S-ar putea să vă placă și
- Aaos 2010Document220 paginiAaos 2010Yusufa ArdyÎncă nu există evaluări
- Case Based AnesDocument251 paginiCase Based AnesRDÎncă nu există evaluări
- PDFDocument286 paginiPDFLia CorneliaÎncă nu există evaluări
- Nabh Standards For Small Healthcare Organisations: Satndards SummaryDocument7 paginiNabh Standards For Small Healthcare Organisations: Satndards SummaryPrabhat KumarÎncă nu există evaluări
- Practice CPC Exam - Coding Certification Tips (PDFDrive)Document18 paginiPractice CPC Exam - Coding Certification Tips (PDFDrive)Sai SmaranÎncă nu există evaluări
- The Osseous Genioplasty: Clinicsin Plastic SurgeryDocument16 paginiThe Osseous Genioplasty: Clinicsin Plastic SurgeryRajan KarmakarÎncă nu există evaluări
- Thoracic Endoscopic Spine Surgery A ComprehensiveDocument11 paginiThoracic Endoscopic Spine Surgery A Comprehensivesanjay chhawraÎncă nu există evaluări
- Panduan Praktik Klinis (PPK) Prosedur Tindakan/Operasi Bedah Orthopedik Rsup Fatmawati Jakarta 2014 - 2016Document2 paginiPanduan Praktik Klinis (PPK) Prosedur Tindakan/Operasi Bedah Orthopedik Rsup Fatmawati Jakarta 2014 - 2016Arbianti AstutiÎncă nu există evaluări
- (10920684 - Neurosurgical Focus) Percutaneous Pedicle Screw Fixation of The Lumbar SpineDocument9 pagini(10920684 - Neurosurgical Focus) Percutaneous Pedicle Screw Fixation of The Lumbar Spineefancoolhand09Încă nu există evaluări
- JCM 10 02422 v2Document10 paginiJCM 10 02422 v2DR SUNIL SINGHÎncă nu există evaluări
- IndianJAnaesth6311924-2183535 060355Document8 paginiIndianJAnaesth6311924-2183535 060355Abhijeet ThakurÎncă nu există evaluări
- Real-Time Ultrasound-Guided Paramedian Epidural Access: Evaluation of A Novel In-Plane TechniqueDocument10 paginiReal-Time Ultrasound-Guided Paramedian Epidural Access: Evaluation of A Novel In-Plane TechniqueANGELICAÎncă nu există evaluări
- Ultrasound-Guided Truncal Blocks For PerioperativeDocument15 paginiUltrasound-Guided Truncal Blocks For PerioperativeRuxandra GrigorescuÎncă nu există evaluări
- Lateral Supraorbital Approach Vs Pterional Approach: An Anatomic Qualitative and Quantitative EvaluationDocument9 paginiLateral Supraorbital Approach Vs Pterional Approach: An Anatomic Qualitative and Quantitative EvaluationMartina javiera Alarcon AcevedoÎncă nu există evaluări
- Quantitative Anatomical Comparison of Anterior, Anterolateral and Lateral, Microsurgical and Endoscopic Approaches To The Middle Cranial FossaDocument49 paginiQuantitative Anatomical Comparison of Anterior, Anterolateral and Lateral, Microsurgical and Endoscopic Approaches To The Middle Cranial FossaAndrés BotelloÎncă nu există evaluări
- 4 IndianJAnaesth617581-2226112 - 061101Document6 pagini4 IndianJAnaesth617581-2226112 - 061101Mythology KingdomÎncă nu există evaluări
- Abat F. 2019. Comparison US Guided vs. Blind Interventions Supraspinatus TendinopathyDocument10 paginiAbat F. 2019. Comparison US Guided vs. Blind Interventions Supraspinatus TendinopathyJavier MartinÎncă nu există evaluări
- My Published Paper 6, AnesthesiaDocument5 paginiMy Published Paper 6, Anesthesiamir sahirÎncă nu există evaluări
- Comparison of Pre Procedural and Real Time Ultrasound Guided Spinal Anesthesia For Traumatic Lower Limb InjuryDocument7 paginiComparison of Pre Procedural and Real Time Ultrasound Guided Spinal Anesthesia For Traumatic Lower Limb InjuryIJAR JOURNALÎncă nu există evaluări
- Ease of Lumbar Epidural Catheter Insertion With.11Document5 paginiEase of Lumbar Epidural Catheter Insertion With.11jagadish aÎncă nu există evaluări
- H Outcomes of Total Knee Arthroplasty in Degenerative Osteoarthritic Knee With Genu RecurvatumDocument10 paginiH Outcomes of Total Knee Arthroplasty in Degenerative Osteoarthritic Knee With Genu RecurvatumYuji AibÎncă nu există evaluări
