S-ar putea să vă placă și
- Nonalcoholic Fatty Liver Disease (Nafld) Challenge To DiagnosisDocument31 paginiNonalcoholic Fatty Liver Disease (Nafld) Challenge To DiagnosisMohamed NaguibÎncă nu există evaluări
- Nutrition in the Chemo Chair: From an Oncology Dietitian’s PerspectiveDe la EverandNutrition in the Chemo Chair: From an Oncology Dietitian’s PerspectiveÎncă nu există evaluări
- MTAP 100 ASSESSMENT #2 Lipids and ProteinsDocument161 paginiMTAP 100 ASSESSMENT #2 Lipids and ProteinsRoselle Joyce Arce CalubanÎncă nu există evaluări
- Journal of Functional FoodsDocument11 paginiJournal of Functional FoodsChintya JessicaÎncă nu există evaluări
- Waist-to-Height Ratio Best Predicts DyslipidemiaDocument6 paginiWaist-to-Height Ratio Best Predicts DyslipidemiaFitri annisaÎncă nu există evaluări
- Goh - Excess Fat in The Abdomen - 2018Document6 paginiGoh - Excess Fat in The Abdomen - 2018MIRIAM VIDURRIZAGAÎncă nu există evaluări
- 74 Iajps74122019 PDFDocument7 pagini74 Iajps74122019 PDFiajpsÎncă nu există evaluări
- Lahav 2023Document9 paginiLahav 2023dyane VatriciaÎncă nu există evaluări
- CEREDA, 2013 - Anthropometric Indices of Fat Distribution and Cardiometabolic Risk in Parkinson's DiseaseDocument8 paginiCEREDA, 2013 - Anthropometric Indices of Fat Distribution and Cardiometabolic Risk in Parkinson's DiseaseAndressa BurgosÎncă nu există evaluări
- Fin 2104Document6 paginiFin 2104Prima Artya KurniawanÎncă nu există evaluări
- Fat Cell Size, Insulin Sensitivity, and Inflammation in Obese ChildrenDocument6 paginiFat Cell Size, Insulin Sensitivity, and Inflammation in Obese ChildrenwilmaÎncă nu există evaluări
- Extensive Weight Loss Reveals Distinct Gene Expression Changes in Human Subcutaneous and Visceral Adipose TissueDocument11 paginiExtensive Weight Loss Reveals Distinct Gene Expression Changes in Human Subcutaneous and Visceral Adipose TissueJulia SCÎncă nu există evaluări
- Leptin AscitesDocument5 paginiLeptin AscitesdonkeyendutÎncă nu există evaluări
- Surset Gastico 8Document2 paginiSurset Gastico 8Anonymous J6dN5VFDÎncă nu există evaluări
- Prediction of Liver Steatosis Applying A New Score in Subjects From The Brazilian Longitudinal Study of Adult HealthDocument10 paginiPrediction of Liver Steatosis Applying A New Score in Subjects From The Brazilian Longitudinal Study of Adult HealthtozinguedoÎncă nu există evaluări
- The Relationship Between Serum Bilirubin and Elevated Fibrotic Indices Among HBV Carriers: A Cross-Sectional Study of A Chinese PopulationDocument12 paginiThe Relationship Between Serum Bilirubin and Elevated Fibrotic Indices Among HBV Carriers: A Cross-Sectional Study of A Chinese PopulationRosiyahÎncă nu există evaluări
- Obesity Is Protective Factor in Hepatocellular.764Document1 paginăObesity Is Protective Factor in Hepatocellular.764marizaÎncă nu există evaluări
- Pancreatic Fat Deposition Is Increased and Related To Beta Cell Function in Women With Familial Partial LipodystrophyDocument6 paginiPancreatic Fat Deposition Is Increased and Related To Beta Cell Function in Women With Familial Partial LipodystrophyThiago AlfradiqueÎncă nu există evaluări
- Prediction of Future Gastric Cancer Risk Using A Machine Learning Algorithm and Comprehensive Medical Check-Up Data: A Case-Control StudyDocument9 paginiPrediction of Future Gastric Cancer Risk Using A Machine Learning Algorithm and Comprehensive Medical Check-Up Data: A Case-Control StudyAriani ArinÎncă nu există evaluări
