Documente Academic
Documente Profesional
Documente Cultură
Child Survival Gain in Tanzania
Încărcat de
Alfred MkingaDescriere originală:
Drepturi de autor
Formate disponibile
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentDrepturi de autor:
Formate disponibile
Child Survival Gain in Tanzania
Încărcat de
Alfred MkingaDrepturi de autor:
Formate disponibile
Articles
EMBARGO: 00:01H (UK time) Friday April 11, 2008. In North America the embargo lifts at
18:30 (EDT) Thursday April 10, 2008
Child survival gains in Tanzania: analysis of data from
demographic and health surveys
Honorati Masanja, Don de Savigny, Paul Smithson, Joanna Schellenberg, Theopista John, Conrad Mbuya, Gabriel Upunda, Ties Boerma,
Cesar Victora, Tom Smith, Hassan Mshinda
Summary
Lancet 2008; 371: 1276–83 Background A recent national survey in Tanzania reported that mortality in children younger than 5 years dropped
Ifakara Health Research and by 24% over the 5 years between 2000 and 2004. We aimed to investigate yearly changes to identify what might have
Development Centre, Ifakara, contributed to this reduction and to investigate the prospects for meeting the Millennium Development Goal for child
Tanzania (H Masanja PhD,
survival (MDG 4).
Prof D de Savigny PhD,
P Smithson MPH,
J Schellenberg PhD, Methods We analysed data from the four demographic and health surveys done in Tanzania since 1990 to generate
H Mshinda PhD); Swiss Tropical estimates of mortality in children younger than 5 years for every 1-year period before each survey back to 1990. We
Institute, Basel, Switzerland
estimated trends in mortality between 1990 and 2004 by fitting Lowess regression, and forecasted trends in mortality
(D de Savigny, Prof T Smith PhD);
London School of Hygiene and in 2005 to 2015. We aimed to investigate contextual factors, whether part of Tanzania’s health system or not, that
Tropical Medicine, London, UK could have affected child mortality.
(J Schellenberg); World Health
Organization, Dar es Salaam,
Tanzania (T John MSc); Ministry
Findings Disaggregated estimates of mortality showed a sharp acceleration in the reduction in mortality in children
of Health and Social Welfare, younger than 5 years in Tanzania between 2000 and 2004. In 1990, the point estimate of mortality was 141·5 (95% CI
Dar es Salaam, Tanzania 141·5–141·5) deaths per 1000 livebirths. This was reduced by 40%, to reach a point estimate of 83·2 (95% CI
(C Mbuya MPH, G Upunda MPH); 70·1–96·3) deaths per 1000 livebirths in 2004. The change in absolute risk was 58·4 (95% CI 32·7–83·8; p<0·0001).
World Health Organization,
Geneva, Switzerland
Between 1999 and 2004 we noted important improvements in Tanzania’s health system, including doubled public
(T Boerma PhD); and University expenditure on health; decentralisation and sector-wide basket funding; and increased coverage of key child-survival
of Pelotas, Pelotas, Brazil interventions, such as integrated management of childhood illness, insecticide-treated nets, vitamin A supplementation,
(Prof C Victora PhD) immunisation, and exclusive breastfeeding. Other determinants of child survival that are not related to the health
Correspondence to: system did not change between 1999 and 2004, except for a slow increase in the HIV/AIDS burden.
Honorati Masanja, Ifakara Health
Research and Development
Centre, Kiko Avenue, Plot N 463, Interpretation Tanzania could attain MDG 4 if this trend of improved child survival were to be sustained. Investment
Mikocheni, Dar es Salaam, in health systems and scaling up interventions can produce rapid gains in child survival.
Tanzania
hmasanja@ihrdc.or.tz
Funding Government of Norway.
Introduction birth-history surveys to obtain direct retrospective
The Millennium Development Goal (MDG 4) to reduce estimates of child mortality.11 Such national surveys are
mortality in children younger than 5 years by two-thirds done every 4–5 years and generally include measures of
between 1990 and 2015 has come into focus in recent coverage for priority child-health interventions.12 The
years as a galvanising force to align global and national surveys are standardised by national bureaux of statistics
efforts towards poverty reduction and better health.1–4 such as demographic and health surveys (DHS), which
Much of the current burden of mortality in children are sponsored by USAID, and multiple indicator cluster
younger than 5 years in low-income countries is surveys, which are sponsored by UNICEF. More than
preventable if effective coverage of available cost-effective 40 national mortality surveys from the 60 priority
interventions can be achieved.5 However, global countries will be available in 2005–07,12 one of the first of
assessments of the 60 priority countries where most which is from Tanzania.
children younger than 5 years die show that very few are In 1990, mortality in children younger than 5 years in
on track to reach MDG 4.1,6 Many of these countries are in Tanzania was 141 per 1000 livebirths; thus, Tanzania’s
sub-Saharan Africa, where little or no reduction in MDG 4 is to reduce this to 47 per 1000 by 2015. In
mortality in children younger than 5 years was evident Tanzania, demographic and health surveys were done
throughout the 1990s. Since 2000, global health initiatives in 1992, 1996, 1999, and 2005.13–16 The first three surveys
and resources for health have increased sharply,7 which showed that the rate of child mortality throughout
has increased coverage of life-saving child health the 1990s was high but static, oscillating between 141 and
interventions in several countries.8–10 We would therefore 147 deaths per 1000 children (table 1). The most recent
expect to see more evidence of progress towards MDG 4 survey, from late 2004 and early 2005, showed that the
in such settings in the mid-decade assessments. probability that a child would die before they reached
Since registration systems in sub-Saharan Africa have their fifth birthday fell by 24%, from 146·6 (95% CI
low coverage, most countries rely on periodic national 128·4–164·8) deaths per 1000 in 1999 to 112·0 (95% CI
1276 www.thelancet.com Vol 371 April 12, 2008
Articles
102·6–121·5) deaths per 1000 in 2004 (p<0·02).15 Similarly,
Midpoint of period Sample size Mortality (deaths per 1000)
the probability of dying before the first birthday (data not (households)
shown) fell by 31% from 99 to 68 deaths per 1000 over the
1987–9213 1990 8327 141·2 (95% CI 128·1–154·3)
same period. Reductions in mortality were concentrated
1991–9614 1993 7969 136·5 (95% CI 124·8–148·2)
in postneonatal infants (ie, those older than 28 days and
1994–99*16 1996 3615 146·6 (95% CI 128·4–164·8)
younger than 12 months) and were greater in rural areas.
