S-ar putea să vă placă și
- Journal 4Document5 paginiJournal 4dr. Nadia Salsabila100% (1)
- Jurnal BedahDocument3 paginiJurnal BedahAb Hakim MuslimÎncă nu există evaluări
- An Atypical Esthesioneuroblastoma of The Sphenoid Sinus A Case ReportDocument4 paginiAn Atypical Esthesioneuroblastoma of The Sphenoid Sinus A Case ReportInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Mediastinal Abscess After EndobronchialDocument3 paginiMediastinal Abscess After EndobronchialDm LdÎncă nu există evaluări
- Anaesthesia Management in Endoscopic Ultrasound Guided Lung BiopsyDocument2 paginiAnaesthesia Management in Endoscopic Ultrasound Guided Lung BiopsyInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Preprint Not Peer Reviewed: Corresponding AuthorDocument14 paginiPreprint Not Peer Reviewed: Corresponding AuthorАмина ПлотноваÎncă nu există evaluări
- Bronchial and Arterial Sleeve Resection For Centrally-Located Lung CancersDocument10 paginiBronchial and Arterial Sleeve Resection For Centrally-Located Lung CancersJovelyn SagangÎncă nu există evaluări
- Bronchial Artery Pseudoaneurysm and Mediast - 2021 - Archivos de BronconeumologDocument2 paginiBronchial Artery Pseudoaneurysm and Mediast - 2021 - Archivos de BronconeumologMomoh GaiusÎncă nu există evaluări
- BIBL 12 Liver MetastasisDocument3 paginiBIBL 12 Liver Metastasisstoia_sebiÎncă nu există evaluări
- Asthma: Further ReadingDocument13 paginiAsthma: Further ReadingcarlosÎncă nu există evaluări
- 2017 Renal Cell Carcinoma Metastasis To The Vocal Cord A Case ReportDocument5 pagini2017 Renal Cell Carcinoma Metastasis To The Vocal Cord A Case ReportAlfonsoSánchezÎncă nu există evaluări
- LungDocument5 paginiLungWafa MediÎncă nu există evaluări
- Asian Journal of Anesthesiology: K.M. Lai, M.H. Hsieh, F. Lam, C.Y. Chen, T.L. Chen, C.C. ChangDocument2 paginiAsian Journal of Anesthesiology: K.M. Lai, M.H. Hsieh, F. Lam, C.Y. Chen, T.L. Chen, C.C. ChangSyamsi KubangunÎncă nu există evaluări
- 全肺袖状切除术的适应证和技巧Document12 pagini全肺袖状切除术的适应证和技巧paul WhooÎncă nu există evaluări
- Mondoni Et AlDocument11 paginiMondoni Et AlpandylouisputraÎncă nu există evaluări
- A Systematic Review of Sinonasal Oncocytomas and Oncocytic Carcinomas: Diagnosis, Management, and Technical ConsiderationsDocument11 paginiA Systematic Review of Sinonasal Oncocytomas and Oncocytic Carcinomas: Diagnosis, Management, and Technical ConsiderationsInes Camilla PutriÎncă nu există evaluări
- Treatment Cysts: Thoracoscopic PleuropericardialDocument8 paginiTreatment Cysts: Thoracoscopic PleuropericardialJuhi SahajwaniÎncă nu există evaluări
- Endobronchial Ultrasound: What Is It and When Should It Be Used?Document6 paginiEndobronchial Ultrasound: What Is It and When Should It Be Used?Legenda AkÎncă nu există evaluări
- Respiratory Medicine Case Reports: SciencedirectDocument4 paginiRespiratory Medicine Case Reports: SciencedirectrodtobingÎncă nu există evaluări
- Relato Caso de Hpe Intra CapsularDocument5 paginiRelato Caso de Hpe Intra Capsularalbertofigueiredo_14Încă nu există evaluări
- Lung Adenocarcinoma With Solitary MetastDocument88 paginiLung Adenocarcinoma With Solitary MetastMikmik bay BayÎncă nu există evaluări