- Yoshida Proximal Obturator Nerve BlockDocument7 paginiYoshida Proximal Obturator Nerve BlockFACULTY FOLDERSÎncă nu există evaluări
- Sebastian Ruetten, MD, PHD, Martin Komp, MD, PHD, and Georgios Godolias, MD, ProfDocument9 paginiSebastian Ruetten, MD, PHD, Martin Komp, MD, PHD, and Georgios Godolias, MD, ProfKaustubh KeskarÎncă nu există evaluări
- Regional AnalgesiaDocument5 paginiRegional AnalgesiajdjhdÎncă nu există evaluări
- Percutaneous Computed-Tomography-Guided Biopsy of The Spine: 229 ProceduresDocument6 paginiPercutaneous Computed-Tomography-Guided Biopsy of The Spine: 229 ProceduresMarcelo MudoÎncă nu există evaluări
- Effects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric StudyDocument8 paginiEffects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric Studysiti hanifahÎncă nu există evaluări
- Percutaneous Ultrasound Guided Versus Open Cut Down Access To Femoral Vessels For The Placement of A REBOA CatheterDocument7 paginiPercutaneous Ultrasound Guided Versus Open Cut Down Access To Femoral Vessels For The Placement of A REBOA CatheterNormanÎncă nu există evaluări
- Posterior Lumbar Interbody Fusion (PLIF) With Cages and Local Bone Graft in The Treatment of Spinal StenosisDocument7 paginiPosterior Lumbar Interbody Fusion (PLIF) With Cages and Local Bone Graft in The Treatment of Spinal StenosisMd.Shafiul EzazÎncă nu există evaluări
- Perioperative Point-of-Care Ultrasonography: The Past and The Future Are in Anesthesiologists' HandsDocument3 paginiPerioperative Point-of-Care Ultrasonography: The Past and The Future Are in Anesthesiologists' HandsSyahrul Mubarak Danar SumantriÎncă nu există evaluări
- JOurnal Uro 2Document6 paginiJOurnal Uro 2Gladys AilingÎncă nu există evaluări
- Basic Arthroplasty - Unit 4 - Ext Mech Allograft BurnettDocument21 paginiBasic Arthroplasty - Unit 4 - Ext Mech Allograft BurnettShu Yang HuÎncă nu există evaluări
- J Wneu 2019 05 148Document11 paginiJ Wneu 2019 05 148Cristian OñateÎncă nu există evaluări
- Total Knee Replacement Modifies The Preoperative Tibial Torsion Angle - Similar Results Between Computer-Assisted and Standard TechniqueDocument9 paginiTotal Knee Replacement Modifies The Preoperative Tibial Torsion Angle - Similar Results Between Computer-Assisted and Standard TechniqueJoko TriwardonoÎncă nu există evaluări
- ASA Regional AnesthesiaDocument10 paginiASA Regional Anesthesiayessy32lÎncă nu există evaluări
- Double Bundle PCL Technique and Outcomes 2011Document8 paginiDouble Bundle PCL Technique and Outcomes 2011hieuminhduong7Încă nu există evaluări
- Ultrasoud Guidance For Lumbar PunctureDocument12 paginiUltrasoud Guidance For Lumbar PunctureDavid Avellaneda TalledoÎncă nu există evaluări
- PIIS1529943021008196Document11 paginiPIIS1529943021008196Juan Carlos del ReyÎncă nu există evaluări
- 10 1016@j Jclinane 2019 04 037Document2 pagini10 1016@j Jclinane 2019 04 037Nitin HayaranÎncă nu există evaluări
- Airway Management Using UltrasoundDocument7 paginiAirway Management Using Ultrasoundroflova1908Încă nu există evaluări
- Arthroscopic Treatment of Anterosuperior Rotator CDocument8 paginiArthroscopic Treatment of Anterosuperior Rotator CGabriel RojasÎncă nu există evaluări
- Comparative Anatomical Analysis of The Transcallosal-Transchoroidal and Transcallosal-Transforniceal-Transchoroidal Approaches To The Third VentricleDocument10 paginiComparative Anatomical Analysis of The Transcallosal-Transchoroidal and Transcallosal-Transforniceal-Transchoroidal Approaches To The Third VentricleZeptalanÎncă nu există evaluări
- Haglund's Syndrome Schneider2000Document5 paginiHaglund's Syndrome Schneider2000emrahaltuntasÎncă nu există evaluări