2000–0515 2003 9735 112·0 (95% CI 102·6–121·5)
Neither neonatal nor maternal survival increased during
this period. The 24% drop in mortality in children Data from four demographic and health surveys in Tanzania since 1990. *The 1999 survey was an interim survey of
13–16
younger than 5 years, to 112 deaths per 1000, was reproductive and child health, that used a smaller sample size but identical methods for estimation of mortality.
calculated from the average mortality across the 5 years Table 1: Estimates of mortality in children younger than 5 years
before the survey.
Such a decline is unlikely to be due to one factor.17 But in 1991–92, and 22 000 in 2001–02. The sampling of the
what can account for it? What are the prospects now for survey was designed to allow estimates of household
Tanzania to reach MDG 4 over the ensuing 10 years? And variables for the 21 administrative regions of mainland
what can we learn that would help other countries to Tanzania. Household and individual indicators included
accelerate progress towards MDG 4? We aimed to measures of income poverty and performance of priority
calculate the annual rates to examine the pattern of the sectors as defined in a paper on the government’s
reduction in mortality and to see if the point estimate for poverty-reduction strategy.20,21 Data for trends in gross
the year 2004 differed from historical values or from the domestic product (GDP) per person were obtained from
period average. We also investigated Tanzania’s health- the Bank of Tanzania’s annual reports,22 the Penn World
system investments, including coverage of child-survival Tables,23 and the Tanzania public expenditure review.24
interventions between the late 1990s and 2000–04, and
examined other factors, not related to the health system, Statistical analysis
such as national economic growth, poverty reduction, We analysed the raw data from all four Tanzania DHS
food security, climate shock, fertility, maternal education, surveys (1992, 1996, 1999, and 2004)13–16 to generate several
and HIV/AIDS, that could plausibly have exerted large, estimates of mortality in children younger than 5 years
rapid effects on child survival. for every 1-year period before the respective survey back
to 1990, by use of direct methods based on complete birth
Methods histories. For every child recorded in these birth histories,
Data sources we computed survival for every month from birth until
To assess trends in mortality since 1990 we used all four either their fifth birthday or the date of the survey. We
Tanzanian demographic and health surveys, from 1992, grouped periods at risk and deaths for each calendar year,
1996, 1999, and 2004–05.13–16 These were nationally and constructed a separate life table for each year in the
representative cluster sample surveys that covered 8327, birth histories for which sufficient data were available to
7969, 3615, and 9735 households in 1992, 1996, 1999, and show, for a person at each age, the probability that they
2005, respectively. The surveys provided direct estimates would die before their next birthday. This generated
of child mortality through complete fertility (birth) 35 estimates of mortality over the 15-year period from 1990
histories of 32 877 women aged between 15 and 49 years. to 2004. We estimated trends in mortality from 1990
The surveys also provided detailed information about to 2004 by fitting Lowess regression25 of the natural log of
household demographics; asset ownership; dwelling mortality in children younger than 5 years [ln(5q0)] to
conditions; health and nutritional status of women and time with bandwidths ranging from 0·2 (representing
children; coverage of health-care services such as high sensitivity to recent data) to 2·0 (low sensitivity) and
immunisation, insecticide-treated nets, and maternal forecasted this trend for mortality from 2005 to 2015 with
and child health; and current knowledge and practices the same range of bandwidths. We calculated confidence
related to health. Survey data were obtained by trained intervals for probabilities with Greenwood’s formula.26
personnel, with the verbal informed consent of We obtained fiscal-year data on total health spending,
participants. To assess coverage of child-health both on-budget and off-budget, from the public-expenditure
interventions, we also used a 2003 survey on service reviews of the Tanzanian Ministry of Finance and Ministry
provision in Tanzania, which was a nationally of Health and Social Welfare.24 Spending data included all
representative facility-based survey of maternal and child domestic government health spending (including the
health and HIV/AIDS services.18 All the surveys provided government’s contribution to the national health insurance
cross-sectional data on intervention coverage in their fund) and all aid spending on health from official
respective years. documents. We did not include private out-of-pocket
We obtained data for poverty from Tanzanian household expenditure. We adjusted total government health
budget surveys in 1992 and 2002,19 which tracked the expenditure for each year with consumer price-index
progress of the government’s poverty-monitoring deflators on the 1998/99 base year to provide the total
strategy. These surveys sampled 4000 households government health expenditures per person per year. Thus,
www.thelancet.com Vol 371 April 12, 2008 1277
Articles
Factors not related to health systems included fertility,
200
GDP per person, and rates of poverty. We also examined
180 153·1 any major shocks, such as measles or meningitis
Mortality in children younger than 5 years
141·5
160 epidemics, famine, or increased food insecurity, that
128·2
(deaths per 1000 livebirths)
140 might have affected mortality differently in the 1990s and
108·6
120 after 2000.
100 83·2
Role of the funding source
80
The corresponding author had full access to all the data
60
in the study and had final responsibility for the decision
40 to submit for publication.