- Ijbsv07p1003 PDFDocument13 paginiIjbsv07p1003 PDFDeedee RenovaldiÎncă nu există evaluări
- Diaz_Gomis_CN_HealthydietaryDocument9 paginiDiaz_Gomis_CN_HealthydietaryNoemy RodriguezÎncă nu există evaluări
- MSB 20188793 PDFDocument16 paginiMSB 20188793 PDFAndreea RoxanaÎncă nu există evaluări
- Waist Size, BMI, and Prostate Cancer RiskDocument7 paginiWaist Size, BMI, and Prostate Cancer Risktri1994Încă nu există evaluări
- Is Visceral Adiposity A Significant Correlate of Subcutaneous Adipose Cell Lipolysis in Men?Document7 paginiIs Visceral Adiposity A Significant Correlate of Subcutaneous Adipose Cell Lipolysis in Men?Zachary LeeÎncă nu există evaluări
- Direk 2013Document13 paginiDirek 2013Rafaela VeigaÎncă nu există evaluări
- A Low Carbohydrate, High Protein Diet Slows Tumor Growth and Prevents Cancer InitiationDocument11 paginiA Low Carbohydrate, High Protein Diet Slows Tumor Growth and Prevents Cancer Initiationanna.andreouu321Încă nu există evaluări
- The Liver: HST.035 Spring 2003Document35 paginiThe Liver: HST.035 Spring 2003miss illaÎncă nu există evaluări
- Associations of BMI With All-Cause MortalityDocument10 paginiAssociations of BMI With All-Cause MortalityainindyaÎncă nu există evaluări
- 2 A Canela Atenua A Adiposidade e Afeta A ExpressãoDocument11 pagini2 A Canela Atenua A Adiposidade e Afeta A Expressãoguto hdÎncă nu există evaluări
- Associations of Serum Fibroblast Growth Factor 23 Levels With Obesity and Visceral Fat Accumulation PDFDocument6 paginiAssociations of Serum Fibroblast Growth Factor 23 Levels With Obesity and Visceral Fat Accumulation PDFAkiko Syawalidhany TahirÎncă nu există evaluări
- Tchernof2013 PDFDocument46 paginiTchernof2013 PDFindahÎncă nu există evaluări
- IJBTR - Bio-tech-Studies On Leptin and MC4R Gene in Obese Population of South Western Province of Saudi Arabia Final ProofedDocument10 paginiIJBTR - Bio-tech-Studies On Leptin and MC4R Gene in Obese Population of South Western Province of Saudi Arabia Final ProofedTJPRC PublicationsÎncă nu există evaluări
- Obesity Control and Liver Health in Breast CancerDocument7 paginiObesity Control and Liver Health in Breast CancerMr XÎncă nu există evaluări
- tmpDDA TMPDocument7 paginitmpDDA TMPFrontiersÎncă nu există evaluări
- Obesity Phenotypes and Their Paradoxical Association With Cardiovascular DiseasesDocument64 paginiObesity Phenotypes and Their Paradoxical Association With Cardiovascular DiseasesIkke OppgaveÎncă nu există evaluări
- Review: Saint James School of Medicine, Albert Lake Drive, The Quarter A-1 2640, Anguilla, British West IndiesDocument15 paginiReview: Saint James School of Medicine, Albert Lake Drive, The Quarter A-1 2640, Anguilla, British West IndieslintangsrÎncă nu există evaluări
- Accepted Manuscript: Journal of HepatologyDocument31 paginiAccepted Manuscript: Journal of HepatologyNCÎncă nu există evaluări
- Animal 2Document20 paginiAnimal 2mahsagh7477Încă nu există evaluări
- #4 (Sofà A)Document6 pagini#4 (Sofà A)Sofia OrduñoÎncă nu există evaluări
- 1 s2.0 S0378512223004516 MainDocument9 pagini1 s2.0 S0378512223004516 MainTuyết mai ĐặngÎncă nu există evaluări
- Znu 00807000353Document7 paginiZnu 00807000353Amber FletchefÎncă nu există evaluări