- 2017 Results of Endoscopically-Assisted Cubital Tunnel Release Without Using Any Specific InstrumentDocument4 pagini2017 Results of Endoscopically-Assisted Cubital Tunnel Release Without Using Any Specific InstrumentDimitris RodriguezÎncă nu există evaluări
- Abdallah 2017 PCL Avulsion OpenDocument6 paginiAbdallah 2017 PCL Avulsion Openshafia bunga nayradinaÎncă nu există evaluări
- Clinical and Radiological Outcomes of Osteoarth 2019 Orthopaedics TraumatoDocument6 paginiClinical and Radiological Outcomes of Osteoarth 2019 Orthopaedics TraumatodrelvÎncă nu există evaluări
- Journal Homepage: - : IntroductionDocument7 paginiJournal Homepage: - : IntroductionIJAR JOURNALÎncă nu există evaluări
- 6Document8 pagini6Mihai PopescuÎncă nu există evaluări
- Article PDFDocument9 paginiArticle PDFAqsa FarooqÎncă nu există evaluări
- Touhy y CateterDocument8 paginiTouhy y CateterhumildementeanestesiosÎncă nu există evaluări
- 10 1016@j Arthro 2006 07 006Document8 pagini10 1016@j Arthro 2006 07 006YoshitaÎncă nu există evaluări
- Comparison of Isocentric C-Arm 3-DimensionaDocument7 paginiComparison of Isocentric C-Arm 3-Dimensionagevowo3277Încă nu există evaluări
- Vascular Access: The Impact of Ultrasonography: Acesso Vascular: o Impacto Da UltrassonografiaDocument6 paginiVascular Access: The Impact of Ultrasonography: Acesso Vascular: o Impacto Da UltrassonografiaLatescu ConstantinÎncă nu există evaluări
- An Accurate Full-Flexion Anterolateral Portal For Needle Placement in The Knee Joint With Dry OsteoarthritisDocument7 paginiAn Accurate Full-Flexion Anterolateral Portal For Needle Placement in The Knee Joint With Dry OsteoarthritisOthoniel RamirezÎncă nu există evaluări
- Avoidance of Wrong-Level Thoracic Spine Surgery: Intraoperative Localization With Preoperative PercutaneousDocument5 paginiAvoidance of Wrong-Level Thoracic Spine Surgery: Intraoperative Localization With Preoperative PercutaneousWinnie LiÎncă nu există evaluări
- Comparison of Joint Perception Between Posterior-Stabilized and Ultracongruent Total Knee Arthroplasty in The Same PatientDocument9 paginiComparison of Joint Perception Between Posterior-Stabilized and Ultracongruent Total Knee Arthroplasty in The Same PatientNuno PaisÎncă nu există evaluări
- Improved Accuracy of Component PositioningDocument9 paginiImproved Accuracy of Component Positioningswastik baratÎncă nu există evaluări
- SurgicalTipsandTricksDuringUrethroplastyforBulbarUrethralStricturesFocusingonAccurateLocalisationoftheStricture ResultsfromaTertiaryCentreDocument8 paginiSurgicalTipsandTricksDuringUrethroplastyforBulbarUrethralStricturesFocusingonAccurateLocalisationoftheStricture ResultsfromaTertiaryCentreTomek RÎncă nu există evaluări
- Continuous Pericapsular Nerve Group Block For Hip Surgery: A Case SeriesDocument17 paginiContinuous Pericapsular Nerve Group Block For Hip Surgery: A Case SeriesVivek Vishal SahÎncă nu există evaluări
- Nerve-Sparing Radical Hysterectomy in Cervical CancerDocument6 paginiNerve-Sparing Radical Hysterectomy in Cervical CancerdenisdeniÎncă nu există evaluări
- Intramedullary Control of Distal Femoral Resection Results in Precise Coronal Alignment in TKADocument7 paginiIntramedullary Control of Distal Femoral Resection Results in Precise Coronal Alignment in TKAAsmed El SalugÎncă nu există evaluări
- The Modified Brostr M Gould Procedure - Early Results Usi - 2014 - Foot and AnklDocument5 paginiThe Modified Brostr M Gould Procedure - Early Results Usi - 2014 - Foot and AnklFyodorovich Makarov NikolaiÎncă nu există evaluări
- Fluoroscopic Analysis of The Kinematics of Deep Exion in Total Knee ArthroplastyDocument4 paginiFluoroscopic Analysis of The Kinematics of Deep Exion in Total Knee Arthroplastyjmhinos4833Încă nu există evaluări