20
0 Results
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Year
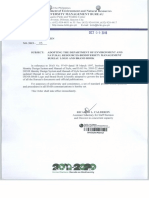
Our results for disaggregated annual mortality (figure 1)
show that the rate of reduction accelerated between 2000
Figure 1: Annual mortality in children younger than 5 years from 1990 to 2005 and 2004. In 2004–05, the reduction in mortality
Data are from an analysis of the 2004–05 national demographic and health surveys in Tanzania.15 Dotted line between 1990 and 1999 was 1·4% per year whereas
shows Tanzania’s MDG-4 target of 47 deaths per 1000 livebirths by 2015. Vertical lines show 95% CIs for survival
probabilities.
for 2000 to 2005, this trend accelerated to 10·8% per year
(from regression trend analysis). The point estimate of
200
mortality in children younger than 5 years in 2004
was 83·2 (95% CI 70·1–96·3) per 1000, which was
180 40% lower than typical values seen in the 1990s
corresponding to a change of 58·3 per 1000 in absolute
160
risk (95% CI 32·7–83·9). This raises the question: is
Mortality in children younger than 5 years
140 MDG 4 more achievable than was previously appreciated?
(deaths per 1000 livebirths)
Figure 2 shows the family of smoothed regressions of the
120
combined disaggregated mortality data from all four
100 demographic and health surveys with extrapolation
to 2015 under different weightings for the recent past. All
80 these weighting projections suggest that MDG 4 is within
60 reach in Tanzania by 2015.
We compared the status of selected health-system
40 factors across the major functions of governance,
financing, resource allocation, and service delivery
20
for 1999 and 2005. Health systems improved substantially
0 on the basis of most of the indicators that we investigated.
1990 1995 2000 2005 2010 2015 With respect to governance, financing, and resources,
Year
Tanzania adopted a sector-wide approach (SWAp) for
Figure 2: Estimates of annual mortality in children younger than 5 years medium-term and long-term planning, in which a
Data are from reanalysis of four national demographic and health surveys in Tanzania, which included the birth coherent policy and expenditure programme, under
histories of 32 877 women aged 15–49 years in 1992, 1996, 1999, and 2004–05.13–16 The MDG-4 target in 2015 is government leadership, was jointly funded by pooled
shown by the horizontal line. The dotted line shows the rate of reduction needed to reach this target. Lowess
regression forecasts of possible future trends are shown by coloured lines, with red giving most weight and yellow
government and donor partners. A so-called basket
giving least weight to recent data trends. fund, jointly funded by partners, was created to provide
an additional US$0·50 per person to districts as
monetary amounts are represented in the international recurrent financing support. This approach was
dollar, a hypothetical unit of currency with the purchasing implemented in 2000–01 and constituted a major change
power that the US dollar had in the USA at a specific time. in the health system that decentralised substantial
We obtained total health expenditure including private financial resources for the first time. Moreover,
out-of-pocket spending from WHO statistics.27 between 1999 and 2004, we noted a 2·3-fold increase in
We searched for information on all contextual factors total government health expenditure, from US$4·70 to
that might have affected trends in child survival, $11·70 per person. Total health expenditure, including
differentiating factors related to health systems from private expenditure, increased from US$23 to $29 per
those that were not.28 Factors related to health systems person,27 indicating that most of the growth in health
included the comparative provision, use, or coverage of spending was due to increases in government
key child-survival interventions in 1999 and 2004; relevant expenditure.
policy changes regarding management, decentralisation, On the policy front, many health reforms planned
and services; and trends in public expenditure on health. during the 1990s started to be implemented during
1278 www.thelancet.com Vol 371 April 12, 2008
Ref number 08TL_1668_1 Palette Special Characters
Articles
the 2000s, including the sector-wide approach basket
1999
funding; new guidelines, methods, and informatics for 2005
district planning and management; and new policies
Antenatal care
(eg, substitution of more effective first-line anti-malarial
drugs). Under its poverty-reduction strategy, Tanzania’s
Measles immunisation
Ministry of Health and Social Welfare increased the
priority of cost-effective interventions which supported Fully immunised child at 12 months
national decisions and commitments to scale up and
strengthen several key child-survival interventions such Exclusive breastfeeding 0–2 months
as Integrated Management of Childhood Illness (IMCI),
vitamin A supplementation, immunisation, and Child given oral rehydration treatment
insecticide-treated nets. We did not record major gains
in numbers of health professionals or physical Iron supplementation
Intervention
infrastructure for health during this period.
Malaria intermittent preventive treatment
For service delivery, the coverage of interventions
relevant to child survival improved between the 1999
Exclusive breastfeeding 0–6 months
and 2004–05 surveys (figure 3). The most noticeable
changes were vitamin A supplementation (up from 14% Households with at least one mosquito net
in 1999 to 85% in 2005), IMCI (up from 19% to 73% of
districts), households with mosquito nets (up from 21% Districts with integrated management
of childhood illnesses
to 46%), children sleeping under insecticide-treated nets
(up from 10% to 29%), iron supplementation in Vitamin A supplementation
pregnancy (up from 44% to 61%), oral rehydration
Child sleeping under ever-treated
therapy for children (up from 57% to 70%), and exclusive insecticide-treated net
breastfeeding for those younger than 2 months of age 0 10 20 30 40 50 60 70 80 90 100
(up from 58% to 70%) and younger than 6 months (up Coverage (%)
from 32% to 41%). Coverage of other interventions did
not change significantly, since it was already high Figure 3: Comparison of access to key child survival interventions between 1999 and 2005
in 1999 (figure 3). Coverage of prevention of Data are from national demographic and health surveys in Tanzania.
mother-to-child transmission of HIV (PMTCT) and
antiretroviral therapy as of 2005 remained very low, and water was a protected source.29 The total fertility rate
therefore unlikely to have contributed to a reduction in did not change over this period, but the average age at
mortality in children younger than 5 years. As a risk first birth was 19·0 years in 2000, and 19·4 years in
factor for child mortality, rates of underweight and 2002; the rate of adolescent childbearing diminished
stunted children improved from 29% and 44% in 1999, (from 26·1% to 24·6%); and median birth intervals did
to 22% and 38% in 2005, respectively. not change (33·3 and 33·4 months, respectively).
