S-ar putea să vă placă și
- GAP ANALYSIS Patient Safety Event Reporting SystemDocument76 paginiGAP ANALYSIS Patient Safety Event Reporting SystemJery JsÎncă nu există evaluări
- POSTER Event Reporting ContestDocument1 paginăPOSTER Event Reporting ContestJery JsÎncă nu există evaluări
- POSTER Event Reporting Examples ACUTEDocument8 paginiPOSTER Event Reporting Examples ACUTEJery JsÎncă nu există evaluări
- Appendix E - Just Culture FlowChartDocument1 paginăAppendix E - Just Culture FlowChartJery JsÎncă nu există evaluări
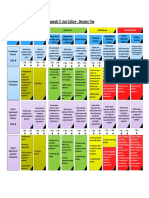
- Appendix C - Just Culture Decision TreeDocument1 paginăAppendix C - Just Culture Decision TreeJery JsÎncă nu există evaluări
- Just Culture March 2018Document12 paginiJust Culture March 2018Jery JsÎncă nu există evaluări
- Ebook A Guide To Improving Your Patient Safety Event Reporting Culture Plus A Leadership Action ListDocument8 paginiEbook A Guide To Improving Your Patient Safety Event Reporting Culture Plus A Leadership Action ListJery JsÎncă nu există evaluări
- Appendix B - Just Culture Workflow ProcessDocument1 paginăAppendix B - Just Culture Workflow ProcessJery JsÎncă nu există evaluări
- Nursing RatioDocument1 paginăNursing RatioJery JsÎncă nu există evaluări
- Appendix A - Just Culture AlgorithmDocument1 paginăAppendix A - Just Culture AlgorithmJery JsÎncă nu există evaluări
- CALCULATOR Patient Safety Event Reporting Rate CalculatorDocument13 paginiCALCULATOR Patient Safety Event Reporting Rate CalculatorJery JsÎncă nu există evaluări
- Appendix A - AlgorithmDocument1 paginăAppendix A - AlgorithmJery JsÎncă nu există evaluări
- CHECKLIST Intensive Reporting Days ChecklistDocument1 paginăCHECKLIST Intensive Reporting Days ChecklistJery JsÎncă nu există evaluări
- GAP ANALYSIS Patient Safety Event Reporting SystemDocument76 paginiGAP ANALYSIS Patient Safety Event Reporting SystemJery JsÎncă nu există evaluări
- ESR Required Documents (Policies, Guidelines, Forms) : Policy HR.5Document4 paginiESR Required Documents (Policies, Guidelines, Forms) : Policy HR.5Jery JsÎncă nu există evaluări
- ESR Required Documents (Policies, Guidelines, Forms) : Policy HR.5Document4 paginiESR Required Documents (Policies, Guidelines, Forms) : Policy HR.5Jery JsÎncă nu există evaluări
- KPI Monitoring ManualDocument231 paginiKPI Monitoring ManualJery Js100% (1)
- KPI Monitoring ManualDocument229 paginiKPI Monitoring ManualJery JsÎncă nu există evaluări
- CBAHI New StandardDocument267 paginiCBAHI New StandardJack Patag100% (2)
- CBAHI-ESR Standards Handbook AMANDocument28 paginiCBAHI-ESR Standards Handbook AMANJery JsÎncă nu există evaluări
- Dr. Shaptar. EyeDocument1 paginăDr. Shaptar. EyeJery JsÎncă nu există evaluări
- Implementation Guidelines For The Canadian Emergency Department Triage & Acuity Scale (CTAS)Document27 paginiImplementation Guidelines For The Canadian Emergency Department Triage & Acuity Scale (CTAS)Jery JsÎncă nu există evaluări
- Hospital Survey On Patient SafetyDocument18 paginiHospital Survey On Patient SafetyJery JsÎncă nu există evaluări
- Final Revisions To Telemedicine StandardsDocument3 paginiFinal Revisions To Telemedicine StandardsJery JsÎncă nu există evaluări
- Quality Management Program MonitoringDocument14 paginiQuality Management Program MonitoringJery JsÎncă nu există evaluări
- 16 Typical Hospital Business Process KPIs in Two CategoriesDocument6 pagini16 Typical Hospital Business Process KPIs in Two CategoriesJery JsÎncă nu există evaluări
- Hospital structure indicators dashboardDocument4 paginiHospital structure indicators dashboardJery JsÎncă nu există evaluări
- CBAHI IndicatorsDocument4 paginiCBAHI IndicatorsJery Js0% (1)
- December 2020 KPIDocument9 paginiDecember 2020 KPIJery JsÎncă nu există evaluări
- KPI Guidance Version1.1 2013Document70 paginiKPI Guidance Version1.1 2013Silvia IonitaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Neonates: Clinical Syndromes and Cardinal Fea-Tures of Infectious Diseases: Approach To Diagnosis and Initial ManagementDocument7 paginiNeonates: Clinical Syndromes and Cardinal Fea-Tures of Infectious Diseases: Approach To Diagnosis and Initial ManagementFatma ElzaytÎncă nu există evaluări