- 1 s2.0 S1871402118303023 MainDocument7 pagini1 s2.0 S1871402118303023 MainLiliNurmawatiÎncă nu există evaluări
- Critical Reviews in Oncology / Hematology: F. Bozzetti, Z. Stanga TDocument12 paginiCritical Reviews in Oncology / Hematology: F. Bozzetti, Z. Stanga TshangrilaÎncă nu există evaluări
- Aumento Plasmático Dos Poluentes Advém Da Lipólise Subcutânea - IJO - 01Document7 paginiAumento Plasmático Dos Poluentes Advém Da Lipólise Subcutânea - IJO - 01Elenice Peltz NutricionistaÎncă nu există evaluări
- Seminario 9 ObesidadDocument11 paginiSeminario 9 Obesidadpau_sebÎncă nu există evaluări
- Fendo 11 00068Document9 paginiFendo 11 00068pelinÎncă nu există evaluări
- Liver Cirrhosis Research PapersDocument7 paginiLiver Cirrhosis Research Papersaflbmmmmy100% (1)
- Abstracts For The Website - pdf1441898071Document166 paginiAbstracts For The Website - pdf1441898071Radu MiricaÎncă nu există evaluări
- 07 MJN 24 (3) Nopphanath Et Al.Document10 pagini07 MJN 24 (3) Nopphanath Et Al.Egy SunandaÎncă nu există evaluări
- Diabetology & Metabolic Syndrome: Research Open AccessDocument11 paginiDiabetology & Metabolic Syndrome: Research Open AccessanonÎncă nu există evaluări
- graessler2012Document9 paginigraessler2012dora guzmanÎncă nu există evaluări
- Paretic Knee Extensor Energy Gait Pace and Also Body Fat Mass Are Generally Main Determining Factors Regarding Peak Aerobic Ability Within Subacute Cerebrovascular Event Observational Cohort ExaminenmdolDocument1 paginăParetic Knee Extensor Energy Gait Pace and Also Body Fat Mass Are Generally Main Determining Factors Regarding Peak Aerobic Ability Within Subacute Cerebrovascular Event Observational Cohort Examinenmdolsantasoap65Încă nu există evaluări
- Lipid Disturbances in Breast Cancer Patients During ChemotherapyDocument11 paginiLipid Disturbances in Breast Cancer Patients During ChemotherapySteve GannabanÎncă nu există evaluări
- Nutrients 16 00846Document13 paginiNutrients 16 00846Vianey Rios CarbajalÎncă nu există evaluări
- Article 1Document13 paginiArticle 1samanÎncă nu există evaluări
- Met 2019 0059Document6 paginiMet 2019 0059raihannah othmanÎncă nu există evaluări
- Obesity - StatPearls - NCBI BookshelfDocument8 paginiObesity - StatPearls - NCBI BookshelfWidad SalsabilaÎncă nu există evaluări
- 28Jul2020CIJF 2020 0562 - ManuscriptDocument29 pagini28Jul2020CIJF 2020 0562 - ManuscriptGarvita KharbandaÎncă nu există evaluări
- EPICDocument6 paginiEPICVanesa GonzalezÎncă nu există evaluări
- Metabolic Syndrome XDocument11 paginiMetabolic Syndrome XAndres RiveraÎncă nu există evaluări
- Shi 2023 Ic 230059 1683052065.2246Document3 paginiShi 2023 Ic 230059 1683052065.2246Melchorita stephanie Nuñez CordovaÎncă nu există evaluări
- HIV Infection and Cardiovascular Diseases The Obnoxious DuosDocument5 paginiHIV Infection and Cardiovascular Diseases The Obnoxious DuosKIU PUBLICATION AND EXTENSIONÎncă nu există evaluări
- Science 10 Q4 M8Document14 paginiScience 10 Q4 M8Kuerth Vinluan100% (1)
- Bantolinao, Liezl Dawn Entuna 2246018715Document2 paginiBantolinao, Liezl Dawn Entuna 2246018715shyÎncă nu există evaluări
- Hyperlipidemia 1. PathophysiologyDocument2 paginiHyperlipidemia 1. PathophysiologyGlyneth FranciaÎncă nu există evaluări
- MED TECH Clinical ChemistryDocument3 paginiMED TECH Clinical ChemistryJan Martin Mogueis JustoÎncă nu există evaluări