Of all the factors not related to Tanzania’s health Tanzania had a low rate of food-energy deficiency (43·9%)
system that could possibly have affected child survival in 2000.30
(table 2), the only change was a worsening of the The estimated prevalence of HIV in adults aged
manifestations of the HIV epidemic. Over the 5 years 15–49Refyears
numberwas 8%, according08TL_1668_3
to the demographic and Palette
of our study, Tanzania’s national wealth (in GDP per health survey in 1999,16 whereas the first national
Editor Editor name: TS Key 1 Key 1 Axis break
person) increased by 93 international dollars: from $819 community-based survey of HIV prevalence in 2003–04 Key 2 Key 2
to $912 per person between 1999 and 200423 (or US$256 established
Author the rate to be 7% inAuthoradults nameaged 15–49 years.18 Key 3 Key 3
to $303). The proportion of households living below the Urban areas had higher rates of HIV than did rural areas. Key 4 Key 4
Created by Illustrator name Key 5 Key 5
poverty line was 36% in 2001–02 and 39% in 1991–92 In 2004, only 3–9% of health facilities ran programmes Key 4 Key 4 Tick
(p=0·29). Poverty in urban areas, excluding Dar es for prevention
Section of mother-to-child-transmission
Section name: of HIV; Key 5 Key 5
Salaam, decreased from 29% to 26% during this period most of these were district and faith-based hospitals and
(p=0·60), whereas that in rural areas dropped from 41% a few health centres. By 2006, only 13% of health facilities
to 39% (p=0·52).29 The educational attainment of adults offered
Textat least one of the four components
retyped Urgent of the PMTCT
improved only marginally between 1999 and 2004, with programme.31
Image redrawn Special instructions
greater gains for women than for men (table 3).14,15 When we analysed the differentials between coverage
Similarly, literacy rates did not change; about two-thirds of health interventions between 1999 and 2004 using a
of the women were reported to be literate throughout modelling system,32 we extrapolated a 33% reduction of
this period. Population-based statistics on access to safe mortality in children younger than 5 years, from 129 to
water in Tanzania were sparse; those that were available 86 deaths per 1000 livebirths. These effects would mainly
indicated no change between 2000 and 2002 in the be attributable to reduction of postneonatal mortality in
proportion of households for which the main supply of children younger than 5 years.
www.thelancet.com Vol 371 April 12, 2008 1279
Articles
suggest that Tanzania is on the trajectory necessary to
1999 2004–05
achieve MDG 4 by 2015, for a range of different weightings
Gross domestic product per person US$256 US$303 of past performance in the distant or near past, back
Number living in poverty (food) 21·6% 18·7% to 1990. Our results differ from those of an analysis of all
Number living in poverty (basic 38·6% 35·7% available data from direct and indirect estimates of
needs)
mortality disaggregated into 2-year intervals, including
Food security No change
data before 1990, which concluded that Tanzania would
Climate shock No change
not be able to achieve this goal.6 However, the data from
Total fertility rate (children for 5·6 (5·0–6·1) 5·7 (5·4–5·9)
every mother)
before 1990 can have little bearing on the ability to achieve
a goal for which the starting point is 1990, especially
Low birthweight 133/3206 (3·8%) 344/8551 (3·7%)
since the purpose of the MDG was to elicit changes in
Age at first birth (years) 19·2 (17·4–21·6) 19·4 (17·7–21·8)
trends. To assume that the trend before 1990 continued
Birth spacing (months) 33·3 (28·0–41·0) 33·4 (28·0–42·4)
would imply that setting the goal was futile. In this
Meningitis epidemics None None
specific instance, performance was poor before 1990, and
Measles epidemics None None
inclusion of earlier data biases the conclusion towards a
HIV/AIDS epidemics Increasing
mortality slower improvement. Furthermore, all extrapolations
must, of necessity, assume a degree of continuity in the
Data are number (%), rate (95% CI), or median (IQR), unless otherwise specified. underlying processes, and so tend to over-smooth if a
Table 2: Comparison of non-health system changes between 1999 trend accelerates, as it seems to have done in Tanzania in
and 2005 that might be expected to affect child survival about 2000. Since aggregation of the data into longer
time-units tends to increase the degree of this smoothing,
we disaggregated the data into shorter time units.
Completed primary education Completed secondary Years of schooling The large reduction in mortality evident since 2000
education
immediately raises questions about the quality of surveys
1999 2004–05 1999 2004–05 1999 2004–05 and data and about comparability over time. Additional
Women 46% 49% 5% 9% 6·1 6·2 quality control was provided for the 2004–05 demographic
Men 51% 52% 7% 11% 6·2 6·3 and health survey and its data precisely because fewer
child deaths were recorded than were expected.15
Data are from demographic and health surveys in Tanzania in 1999 and 2005.15,16
Under-reporting bias could also have occurred, for
Table 3: Educational attainment of men and women aged 15–49 years example if maternal mortality increased because of
HIV/AIDS or other factors. The cross-sectional
Discussion demographic and health surveys did not gather
In Tanzania, the most recent demographic and health information about children whose mothers died.