- HPWJ Medical Alert Card SampleDocument2 paginiHPWJ Medical Alert Card SampleSameer Kumar JubailÎncă nu există evaluări
- Aortic AneurysmDocument26 paginiAortic Aneurysmchetanm2563100% (1)
- What Are The Psychological Benefits of GratitudeDocument6 paginiWhat Are The Psychological Benefits of GratitudebrendaÎncă nu există evaluări
- Acute Severe Asthma (Status Asthmaticus)Document20 paginiAcute Severe Asthma (Status Asthmaticus)blok etikakedokteranÎncă nu există evaluări
- Health7 q1 Mod5 Healthservices v3Document24 paginiHealth7 q1 Mod5 Healthservices v3Jas Dela Serna SerniculaÎncă nu există evaluări
- Analysis On The Green Economic Productivity ofDocument42 paginiAnalysis On The Green Economic Productivity ofIrllyshouldslepepÎncă nu există evaluări
- PERDEV Handout - M5 (Coping With Stress) - ModifiedDocument2 paginiPERDEV Handout - M5 (Coping With Stress) - ModifiedElla MirandaÎncă nu există evaluări
- Virtual GriefDocument1 paginăVirtual GriefWXYZ-TV Channel 7 DetroitÎncă nu există evaluări
- Levocetirizine Dihydrochloride 5 MG Film-Coated Tablet AntihistamineDocument3 paginiLevocetirizine Dihydrochloride 5 MG Film-Coated Tablet AntihistamineRuel Vincent AsubarÎncă nu există evaluări
- Making Decisions About CPR: Learning OutcomesDocument8 paginiMaking Decisions About CPR: Learning Outcomesicen00bÎncă nu există evaluări
- Understanding the pros and cons of early marriage for teenagersDocument15 paginiUnderstanding the pros and cons of early marriage for teenagersShoba ManoharanÎncă nu există evaluări
- Brain Tumors - KY Cancer RegistryDocument45 paginiBrain Tumors - KY Cancer RegistryMohammad Galih PratamaÎncă nu există evaluări
- Managing Rheumatic and Musculoskeletal Diseases - Past, Present and FutureDocument6 paginiManaging Rheumatic and Musculoskeletal Diseases - Past, Present and FutureNICOLASÎncă nu există evaluări
- Engine Oil MsdsDocument4 paginiEngine Oil MsdsTawanda MushayiÎncă nu există evaluări
- Incident Reporting and Investigation ProcedureDocument8 paginiIncident Reporting and Investigation ProcedureWitara Saja67% (3)
- Iliotibial Band Syndrome - FannyDocument13 paginiIliotibial Band Syndrome - FannyAlfiani Rosyida Arisanti Syafi'iÎncă nu există evaluări
- Acute Appendicitis: Anatomy, Pathophysiology, and Clinical PresentationDocument26 paginiAcute Appendicitis: Anatomy, Pathophysiology, and Clinical PresentationSimonGonzalezAponteÎncă nu există evaluări
- Peter Lin, MD Biography: Medical TopicsDocument4 paginiPeter Lin, MD Biography: Medical TopicsBeo ThaiÎncă nu există evaluări
- Appointment Letters Independent DirectorsDocument62 paginiAppointment Letters Independent DirectorsArudra KumarÎncă nu există evaluări
- Types of Poverty: Learn Economics To Have A Better Understanding of How The Economy Affects EveryoneDocument4 paginiTypes of Poverty: Learn Economics To Have A Better Understanding of How The Economy Affects Everyoneluckii8star100% (1)
- Treatment Planning in Dentistry (Second Edition)Document476 paginiTreatment Planning in Dentistry (Second Edition)cahya100% (1)
- Journal Homepage: - : IntroductionDocument2 paginiJournal Homepage: - : IntroductionIJAR JOURNALÎncă nu există evaluări
- Ovitrelle Epar Medicine Overview - enDocument3 paginiOvitrelle Epar Medicine Overview - enPhysics with V SagarÎncă nu există evaluări
- Chapter 9 KeyDocument17 paginiChapter 9 KeySrinu WestÎncă nu există evaluări
- Bronchitis, Pneumonia and Bronchial Asthma in ChildrenDocument82 paginiBronchitis, Pneumonia and Bronchial Asthma in Childrenstrawberry pieÎncă nu există evaluări
- Well Fact Sheet: Suitability of Water For Livestock Fact SheetDocument2 paginiWell Fact Sheet: Suitability of Water For Livestock Fact SheetHill County Conservation DistrictÎncă nu există evaluări
- Example PT1 Backwards Planning - DeinstitutionalizationDocument8 paginiExample PT1 Backwards Planning - Deinstitutionalization213 212Încă nu există evaluări
- Viral HEPATITIS PPT by ApplemberDocument45 paginiViral HEPATITIS PPT by ApplemberEmpress ApplemberÎncă nu există evaluări
- Nitric Acid 70%Document10 paginiNitric Acid 70%Oscar ValdezÎncă nu există evaluări