S-ar putea să vă placă și
- DOH Programs Related To Family Health (EDITED)Document93 paginiDOH Programs Related To Family Health (EDITED)Brix Valdriz100% (4)
- Department of Health Programs Related To Family HealthDocument62 paginiDepartment of Health Programs Related To Family HealthBea Bianca CruzÎncă nu există evaluări
- NCM 104 - Community Health Nursing 1Document10 paginiNCM 104 - Community Health Nursing 1ChelleyOllitro100% (3)
- Roles of Community Health NurseDocument12 paginiRoles of Community Health NurseEDz Delica SandovalÎncă nu există evaluări
- CHN BagDocument2 paginiCHN BagSpread Mushoo100% (13)
- Maternal Child NursingDocument31 paginiMaternal Child Nursingmatrixtrinity88% (24)
- #3 Family - Post Test 2Document2 pagini#3 Family - Post Test 2Sheena Valenzuela75% (4)
- Community Healtth Nursing I. Evolution of Public Health Nursing in The Philippines HealthDocument11 paginiCommunity Healtth Nursing I. Evolution of Public Health Nursing in The Philippines HealthHannahleth GorzonÎncă nu există evaluări
- Ethical Considerations in Community Health NursingDocument26 paginiEthical Considerations in Community Health NursingMarlon Glorioso II100% (2)
- Doh Health Programs MaternalDocument82 paginiDoh Health Programs MaternalWilma Nierva BeraldeÎncă nu există evaluări
- Exam FamilyDocument2 paginiExam FamilyJonaPhieDomingoMonteroIIÎncă nu există evaluări
- New Technologies Related To Public Health Electronic InformationDocument20 paginiNew Technologies Related To Public Health Electronic InformationMarlon Glorioso II100% (2)
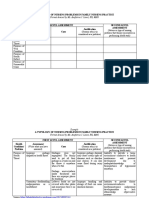
- Typology of Nursing Problems in Family Nursing PracticeDocument2 paginiTypology of Nursing Problems in Family Nursing PracticeHarlene Joyce Rey100% (3)
- The Doh Nutrition ProgramDocument10 paginiThe Doh Nutrition ProgramDianne MaeÎncă nu există evaluări
- CHN-RLE Module 2 (Home Visits)Document5 paginiCHN-RLE Module 2 (Home Visits)Ems Rio Bal100% (1)
- Doh Programs Related To Family HealthDocument24 paginiDoh Programs Related To Family Healthmirai desuÎncă nu există evaluări
- Community Health Nursing 1 NCM 104Document4 paginiCommunity Health Nursing 1 NCM 104Sheila May Teope Santos100% (1)
- EPI Vaccines HandoutsDocument14 paginiEPI Vaccines HandoutsBurhan uddin100% (11)
- Different Fields of NursingDocument29 paginiDifferent Fields of NursingRichmond Tan67% (9)
- Community Health NursingDocument237 paginiCommunity Health Nursingjhing_apdan100% (2)
- Community Health NursingDocument43 paginiCommunity Health Nursingstellie2593% (69)
- Course Syllabus Part A Course SpecificationsDocument12 paginiCourse Syllabus Part A Course SpecificationsAngel Joy Catalan100% (4)
- Doh Programs PDFDocument68 paginiDoh Programs PDFMikaela Lozano100% (1)
- Mandatory Infants and Children Health Immunization Act of 2011 Compulsory ImmunizationDocument3 paginiMandatory Infants and Children Health Immunization Act of 2011 Compulsory Immunizationbunso padilla100% (2)
- Nursing Care of A Family With A PreschoolerDocument32 paginiNursing Care of A Family With A PreschoolerBea Flor Rapisura-PegadÎncă nu există evaluări
- Unang YakapDocument3 paginiUnang YakapBernadeth Labrador100% (1)
- Records in Family Health Nursing PracticeDocument6 paginiRecords in Family Health Nursing PracticeA.j. Caraca89% (9)
- Community Assessment and DiagnosisDocument25 paginiCommunity Assessment and DiagnosisVince Patrick LeonidaÎncă nu există evaluări
- CHN-Week 1Document4 paginiCHN-Week 1rich_dela_china100% (3)
- NCM 107 1Document5 paginiNCM 107 1Clint Mikael EulatrizÎncă nu există evaluări
- REPORT Expanding Fields of Community and Public Health NursingDocument39 paginiREPORT Expanding Fields of Community and Public Health NursingPatrick Nava100% (2)
- Garantisadong PambataDocument3 paginiGarantisadong Pambataboss062212Încă nu există evaluări
- Essential Newborn Care: The DOH/WHO ProtocolDocument21 paginiEssential Newborn Care: The DOH/WHO ProtocolfelicitycherubÎncă nu există evaluări
- Care of Mother, Child and Adolescent (Well-Client) : Service CapabilityDocument4 paginiCare of Mother, Child and Adolescent (Well-Client) : Service CapabilityAJ Bay100% (3)