survey in 2005 showed a 24% improvement in child However, the demographic surveillance systems in
survival, with mortality rates in children younger than Tanzania, which track entire populations longitudinally,
5 years down from 147 deaths per 1000 for 1994–99 to also reported reductions in mortality in children younger
112 deaths per 1000 for 2000–04 (p<0·02).15,33 In national than 5 years, which substantiates the data from the
birth-history surveys, these 5-year averages conceal the demographic and health surveys.35 Furthermore,
pattern and degree of change in yearly rates. Since this demographic and health surveys in 1999 and 2005 did
5-year change substantially exceeded 15%, the minimum not detect any major increases in maternal mortality
regarded by Korenromp and colleagues34 as indicative of between these two periods, although such changes would
a true reduction, we decided to calculate the yearly rates be difficult to detect in sample sizes used in the
to examine the pattern of the reduction and to see if the demographic and health surveys. With respect to deaths
point estimate for the year 2004 differed from historical of mothers due to HIV/AIDS, reduced mortality in
values or from period average. children younger than 5 years is probably not an artifact
Our analysis of the annual rates shows a pattern of caused by the under-reported deaths, since the estimated
continuous reduction in mortality reaching 83·2 (95% CI magnitude of this effect in a rural Tanzanian population
70·1–96·3) deaths per 1000 in 2004. Within the with an HIV prevalence of 4·3% would underestimate
2004–05 survey data, five of the six lowest values over the deaths in children younger than 5 years by only 2·3%.36
15 years were recorded in the last 5 years,15 indicating that If we assume that our finding of a reduction in mortality
mortality in this group fell by 40% between 1990 and 2004. for children younger than 5 years is real, what can explain
Based on Tanzania’s 2002 population of 34·4 million, this apparent acceleration of survival in Tanzania after a
this finding suggests that 280 000 children’s lives were decade of high but static mortality rates in the 1990s?
saved between 1999 and 2005 that would otherwise have And can this improvement be sustained? We examined
been lost had the prevailing rate of the 1990s continued. differences in the health system in Tanzania between 1999
Our analyses of data from all four demographic and and 2004 and in external factors that could reasonably be
health surveys, analysed by year of reference, thus expected to have contributed to large survival gains over
1280 www.thelancet.com Vol 371 April 12, 2008
Articles
this short period. Between 1999 and 2004, Tanzania more interventions, such as antenatal care an immunisation,
than doubled its public expenditure on health; such coverage was already high, and did not change.
increased expenditure has been strongly correlated with Modelling showed that a 33% reduction of mortality in
increased survival in children younger than 5 years in children younger than 5 years could be expected
developing countries, especially in poor people.37 between 1999 and 2004, from 129 to 86 deaths per
Increased public expenditure on health could also be 1000 livebirths. These effects would mainly be in
especially powerful in decentralised health systems when reduction of postneonatal mortality in children younger
such resources are targeted towards essential cost-effective than 5 years. The predicted failure to affect neonatal (and
interventions.38 Tanzania implemented such governance maternal) mortality draws attention to problems with the
shifts towards greater decentralisation in 2000, by continuum of care necessary to achieve MDGs. The
introducing sector-wide capitation grants that gave general scarcity of data and analyses continues to limit
districts substantial financial resources. This was perhaps programme efforts and monitoring of progress.
one of the most important distinctions in Tanzania’s Among factors not related to the health system, gains
health system between the 1990s and the 2000s, since it in wealth would be expected to exert a major effect on
opened opportunities for local problem solving and survival in children younger than 5 years. Tanzania has
provided resources for districts to selectively increase enjoyed many decades of political stability and, in recent
resources for key interventions, as has been shown in years, steady economic growth. Nevertheless, GDP per
pilot studies since 1996.38 person has increased by only 93 international dollars
Decentralisation allowed the introduction and scale-up (US$47) over the 5 years between 1999 and 2004. An
of new interventions such as the integrated management increase of this size corresponds to an expected decrease
of childhood illness, which facilitated adoption of new in mortality in children younger than 5 years of 2·2%, on
treatment policies for malaria that replaced failing the basis of a regression of GDP (in international dollars)
first-line treatments with more effective case management per person and mortality in children younger than 5 years
for the largest single cause of death for children. The for 45 sub-Saharan countries (data reanalysed from WHO
IMCI programme also assisted promotion of the use of statistics).27 Although important, this growth in national
insecticide-treated nets for malaria prevention. Sentinel wealth would be unlikely to account for much of our
districts had piloted the introduction of IMCI from 1997, finding of a 40% reduction in mortality, especially since
with full provision, increased use, and effective coverage the proportion of the population living below the absolute
by 1999–2000.39 Impact studies showed that, after a 2-year poverty line and food poverty line in the 1990s had
follow-up, IMCI was associated with 13% lower child improved only slightly in 2002. Although gains have been
mortality in pilot districts that had health-system made in the education of Tanzania’s current cohort of
strengthening than in other districts.40 Other pilot studies schoolchildren, child-health outcomes are affected by the
in Tanzania showed the high local effectiveness of educational status of parents, which had improved only
insecticide-treated nets for reduction of mortality in marginally by 2004. Early child-bearing and short
children of this age.41 birth-spacing both raise the risk of child mortality, and
Tanzania started nationwide scale-up of the total fertility rate, average age at first birth, adolescent
insecticide-treated nets in 1999 and of IMCI in 2000, and childbearing, and median birth intervals remained
changed its drug policy for malaria in 2001. Since malaria similar in the two periods. Hence changes in fertility
mortality in Tanzania is concentrated in postneonatal probably did not contribute to our findings of a large
infants younger than 5 years,42 the survival gains recorded improvement in child survival.
in the 2004–05 demographic and health survey were We did not find evidence of any major epidemics (for
highest for postneonatal infants, suggesting that example, of measles or meningitis) that might have
malaria-specific mortality reduction has made progress. occurred in the late 1990s but not in the early 2000s.
