia Activity Flow Description ResponsibleDocument4 paginiRecruitment and Selection Public Service in Malaysia Activity Flow Description Responsiblenurul fatma diyanaÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Security Director Emergency Manager Ridgewood NJ Resume John MorganDocument3 paginiSecurity Director Emergency Manager Ridgewood NJ Resume John MorganJohnMorgan100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Article Therapeutic CommunicationDocument12 paginiArticle Therapeutic CommunicationYolfi RuindunganÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- BSN 3 4 Group 7 Final ManuscriptDocument64 paginiBSN 3 4 Group 7 Final ManuscriptGave gonzalesÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hospital Design GuideDocument6 paginiHospital Design Guidemdeenk0% (2)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Take One Nursing FC PalmrDocument31 paginiTake One Nursing FC Palmrnot your medz duran100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- AccreditationDocument4 paginiAccreditationis_aradanasÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- CT Quickstart Installation Guide: Working Together To Get Your New Technology Online and Begin Providing Patient CareDocument56 paginiCT Quickstart Installation Guide: Working Together To Get Your New Technology Online and Begin Providing Patient CareJenson ManiÎncă nu există evaluări
- Daftar Pustaka SnarsDocument18 paginiDaftar Pustaka SnarsDesy MulyanaÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- JCI AccreditationDocument16 paginiJCI Accreditationjoshua_sx1100% (3)
- Ommaya Reservoir Drug InfusionDocument19 paginiOmmaya Reservoir Drug InfusionDiah Rahayu SetiawatiÎncă nu există evaluări
- Clinical Decision Support SystemsDocument19 paginiClinical Decision Support SystemsMohammad Hamid100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Sample Competency Assessment ToolDocument10 paginiSample Competency Assessment ToolHengkyÎncă nu există evaluări
- @@assessment of Medical Documentation As Per Joint Commission InternationDocument6 pagini@@assessment of Medical Documentation As Per Joint Commission InternationNahari ArifinÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- What Are OPPE and FPPE?Document1 paginăWhat Are OPPE and FPPE?adyÎncă nu există evaluări
- Test Bank For Clinical Nursing Skills 9th Edition by SmithDocument16 paginiTest Bank For Clinical Nursing Skills 9th Edition by SmithJavier Edwards100% (26)
- Cruelty Towards Animals EssayDocument8 paginiCruelty Towards Animals Essayfz75nk7v100% (2)
- Pain Management Practices by Nurses An ApplicationDocument8 paginiPain Management Practices by Nurses An ApplicationNoraÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Pharmacy PracticeDocument72 paginiPharmacy PracticehanasheedhÎncă nu există evaluări
- Draft Guidelines For PMSSY Scheme For EmployeDocument14 paginiDraft Guidelines For PMSSY Scheme For EmployeAbhishek YadavÎncă nu există evaluări
- Week 4 Health Care Facility DesignDocument11 paginiWeek 4 Health Care Facility DesignJessy WairiaÎncă nu există evaluări
- Prevention of Surgical Site Infections: Surgical Patient Care SeriesDocument11 paginiPrevention of Surgical Site Infections: Surgical Patient Care Seriestien duongÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Director of Patient Care Services or Nurse SupervisorDocument2 paginiDirector of Patient Care Services or Nurse Supervisorapi-77594952Încă nu există evaluări
- Jani-King Commercial Cleaning Healthcare ServicesDocument59 paginiJani-King Commercial Cleaning Healthcare ServicesAlejandro SanchezÎncă nu există evaluări
- Mouwasat EDocument138 paginiMouwasat EAnis ThakurÎncă nu există evaluări
- A Guide To The Joint Commission - SDocument8 paginiA Guide To The Joint Commission - Sn100% (1)
- Lab Statistics Fun and Easy Fifth EditionDocument204 paginiLab Statistics Fun and Easy Fifth EditionJosé González CamposÎncă nu există evaluări
- Test Bank For Healthcare Human Resource Management 3rd EditionDocument7 paginiTest Bank For Healthcare Human Resource Management 3rd EditionMarta Tronaas100% (32)
- IV Catheter Insertion PDFDocument17 paginiIV Catheter Insertion PDFHannaÎncă nu există evaluări
- Prevention and Control of InfectionsDocument21 paginiPrevention and Control of InfectionsSunil ThomasÎncă nu există evaluări
- Introduction To Health EducationDocument7 paginiIntroduction To Health EducationUnknown100% (2)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)