- Unang Yakap DOH EINCDocument20 paginiUnang Yakap DOH EINCDustin Diet100% (4)
- Final PPT - EincDocument75 paginiFinal PPT - EincJia Smith100% (3)
- Community Health Nursing in The PhilippinesDocument27 paginiCommunity Health Nursing in The PhilippinesKaloy Kamao100% (1)
- Unit 1 C H N: A O: What Is A Community ?Document43 paginiUnit 1 C H N: A O: What Is A Community ?Marcus, RN96% (49)
- Standards of Public Health Nursing in The PhilippinesDocument18 paginiStandards of Public Health Nursing in The PhilippinesWilma BeraldeÎncă nu există evaluări
- Module 7 - DOH ProgramDocument32 paginiModule 7 - DOH Programmirai desuÎncă nu există evaluări
- Care of Mother Child, Adolescent (Well Clients)Document2 paginiCare of Mother Child, Adolescent (Well Clients)Shheeeeeshh100% (1)
- Community Health Nursing I (NUPC 105) : Salvador P. Llavore, RM, RN, LPT, Man Dario M. Ragmac RNDocument44 paginiCommunity Health Nursing I (NUPC 105) : Salvador P. Llavore, RM, RN, LPT, Man Dario M. Ragmac RNRamiella Angelica Castro Ribon50% (2)
- Community Health Nursing 1: (Individual and Family As Clients)Document63 paginiCommunity Health Nursing 1: (Individual and Family As Clients)Wilma Nierva Beralde100% (4)
- Bag Technique and Urine TestingDocument25 paginiBag Technique and Urine TestingJairene Dave Martinez Cambalon100% (1)
- National Health SituationDocument118 paginiNational Health Situationmaria erika93% (56)
- CO and COPAR Notes For SendingDocument19 paginiCO and COPAR Notes For SendingMikko McDonie VeloriaÎncă nu există evaluări
- CHN Lecture 1Document20 paginiCHN Lecture 1knotstm100% (1)
- AO 2009 0025 Essential Newborn CareDocument15 paginiAO 2009 0025 Essential Newborn Carejulesubayubay542895% (21)
- Community Health Nursing Review (Edited)Document407 paginiCommunity Health Nursing Review (Edited)api-2658787991% (35)
- Mother FatherDocument10 paginiMother FatherAnonymousTargetÎncă nu există evaluări
- Women's Health and Safe Motherhood ProjectDocument28 paginiWomen's Health and Safe Motherhood Projectalfeel perezÎncă nu există evaluări
- Safe Motherhood ProgramDocument23 paginiSafe Motherhood ProgramAllessandria Daphne Sac Bagacina100% (2)
- CHN - m5Document12 paginiCHN - m5Kristine KimÎncă nu există evaluări
- Family PlanningDocument4 paginiFamily Planningfayetish100% (2)
- Maternal and Infant Mortality RateDocument7 paginiMaternal and Infant Mortality Rateeli pascualÎncă nu există evaluări
- Family Planning: Brief Description of ProgramDocument4 paginiFamily Planning: Brief Description of ProgramTomzki Cornelio100% (1)
- FAMILY PLANNINg ModuleDocument9 paginiFAMILY PLANNINg ModuleWynjoy NebresÎncă nu există evaluări
- Family PlanningDocument2 paginiFamily PlanningAnsary Aguam Alauya Jr.Încă nu există evaluări
- National Family Planning ProgramDocument14 paginiNational Family Planning ProgramMA. JYRELL BONITOÎncă nu există evaluări
- Doh Updated Prog S-ZDocument40 paginiDoh Updated Prog S-Zdeeday echavezÎncă nu există evaluări
- Mother FatherDocument10 paginiMother FatherAnonymousTargetÎncă nu există evaluări
- Cases BSN2-5Document17 paginiCases BSN2-5AnonymousTargetÎncă nu există evaluări
- NDT Post Mid Term AnswersDocument36 paginiNDT Post Mid Term AnswersAnonymousTargetÎncă nu există evaluări
- CHN ReviewerDocument9 paginiCHN ReviewerAnonymousTargetÎncă nu există evaluări
- Walang Kwentang NotesDocument107 paginiWalang Kwentang NotesAnonymousTargetÎncă nu există evaluări
- CHN LawsDocument1 paginăCHN LawsAnonymousTargetÎncă nu există evaluări
- NDT Reviewer PDFDocument9 paginiNDT Reviewer PDFAnonymousTargetÎncă nu există evaluări
- Nursing Care PlanDocument4 paginiNursing Care PlanAnonymousTargetÎncă nu există evaluări
- FluoroquinolonesDocument2 paginiFluoroquinolonesAnonymousTargetÎncă nu există evaluări
- PLM CN NRS 2107 CHN IDocument13 paginiPLM CN NRS 2107 CHN IAnonymousTargetÎncă nu există evaluări
- Health Assessment Lab Health History: Submitted byDocument7 paginiHealth Assessment Lab Health History: Submitted byAnonymousTargetÎncă nu există evaluări