Moreover, several sentinel sites in Tanzania, which Conversely, adult and child mortality due to HIV/AIDS
monitor cause-specific mortality by use of continuous continued to increase slowly,43 and therefore differentials
longitudinal demographic surveillance systems, also in HIV/AIDS interventions might have affected overall
reported reductions in mortality in children younger mortality, since 25% of children who are born to
than 5 years before the findings of the 2004–05 HIV-positive mothers are infected. The PMTCT
demographic and health surveys, and detected declines programme is a proven cost-effective combination of
in malaria and acute febrile illness deaths in children strategies and interventions that can be tailored to specific
younger than 5 years.34,43 These findings add plausibility local conditions. These interventions and strategies,
to the hypothesis that the collective effect of a multifaceted including voluntary and confidential counselling and
approach to malaria contributed to child-survival gains testing, provision of antiretroviral drugs to HIV-positive
during this period.44 Coverage of other child-survival pregnant women, planning of safe delivery procedures,
interventions, such as vitamin A supplementation,45 and counselling about appropriate infant-feeding options,
exclusive breastfeeding, oral rehydration therapy and can reduce mother-to-child transmission by 50%.
iron supplementation for children, increased. For other However, in Tanzania access to HIV/AIDS interventions
www.thelancet.com Vol 371 April 12, 2008 1281
Articles
such as voluntary counselling and testing, PMTCT, and We were unable to estimate the relative contributions
antiretrovirals was not yet sufficient as of 2004 to have of different factors in the health system to reduction of
affected child survival on a national scale. Epidemic child mortality since 2000. However, the collective weight
patterns, including HIV/AIDS and its response, can of so many positive changes in the health system, in the
therefore be excluded as an explanation for the reduction absence of other explanations, is compelling. Rather, we
in child mortality, and could even have worked against could ask why we would not expect to see gains in
this trend. survival.5 Broad, multifaceted progress in stewardship,
Nutrition can be determined by health systems (eg, public expenditure on health, decentralised financing,
micronutrient supplementation and other health sector resource allocation, and better coverage of essential
interventions) and by other factors (eg, food insecurity, child-survival services can work synergistically to effect
poverty, climate shocks, and natural disasters). We did important progress towards MDG 4 in low-income
not identify evidence of major events outside the health countries such as Tanzania. Increased health resources
system that could have contributed to changes in combined with strengthening of decentralised health
nutritional status in Tanzania during the study period. systems to ensure that life-saving interventions reach
However, the nutritional status of children did improve those in need is a key child-survival strategy.
slightly, possibly because of better access to various Contributors
general health interventions (eg, IMCI, insecticide-treated HM and DDS led the conceptualisation of the paper with contributions
nets, and vitamin A supplementation), and slight gains from all authors and wrote the first draft. PS compiled statistical data,
and HM, TS, and DDS did statistical analyses. JS, TJ, CM, GU, TB, and
in wealth. Improved nutritional status is likely to have CV contributed to the interpretation and writing of this manuscript. All
contributed to the reduced risk of mortality in children authors have seen and approved the final version.
younger than 5 years. Conflict of interest statement
If we assume that the trend is real, and is due to a We declare that we have no conflict of interest.
strengthening health system and increased access to key Acknowledgments
child-survival interventions, can this trend be continued? We thank the Government of Norway for encouragement and financial
It should be noted that the most recent demographic and assistance.
health survey, in 2004–05, preceded the potential effect of References
increased funding to Tanzania from the Global Fund to 1 Horton R. A new global commitment to child survival. Lancet 2006;
368: 1041–42.
Fight HIV/AIDS, Tuberculosis and Malaria. Although 2 Martines J, Paul VK, Bhutta ZA, et al. Neonatal survival: a call for
the first grants were announced in late 2002, the actual action. Lancet 2005; 365: 1189–97.
programmes that they supported did not begin until 3 Lawn JE, Cousens S, Bhutta ZA, et al. Why are 4 million newborn
late 2004, and the benefits would not have been detectable babies dying each year? Lancet 2004; 364: 399–401.
4 Bryce J, el Arifeen S, Bhutta ZA, et al. Getting it right for children:
in the last demographic and health survey but can be a review of UNICEF joint health and nutrition strategy for 2006–15.
expected to assist the downward trend into the future. Lancet 2006; 368: 817–19.
For children, these funds will boost access to 5 Black RE, Morris S, Bryce J. Where and why are 10 million children
dying every year? Lancet 2003; 361: 2234.
insecticide-treated nets through a national voucher
6 Murray CJ, Laakso T, Shibuya K, Hill K, Lopez AD. Can we achieve
scheme, which is designed to provide the nets to all Millennium Development Goal 4? New analysis of country trends
pregnant women and their newborn babies, which and forecasts of under-5 mortality to 2015. Lancet 2007; 370: 1040–54.
started in late 2004. Scaling up the PMTCT programme 7 Horton R. The coming decade for global action on child health.
Lancet 2006; 367: 3–5.
and antiretroviral therapy started in 2005; programmes 8 Bryce J, Terreri N, Victora CG, et al. Countdown to 2015: tracking
for zinc supplementation and oral rehydration therapy intervention coverage for child survival. Lancet 2006; 368: 1067–76.
started in 2007; and access to improved antimalarial 9 Victora CG, Fenn B, Bryce J, Kirkwood BR. Co-coverage of
preventive interventions and implications for child-survival
treatment through artemisinin combination therapy strategies: evidence from national surveys. Lancet 2005; 366: 1460–6.
in 2007. 10 UNICEF and Roll Back Malaria. Malaria & children: progress in
Since neonatal mortality remains constant and forms intervention coverage. New York, USA: UNICEF, 2007.
an increasing share of the mortality in children younger 11 Morris SS, Black RE, Tomaskovic L. Predicting the distribution of
under-five deaths by cause in countries without adequate vital
than 5 years, it could emerge as a barrier to continued registration systems. Int J Epidemiol 2003; 32: 1041–51.
reductions in mortality and attainment of MDG 4. 12 UNICEF. Countdown to 2015 child survival: tracking progress in
Renewed efforts are being planned to address neonatal child survival. New York, USA: UNICEF, 2005.
and maternal mortality in Tanzania. These efforts will 13 National Bureau of Statistics, Tanzania, and Macro International.