- The Role of Endoscopic Biopsy and Third Ventriculostomy in TheDocument8 paginiThe Role of Endoscopic Biopsy and Third Ventriculostomy in TheCarlos Daniel Giménez MéndezÎncă nu există evaluări
- RadiopediaDocument4 paginiRadiopediakennyÎncă nu există evaluări
- Histopathologic Analysis of Ct-Guided Core Needle Biopsy in Radiologically Detected Suspicious Mediastinal and Lung Mass: Two Years' Study in Tertiary HospitalDocument4 paginiHistopathologic Analysis of Ct-Guided Core Needle Biopsy in Radiologically Detected Suspicious Mediastinal and Lung Mass: Two Years' Study in Tertiary HospitalDesiree MejicaÎncă nu există evaluări
- Hyareetal 2010Document9 paginiHyareetal 2010DanielMahendraÎncă nu există evaluări
- Orbital Metastasis of A Pediatric Nasopharyngeal Carcinoma A Rare Case ReportDocument4 paginiOrbital Metastasis of A Pediatric Nasopharyngeal Carcinoma A Rare Case ReportInternational Journal of Innovative Science and Research Technology100% (1)
- Ojolns-11 Issue-II F Color - P 11-14-Solitary Fibrous Tumors of The Nose and Paranasal Sinuses-Our ExperienceDocument4 paginiOjolns-11 Issue-II F Color - P 11-14-Solitary Fibrous Tumors of The Nose and Paranasal Sinuses-Our ExperienceDipak Ranjan NayakÎncă nu există evaluări
- NCM 112: (Surgery, CD, I&I, Cellular Aberration) : Lung Cancer (Document8 paginiNCM 112: (Surgery, CD, I&I, Cellular Aberration) : Lung Cancer (Jamaicah N. NagaÎncă nu există evaluări
- 2019 Article 889Document4 pagini2019 Article 889ErickÎncă nu există evaluări
- J.Operative Approaches To The Pineal Region Tumors.1998Document4 paginiJ.Operative Approaches To The Pineal Region Tumors.1998Kysy CodonÎncă nu există evaluări
- 2008 Chest - The Blue ProtocolDocument9 pagini2008 Chest - The Blue Protocoleduardo0% (1)
- US Pulmón para Manejo de Atelectasias PerioperatoriasDocument11 paginiUS Pulmón para Manejo de Atelectasias PerioperatoriasJURAGOMAÎncă nu există evaluări
- Routine Use of Point-of-Care Lung Ultrasound During The COVID-19 PandemicDocument4 paginiRoutine Use of Point-of-Care Lung Ultrasound During The COVID-19 PandemicOswaldo MontesÎncă nu există evaluări
- Aspecto Linfonodal Fujiwara 2010Document7 paginiAspecto Linfonodal Fujiwara 2010VickÎncă nu există evaluări
- Pneumomediastinum, Pneumoretroperitoneum, Pneumoperitoneum and Subcutaneous Emphysema Secondary To A Penetrating Anal InjuryDocument6 paginiPneumomediastinum, Pneumoretroperitoneum, Pneumoperitoneum and Subcutaneous Emphysema Secondary To A Penetrating Anal InjuryMing-Jen TsaiÎncă nu există evaluări
- Thesis Endobronchial UltrasoundDocument4 paginiThesis Endobronchial Ultrasoundafknikfgd100% (2)
- Central Airway TumorDocument9 paginiCentral Airway TumorYanuar AbdulhayÎncă nu există evaluări
- Metastatic Spread of Primary Lung Adenocarcino - 2024 - International Journal ofDocument5 paginiMetastatic Spread of Primary Lung Adenocarcino - 2024 - International Journal ofRonald QuezadaÎncă nu există evaluări
- A Rare Case of Bilateral Adrenocortical Carcinoma With Metastasis in A Young MaleDocument3 paginiA Rare Case of Bilateral Adrenocortical Carcinoma With Metastasis in A Young MaleDixit VarmaÎncă nu există evaluări
- 5725-Article Text-20053-1-10-20210320Document3 pagini5725-Article Text-20053-1-10-20210320Rafael BagusÎncă nu există evaluări