- Nutrition and Diet Therapy: Section 1 Chapter 1: The Relationship of Food and Health Nutrients VitaminsDocument32 paginiNutrition and Diet Therapy: Section 1 Chapter 1: The Relationship of Food and Health Nutrients VitaminsAnonymousTargetÎncă nu există evaluări
- Refleksi Kasus: Trauma Buli Buli Pada Operasi ObstetrikDocument51 paginiRefleksi Kasus: Trauma Buli Buli Pada Operasi ObstetrikvinyÎncă nu există evaluări
- Fhsis IndicatorDocument117 paginiFhsis IndicatorTherese Mae MadroneroÎncă nu există evaluări
- Indicators of HealthDocument31 paginiIndicators of HealthShubham Vsk ArmaÎncă nu există evaluări
- A Development Disaster: HIV/AIDS As A Cause and Consequence of PovertyDocument28 paginiA Development Disaster: HIV/AIDS As A Cause and Consequence of Povertyago87100% (1)
- APPLICATION FORM FOR ETHICAL APPROVAL OF A RESEARCH PROJECT - FilledDocument15 paginiAPPLICATION FORM FOR ETHICAL APPROVAL OF A RESEARCH PROJECT - FilledamanabbÎncă nu există evaluări
- Medical Nursing IDocument12 paginiMedical Nursing If.abrahamÎncă nu există evaluări
- Lecture 4 Plumbing FixturesDocument57 paginiLecture 4 Plumbing FixturesSamille GarciaÎncă nu există evaluări
- Exercise in Environmental Risk AssessmentDocument5 paginiExercise in Environmental Risk AssessmentIsabelÎncă nu există evaluări
- Puerperal SepsisDocument30 paginiPuerperal Sepsisjonaa2564Încă nu există evaluări
- Exercises During PregnancyDocument6 paginiExercises During PregnancyestberryÎncă nu există evaluări
- Art Danial FajriansahDocument8 paginiArt Danial FajriansahCici FarochahÎncă nu există evaluări
- Mens Health ChecklistDocument4 paginiMens Health Checklistglobalmark100% (1)
- SanitationDocument40 paginiSanitationJaynes Ann BoaconÎncă nu există evaluări
- Nikko Lae D. Abdon Submitted To: Sir Errol Osumo: Caloocan Centralle Medical Diagnostic and PolyclinicDocument5 paginiNikko Lae D. Abdon Submitted To: Sir Errol Osumo: Caloocan Centralle Medical Diagnostic and PolyclinicbabykhoÎncă nu există evaluări
- ECO GUARD Brochure (W) PDFDocument4 paginiECO GUARD Brochure (W) PDFSANTHWANAM MED CAREÎncă nu există evaluări
- Pre Construction Risk Assessment (PCRA) 7 10 2015Document4 paginiPre Construction Risk Assessment (PCRA) 7 10 2015yeremia PratamaÎncă nu există evaluări
- DRUGS IN PREGNANCY - A Handbook For Pharmacist and Physician 2021 PDFDocument465 paginiDRUGS IN PREGNANCY - A Handbook For Pharmacist and Physician 2021 PDFadelia100% (1)
- WHO 2019 nCoV Vaccine - Introduction RA - Tool 2020.1 EngDocument33 paginiWHO 2019 nCoV Vaccine - Introduction RA - Tool 2020.1 EngfinnaÎncă nu există evaluări
- KMC Budget English 2019 2020 PDFDocument58 paginiKMC Budget English 2019 2020 PDFAbhishek SatpathyÎncă nu există evaluări
- Pengaruh Senam Nifas Terhadap Tinggi Fundus Uteri Dan Jenis Lochea Pada PrimiparaDocument10 paginiPengaruh Senam Nifas Terhadap Tinggi Fundus Uteri Dan Jenis Lochea Pada PrimiparaRhirin AkaseÎncă nu există evaluări
- BEmONC & CEmONCDocument39 paginiBEmONC & CEmONCYuuki Chitose (tai-kun)100% (3)
- Visual CommunicationDocument20 paginiVisual CommunicationShiela FranciscoÎncă nu există evaluări
- NEW - Microplanning Template For COVID-19 VaccinesDocument43 paginiNEW - Microplanning Template For COVID-19 Vaccinesfeil amor deladaÎncă nu există evaluări
- Medicinal Plants in Parturients of Afia-Yetu Health Center in Likasi (DRC) Prevalence and IndicationsDocument8 paginiMedicinal Plants in Parturients of Afia-Yetu Health Center in Likasi (DRC) Prevalence and IndicationsInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Surgical MenopauseDocument5 paginiSurgical MenopauseSusan HepziÎncă nu există evaluări
- 1 +Theresia+Jamini+1-9Document9 pagini1 +Theresia+Jamini+1-9Florentina yohana ngeluÎncă nu există evaluări
- Beneficiary Details: COVID-19Document1 paginăBeneficiary Details: COVID-19THAMIZHAZHAHAN SÎncă nu există evaluări
- AsepticDocument3 paginiAsepticJen BallesterosÎncă nu există evaluări
- OPN603 MidTerm 18166009 Kaicobad PDFDocument6 paginiOPN603 MidTerm 18166009 Kaicobad PDFKaicobad Hassan KochiÎncă nu există evaluări
- Public Health ConceptsDocument9 paginiPublic Health ConceptsSucheta MitraÎncă nu există evaluări