Tanzania demographic and health survey 1991–02. Dar es Salaam,
coincide with a doubling in the sector-wide district basket Tanzania: National Bureau of Statistics and Calverton, MD, USA:
fund for the Tanzanian health system to US$1·00 per Macro International, 1993.
person per year. Such continued efforts at scaling up will 14 National Bureau of Statistics, Tanzania, and Macro International.
Tanzania demographic and health survey 1996. Dar es Salaam,
need concomitant investments in strengthening of health Tanzania: National Bureau of Statistics and Calverton, MD, USA:
systems, including management of human resources, Macro International, 1997.
procurement and supply chain management, health 15 National Bureau of Statistics, Tanzania, and ORC Macro. Tanzania
demographic and health survey 2004–05. Dar es Salaam, Tanzania:
information management, and constant attention to National Bureau of Statistics and Calverton, MD, USA: ORC
enhancing quality of care. Macro, 2005.
1282 www.thelancet.com Vol 371 April 12, 2008
Articles
16 National Bureau of Statistics, Tanzania, and Measure Evaluation. 32 The Futures Group International. Spectrum policy modeling
Tanzania reproductive and child health survey 1999. Dar es Salaam, system: projecting future requirements for improving reproductive
Tanzania: National Bureau of Statistics and Chapel Hill, NC, USA: health. Washington, DC, USA: The Futures Group
Measure Evaluation, 2000. International, 2008.
17 Victora CG, Schellenberg JA, Huicho L, et al. Context matters: 33 Janson A. Shed some light on darkness: will Tanzania reach the
interpreting impact findings in child survival evaluations. millennium development goals? Acta Paediatr 2007; 96: 781–86.
Health Policy Plan 2005; 20: 18–31. 34 Korenromp EL, Arnold F, Williams BG, Nahlen BL, Snow RW.
18 National Bureau of Statistics, Tanzania, ORC Macro International, Monitoring trends in under-5 mortality rates through national birth
and Tanzania Commission for AIDS. Tanzania HIV/AIDS indicator history surveys. Int J Epidemiol 2004; 33: 1293–301.
survey 2003–04. Dar es Salaam, Tanzania: National Bureau of 35 Adult Morbidity and Mortality Project and Ministry of Health,
Statistics, 2005. Tanzania. The policy implications of Tanzania’s mortality burden:
19 National Bureau of Statistics, Tanzania. Tanzania household budget A ten-year community based perspective. Dar es Salaam, Tanzania:
survey 2000–01. Dar es Salaam, Tanzania: Government of Ministry of Health, 2004.
Tanzania, 2003. 36 Ng’weshemi J, Urassa M, Isingo R, et al. HIV impact on mother
20 Government of Tanzania. Poverty reduction strategy paper. Dar es and child mortality in rural Tanzania. J Acquir Immune Defic Syndr
Salaam, Tanzania: Government of Tanzania, 2001. 2003; 33: 393–404.
21 Government of the United Republic of Tanzania and Vice 37 Houweling TA, Kunst AE, Looman CW, Mackenbach JP.
President’s Office. National strategy for growth and reduction of Determinants of under-5 mortality among the poor and the rich:
poverty (NSGRP). Dar es Salaam, Tanzania: Government of a cross-national analysis of 43 developing countries. Int J Epidemiol
Tanzania, 2005. 2005; 34: 1257–65.
22 Bank of Tanzania. Tanzania: Economic and Financial Indicators. 38 de Savigny D, Kasale H, Mbuya C, Reid G. Fixing health systems.
Dar es Salaam, Tanzania: Bank of Tanzania. http://www.bot-tz.org/ Ottawa, Canada: International Development Research Centre, 2004.
Publications/EconomicIndicators/EconomicAndFinancialIndicator 39 Armstrong Schellenberg JRM, Bryce J, de Savigny D, et al. The
s.htm (accessed on Jan 23, 2007). effect of Integrated Management of Childhood Illness on observed
23 Heston A, Summers R, Aten B. Penn world table version 6.2. quality of care of under-fives in rural Tanzania. Health Policy Plan
Philadelphia, PA, USA: University of Pennsylvania, 2006. 2004; 19: 1–10.
http://pwt.econ.upenn.edu/ (accessed Nov 25, 2007). 40 Armstrong Schellenberg JRM, Adam T, Mshinda H, et al.
24 Ministry of Health, Tanzania. Public expenditure review (PER) Effectiveness and cost of facility-based Integrated Management of
2000–2006. Dar es Salaam, Tanzania: Ministry of Health, United Childhood Illness (IMCI) in Tanzania. Lancet 2004; 364: 1583–94.
Republic of Tanzania, 2006. 41 Armstrong Schellenberg JRM, Abdulla S, Nathan R, et al. Effect of
25 Cleveland WS, Devlin SJ. Locally weighted regression: an approach large-scale social marketing of insecticide-treated nets on child
to regression analysis by local fitting. J Am Stat Assoc 1988; survival in rural Tanzania. Lancet 2001; 357: 1241–47.
83: 596–610. 42 Abdulla S, Adazu K, Masanja H, et al. Patterns of age-specific
26 Collet D. Modelling survival data in medical research. London, UK: malaria mortality in children in endemic areas of sub-Saharan
Chapman & Hall, 1994. Africa. Am J Trop Med Hyg 2007; 77: 99–105.