- Peripheral Primitive Neuro-Ectodermal Tumor of The Pleura About A Rare Caser, With Literature ReviewDocument4 paginiPeripheral Primitive Neuro-Ectodermal Tumor of The Pleura About A Rare Caser, With Literature ReviewInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Transluminal Endoscopic Necrosectomy After Acute Pancreatitis: A Multicentre Study With Long-Term Follow-Up (The GEPARD Study)Document8 paginiTransluminal Endoscopic Necrosectomy After Acute Pancreatitis: A Multicentre Study With Long-Term Follow-Up (The GEPARD Study)victorÎncă nu există evaluări
- Difficult Intubation and Anesthetic Management in An Adult Patient With Undiagnosed Congenital Tracheal Stenosis: A Case ReportDocument6 paginiDifficult Intubation and Anesthetic Management in An Adult Patient With Undiagnosed Congenital Tracheal Stenosis: A Case ReportBianca CaterinalisendraÎncă nu există evaluări
- Fulltext Ajo v2 Id1026Document3 paginiFulltext Ajo v2 Id1026Lavenia Ellein MokiwangÎncă nu există evaluări
- 2000 Metastatic Renal Cell Carcinoma To The Head and Neck AreaDocument3 pagini2000 Metastatic Renal Cell Carcinoma To The Head and Neck AreaAlfonsoSánchezÎncă nu există evaluări
- Motas2018 Pleural Diseases On Single Lung After Pneumonectomy For CancerDocument1 paginăMotas2018 Pleural Diseases On Single Lung After Pneumonectomy For CancerAlin Ionut BurlacuÎncă nu există evaluări
- IPMN Versus Ampullary AdenomaDocument6 paginiIPMN Versus Ampullary AdenomaedwardÎncă nu există evaluări
- Adenoma 2020Document11 paginiAdenoma 2020Residentes AudiologiaÎncă nu există evaluări
- Pulmonary Pseudotumoral Tuberculosis in An Old Man: A Rare PresentationDocument3 paginiPulmonary Pseudotumoral Tuberculosis in An Old Man: A Rare PresentationNurhasanahÎncă nu există evaluări
- Pedunculated Parietal Pleural Lesion A RDocument2 paginiPedunculated Parietal Pleural Lesion A RBhanu PratapÎncă nu există evaluări
- Minimally Invasive Thoracic SurgeryDocument9 paginiMinimally Invasive Thoracic SurgeryLEONEL ALFREDO GUILLEN MARINÎncă nu există evaluări
- Nekrotik UsgDocument5 paginiNekrotik UsgHeru SigitÎncă nu există evaluări
- Edoskopi FleksibelDocument4 paginiEdoskopi FleksibelDex RayÎncă nu există evaluări
- Transaereolar Pulmonary BullectomyDocument7 paginiTransaereolar Pulmonary BullectomyAhmad Ibrahim RumÎncă nu există evaluări
- A Case Series On Olfactory NeuroblastomaDocument4 paginiA Case Series On Olfactory NeuroblastomaIJAR JOURNALÎncă nu există evaluări
- Blunt Bronchial InjuriesDocument3 paginiBlunt Bronchial InjuriesaizatamlikhaÎncă nu există evaluări
- Endobronchial Ultrasound For The Diagnosis and Staging of Lung Cancer (Methods)Document7 paginiEndobronchial Ultrasound For The Diagnosis and Staging of Lung Cancer (Methods)Gio Mari MarcialÎncă nu există evaluări
- Laryngeal Tuberculosis: An Uncommon But Important Cause of OdynophagiaDocument3 paginiLaryngeal Tuberculosis: An Uncommon But Important Cause of OdynophagiaSkripsi ParasitologiÎncă nu există evaluări
- WJCC 7 2623Document8 paginiWJCC 7 2623Gisela LalitaÎncă nu există evaluări
- Thoracic Endoscopy: Advances in Interventional PulmonologyDe la EverandThoracic Endoscopy: Advances in Interventional PulmonologyMichael J. SimoffÎncă nu există evaluări