- Running As A Key Lifestyle Medicine For LongevityDocument11 paginiRunning As A Key Lifestyle Medicine For LongevityKhang T. NguyenÎncă nu există evaluări
- Antioxidant and Lipid Lowering Effects of Elaeocarpus Ganitrus in Cholesterol Fed RabbitsDocument9 paginiAntioxidant and Lipid Lowering Effects of Elaeocarpus Ganitrus in Cholesterol Fed RabbitsKuberBajgainÎncă nu există evaluări
- Art 1Document12 paginiArt 1Irene Ramirez ChavesÎncă nu există evaluări
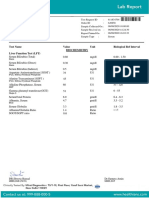
- Test Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Document7 paginiTest Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Himanshu GarkhelÎncă nu există evaluări
- Sona.M:::: Patient Age / Sex 40 Y / Female BranchDocument7 paginiSona.M:::: Patient Age / Sex 40 Y / Female Branchsuresh babujiÎncă nu există evaluări
- Statins Meta-AnalysisDocument180 paginiStatins Meta-AnalysisKiaraÎncă nu există evaluări
- Yoga & HypothyroidismDocument6 paginiYoga & Hypothyroidismtttt45Încă nu există evaluări
- Etnobotani Daun Afrika Dan BioaktivitasnyaDocument26 paginiEtnobotani Daun Afrika Dan BioaktivitasnyaAsgarPurnamaÎncă nu există evaluări
- SP10046667Document17 paginiSP10046667santoshÎncă nu există evaluări
- Met 2008 0065 PDFDocument10 paginiMet 2008 0065 PDFDeedee RenovaldiÎncă nu există evaluări
- 6/22/2011 Classification of Lipids 1Document51 pagini6/22/2011 Classification of Lipids 1DrBasavarajÎncă nu există evaluări
- Effect ModificationDocument64 paginiEffect ModificationDani Yitu MedanituÎncă nu există evaluări
- Ερωτήσεις διάφορεςDocument108 paginiΕρωτήσεις διάφορεςyiafkaÎncă nu există evaluări
- 25 Steps To Take To Prevent AlzheimerDocument9 pagini25 Steps To Take To Prevent AlzheimerRatnaPrasadNalamÎncă nu există evaluări
- Treatment of Hyperlipidemias: Pharmacology TeamDocument53 paginiTreatment of Hyperlipidemias: Pharmacology TeamZaina Masri100% (1)
- Presentation 1Document36 paginiPresentation 1Alice Chews IceÎncă nu există evaluări
- Normal Weight Obesity SyndromeDocument13 paginiNormal Weight Obesity SyndromeMarcelo SabbatiniÎncă nu există evaluări
- Unit 5 TransDocument11 paginiUnit 5 TransGrace FernandoÎncă nu există evaluări
- Antihyperlipidemic Agents: Phar406 Pharmaceutical Chemistry Iv Emu-Spring TermDocument55 paginiAntihyperlipidemic Agents: Phar406 Pharmaceutical Chemistry Iv Emu-Spring TermN. IndupriyaÎncă nu există evaluări
- Is Ghee Bad For CholesterolDocument1 paginăIs Ghee Bad For CholesterolSsr RaoÎncă nu există evaluări
- Chemical, Technological and Biochemical Studies of Purslane LeavesDocument12 paginiChemical, Technological and Biochemical Studies of Purslane LeavesSulistia MuarifaÎncă nu există evaluări
- Anti-Hyperlipidemic Effect of Aqueous Leaf Extract of Emilia Praetermissa Milne-Redh (Asteraceae) in RatsDocument10 paginiAnti-Hyperlipidemic Effect of Aqueous Leaf Extract of Emilia Praetermissa Milne-Redh (Asteraceae) in RatsInternational Network For Natural Sciences100% (1)
- Effect of Honey Bee Venom Apis Mellifera On Hyperglycemia and Hyperlipidemia in Alloxan Induced Diabetic Rabbits 2155 6156.1000507Document4 paginiEffect of Honey Bee Venom Apis Mellifera On Hyperglycemia and Hyperlipidemia in Alloxan Induced Diabetic Rabbits 2155 6156.1000507Solongo GanboldÎncă nu există evaluări
- JN2022819 26Document19 paginiJN2022819 26goutham an rajaÎncă nu există evaluări