27 WHO. World health statistics 2007. Geneva, Switzerland: World 43 Ministry of Health and Social Welfare, Tanzania. Annual health
Health Organization, 2007. statistical abstract. Dar es Salaam, Tanzania: Ministry of Health and
28 Habicht JP, Victora CG, Vaughan JP. Evaluation designs for Social Welfare, 2006.
adequacy, plausibility and probability of public health programme 44 Rowe AK, Steketee RW, Arnold F, et al. Viewpoint: evaluating the
performance and impact. Int J Epidemiol 1999; 28: 10–18. impact of malaria control efforts on mortality in sub-Saharan
29 United Republic of Tanzania Research and Analysis Working Africa. Trop Med Int Health 2007; 12: 1524–39.
Group. Poverty and human development report 2005. Dar es 45 Masanja H, Schellenberg JA, Mshinda HM, et al. Vitamin A
Salaam, Tanzania: Mkuni na Nyota Publishers, 2005. supplementation in Tanzania: the impact of a change in
30 Smith LC, Alderman H, Aduayom D. Food insecurity in programmatic delivery strategy on coverage. BMC Health Serv Res
sub-Saharan Africa: new estimates from household expenditure 2006; 6: 142.
surveys. Washington, DC, USA: International Food Policy Research
Institute, 2006.
31 National Bureau of Statistics, Tanzania, and Macro International.
Tanzania service provision assessment survey 2006. Dar es Salaam,
Tanzania: National Bureau of Statistics and Calverton, MD, USA:
Macro International, 2007.
www.thelancet.com Vol 371 April 12, 2008 1283
S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Harmony Radio, R2.8: Order Codes ReferenceDocument51 paginiHarmony Radio, R2.8: Order Codes ReferenceRalaivao Solofohery Dieu-donnéÎncă nu există evaluări
- CM760 E-Brochure HemobasculaDocument6 paginiCM760 E-Brochure Hemobasculajordigs50Încă nu există evaluări
- GSP Product Info 092711Document19 paginiGSP Product Info 092711Joao SilvaÎncă nu există evaluări
- The Influence of The Transformational LeaderDocument9 paginiThe Influence of The Transformational Leaderkenmuira100% (1)
- Corrugated Horn AntennasDocument4 paginiCorrugated Horn AntennasmiusayÎncă nu există evaluări
- Aling MODEDocument29 paginiAling MODEBojan PetronijevicÎncă nu există evaluări
- Ems Accounting Term 2Document39 paginiEms Accounting Term 2Paballo KoopediÎncă nu există evaluări
- Green Tyre TechnologyDocument4 paginiGreen Tyre TechnologyAnuj SharmaÎncă nu există evaluări
- Add MITx Credentials To Resume and LinkedIn PDFDocument5 paginiAdd MITx Credentials To Resume and LinkedIn PDFRizwanÎncă nu există evaluări
- PV1800VPM SEREIS (1-5KW) : Pure Sine Wave High Frequency Solar Inverter With MPPT InsideDocument4 paginiPV1800VPM SEREIS (1-5KW) : Pure Sine Wave High Frequency Solar Inverter With MPPT InsideHuber CallataÎncă nu există evaluări
- Modern Theory of Interest: IS-LM CurveDocument36 paginiModern Theory of Interest: IS-LM CurveSouvik DeÎncă nu există evaluări
- Puch Moped Horn Wiring Diagram (Chrome Oval Switches)Document1 paginăPuch Moped Horn Wiring Diagram (Chrome Oval Switches)MopedgalÎncă nu există evaluări
- MCMCHistoryDocument18 paginiMCMCHistoryAli S.Încă nu există evaluări
- Tugas Moneter CH 4 - Dewi Lucky Aryanti Sinaga F1119025Document4 paginiTugas Moneter CH 4 - Dewi Lucky Aryanti Sinaga F1119025Scream InungÎncă nu există evaluări
- Food Safety and StandardsDocument8 paginiFood Safety and StandardsArifSheriffÎncă nu există evaluări
- Excel Tips TricksDocument26 paginiExcel Tips Tricksskondra12Încă nu există evaluări
- Introduction To Investment AppraisalDocument43 paginiIntroduction To Investment AppraisalNURAIN HANIS BINTI ARIFFÎncă nu există evaluări
- International Advertising: Definition of International MarketingDocument2 paginiInternational Advertising: Definition of International MarketingAfad KhanÎncă nu există evaluări
- Essays From Previous Years For HseeDocument2 paginiEssays From Previous Years For HseeGagan TottempudiÎncă nu există evaluări
- Vocabulary List Year 6 Unit 10Document2 paginiVocabulary List Year 6 Unit 10Nyat Heng NhkÎncă nu există evaluări
- Section 8 33KVDocument13 paginiSection 8 33KVMuna HamidÎncă nu există evaluări
- Brigada EskwelaDocument4 paginiBrigada EskwelaJas Dela Serna SerniculaÎncă nu există evaluări
- White Paper - Data Communication in Substation Automation System SAS - Part 1 Original 23353Document5 paginiWhite Paper - Data Communication in Substation Automation System SAS - Part 1 Original 23353sabrahimaÎncă nu există evaluări
- National Knowledge Commision and Its Implication in Higher EducationDocument73 paginiNational Knowledge Commision and Its Implication in Higher Educationabhi301280100% (1)
- Epsilon Range Bomba HorizontalDocument8 paginiEpsilon Range Bomba HorizontalsalazarafaelÎncă nu există evaluări
- Biodiversity Management Bureau: Repucjuf The Philippines Department of Environment and Natural ResourcesDocument36 paginiBiodiversity Management Bureau: Repucjuf The Philippines Department of Environment and Natural ResourcesMarijenLeañoÎncă nu există evaluări
- 8051 Development Board Circuit DiagramDocument1 pagină8051 Development Board Circuit DiagramRohan DharmadhikariÎncă nu există evaluări
- Model Solar Car DesignDocument21 paginiModel Solar Car DesignSemih HürmeydanÎncă nu există evaluări
- 2.1 Article On Reasonable Compensation Job Aid 4-15-2015Document3 pagini2.1 Article On Reasonable Compensation Job Aid 4-15-2015Michael GregoryÎncă nu există evaluări
- My Linux Attack Commands-ADocument51 paginiMy Linux Attack Commands-Aapogee.protectionÎncă nu există evaluări