- What Should We Be Careful of Ankle Arthroscopy?: or Thopaedic Surger yDocument9 paginiWhat Should We Be Careful of Ankle Arthroscopy?: or Thopaedic Surger yJaysellePuguonTabijeÎncă nu există evaluări
- Spinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDocument5 paginiSpinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDella Puspita SariÎncă nu există evaluări
- Lateral Oblique Superior To Lateral View CESI 2015Document14 paginiLateral Oblique Superior To Lateral View CESI 2015Michael HuntÎncă nu există evaluări
- Endoscopic Procedures on the SpineDe la EverandEndoscopic Procedures on the SpineJin-Sung KimÎncă nu există evaluări
- Dr. Nasir: Curriculum VitaeDocument15 paginiDr. Nasir: Curriculum VitaeJoshua BoltonÎncă nu există evaluări
- Small Animal Surgical Nursing: Skills and Concepts, 2006, 413 Pages, Sara J. Busch, 0323030637, 9780323030632, Elsevier Mosby, 2006Document19 paginiSmall Animal Surgical Nursing: Skills and Concepts, 2006, 413 Pages, Sara J. Busch, 0323030637, 9780323030632, Elsevier Mosby, 2006mdmostafiz446Încă nu există evaluări
- Analgesia en ObstetriciaDocument21 paginiAnalgesia en ObstetriciaSERGIO VERGEL MANTILLAÎncă nu există evaluări
- Test Bank For Alexanders Surgical Procedures 1st Edition RothrockDocument36 paginiTest Bank For Alexanders Surgical Procedures 1st Edition Rothrockgestleucinice197e100% (33)
- Richter's Sacrospinous FixationDocument13 paginiRichter's Sacrospinous FixationChopin SripramodyaÎncă nu există evaluări
- GO (P) No70 2022 FinDated23 06 2022 - 45Document96 paginiGO (P) No70 2022 FinDated23 06 2022 - 45Manju AlexÎncă nu există evaluări
- NCP TahbsoDocument18 paginiNCP TahbsoUzziah Dharambai GurbuxaniÎncă nu există evaluări
- High Output Stoma Management 2011 PDFDocument6 paginiHigh Output Stoma Management 2011 PDFLutfi AhmadÎncă nu există evaluări
- My Final ReportDocument78 paginiMy Final ReportjhutayÎncă nu există evaluări
- Masquelet Technique A Systematic Review 30 YearsDocument2 paginiMasquelet Technique A Systematic Review 30 YearsKlausÎncă nu există evaluări
- Cost Estimate Form: PatientDocument1 paginăCost Estimate Form: PatientranapÎncă nu există evaluări
- 3rd Sarawak Burn Update FlyerDocument2 pagini3rd Sarawak Burn Update FlyerCY DingÎncă nu există evaluări
- Health Econ BibDocument262 paginiHealth Econ BibAhmed HassanÎncă nu există evaluări
- Liver Abscess Medication - Antibiotics, Antifungal AgentsDocument2 paginiLiver Abscess Medication - Antibiotics, Antifungal AgentsAdi KurniaÎncă nu există evaluări
- Case StudyDocument7 paginiCase StudyMotilaldass100% (1)
- Meeting 10 - Rismawati 190106126Document3 paginiMeeting 10 - Rismawati 190106126RismawatiÎncă nu există evaluări
- Lista de Revista de HINARI 2010Document182 paginiLista de Revista de HINARI 2010Miguel AlcaÎncă nu există evaluări
- Comprehensive Specialities With The Finest Consultants: Paediatric SurgeryDocument2 paginiComprehensive Specialities With The Finest Consultants: Paediatric SurgeryKapil PatwaÎncă nu există evaluări
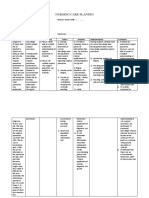
- Nursing Care PlaningDocument3 paginiNursing Care PlaningSudin SamÎncă nu există evaluări
- Bier's Block (Intravenous Regional Anesthesia)Document10 paginiBier's Block (Intravenous Regional Anesthesia)s.alisufyaanÎncă nu există evaluări
- Nursing Resume - Samples & How To Guide PDFDocument2 paginiNursing Resume - Samples & How To Guide PDFEsther Tellez NavarreteÎncă nu există evaluări
- 1 Jyothi Sanjeevini Full DetailsDocument161 pagini1 Jyothi Sanjeevini Full DetailsPramodÎncă nu există evaluări
- HDFC Ie Delhi 07 05 2020 PDFDocument16 paginiHDFC Ie Delhi 07 05 2020 PDFAmit SinghÎncă nu există evaluări
- Module 2. EntrepreneurshipDocument11 paginiModule 2. EntrepreneurshipLangpaoen, Frejobel E.Încă nu există evaluări