- HC PDFDocument428 paginiHC PDFnetemma97Încă nu există evaluări
- Real MadridDocument3 paginiReal MadridNarendran SureshÎncă nu există evaluări
- Changing Trends and Career in Physical EducationDocument22 paginiChanging Trends and Career in Physical Educationrksavita719Încă nu există evaluări
- How To Style Men's Track PantsDocument2 paginiHow To Style Men's Track PantsClassic Polo eComÎncă nu există evaluări
- Umaid Bhawan JodhpurDocument7 paginiUmaid Bhawan JodhpurRamya SarangÎncă nu există evaluări
- ScaniaPartsSolutions2020Brochure A5 V13Document21 paginiScaniaPartsSolutions2020Brochure A5 V13கோவி கோபால் ஆர்ட்ஸ்Încă nu există evaluări
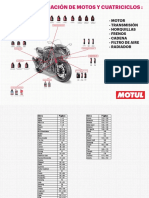
- Guía de Lubricación Motos, Cuatricilos y Motos de AguaDocument194 paginiGuía de Lubricación Motos, Cuatricilos y Motos de AguaJuanÎncă nu există evaluări
- KG 020Document2 paginiKG 020EricÎncă nu există evaluări
- ArnisDocument2 paginiArnisAndrea Mae P. PalmeroÎncă nu există evaluări
- Normal Type: ArenaDocument4 paginiNormal Type: ArenaMuhammad Khairul AnwarÎncă nu există evaluări
- Branford High SchoolDocument1 paginăBranford High SchoolHelen BennettÎncă nu există evaluări
- S.A in Hope 2 WK 7-8 - With AnswerDocument2 paginiS.A in Hope 2 WK 7-8 - With AnswerChristine Manjares - OañaÎncă nu există evaluări
- Essay On Kargil DiwasDocument2 paginiEssay On Kargil DiwasLekshmipriya PÎncă nu există evaluări
- Lc025 Children Go Hungry During PandemicDocument2 paginiLc025 Children Go Hungry During Pandemicİbrahim TarzanÎncă nu există evaluări
- Hope4 Midterm ExamDocument6 paginiHope4 Midterm ExamEarl TrinidadÎncă nu există evaluări
- Unrivalled Comfort: For The Journey AheadDocument4 paginiUnrivalled Comfort: For The Journey AheadSria NingsihÎncă nu există evaluări
- Possessive Adjectives ExercisesDocument1 paginăPossessive Adjectives ExercisesJorge Pertuz100% (2)
- Bamboo EquipmentDocument21 paginiBamboo EquipmentRoel BrionesÎncă nu există evaluări
- The Tale of Peter RabbitDocument4 paginiThe Tale of Peter RabbitWellington LinsÎncă nu există evaluări
- Guilty Crown SonataDocument20 paginiGuilty Crown SonataAdam_G_Parker1738Încă nu există evaluări
- MC 00022 Seth Rosenbloom Intro To Blues V4Document39 paginiMC 00022 Seth Rosenbloom Intro To Blues V4fabio b.Încă nu există evaluări
- The Pterygopalatine FossaDocument6 paginiThe Pterygopalatine FossaxxyumeÎncă nu există evaluări
- Rock Drill & SluDocument59 paginiRock Drill & SluRıfat BingülÎncă nu există evaluări
- Atlas Copco Ga+Xa Technical Kit List 2009Document12 paginiAtlas Copco Ga+Xa Technical Kit List 2009vtichonov50% (4)
- Left 4 Dead ReviewDocument3 paginiLeft 4 Dead ReviewNaim ElmasriÎncă nu există evaluări
- Pei and 03 Ab Unit5Document6 paginiPei and 03 Ab Unit5Bene HispalisÎncă nu există evaluări
- Multi ElementDocument1 paginăMulti Elementapi-3703371Încă nu există evaluări
- Manual Massey FergusonDocument51 paginiManual Massey FergusonPatricio MontÎncă nu există evaluări
- Scene Elements WorksheetDocument1 paginăScene Elements WorksheetDanDan_XPÎncă nu există evaluări
- Tactics: Any LeveDocument5 paginiTactics: Any LeveVenu MadhavÎncă nu există evaluări