S-ar putea să vă placă și
- Strengthen Community ActionsDocument5 paginiStrengthen Community ActionstermskipopÎncă nu există evaluări
- PBH101 Assignment 01Document5 paginiPBH101 Assignment 01Siam AhmedÎncă nu există evaluări
- Hed 313 - Epidemiology-1Document7 paginiHed 313 - Epidemiology-1Tobi OladipupoÎncă nu există evaluări
- Clinical Epidemiology Assignment I: Submitted By: Ibalawanpynhun WriangDocument6 paginiClinical Epidemiology Assignment I: Submitted By: Ibalawanpynhun WriangElegant WriangÎncă nu există evaluări
- Introduction To Health EducationDocument19 paginiIntroduction To Health Educationnyambuj56Încă nu există evaluări
- SGD Lbm1 Modul PrioritasDocument33 paginiSGD Lbm1 Modul PrioritasNor KhasanahÎncă nu există evaluări
- Module 6.1 Prevention and Health ServicesDocument35 paginiModule 6.1 Prevention and Health ServicesSamuel MbiriÎncă nu există evaluări
- SHD Lecture Slides 2023 Themes 5 6Document44 paginiSHD Lecture Slides 2023 Themes 5 6pinehas nguluÎncă nu există evaluări
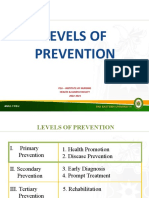
- Levels of Prevention and Modes of InterventionDocument22 paginiLevels of Prevention and Modes of Interventionachuth2980% (5)
- 2021-MPHFT-A01 ExamsDocument13 pagini2021-MPHFT-A01 ExamsƏfąþą RobertÎncă nu există evaluări
- Describe Five Examples of How Each Level of Disease Prevention Is Practiced in Your CountryDocument1 paginăDescribe Five Examples of How Each Level of Disease Prevention Is Practiced in Your Countryhasfa konsoÎncă nu există evaluări
- De Pedro, Lorinel - Pre Duty ResearchDocument3 paginiDe Pedro, Lorinel - Pre Duty Researchdepedro.lorinel10Încă nu există evaluări
- Preventing Illness and Living With Ill HealthDocument11 paginiPreventing Illness and Living With Ill HealthMonique MavronicolasÎncă nu există evaluări
- Prevention of Disease & Health PromotionDocument2 paginiPrevention of Disease & Health PromotionGhith WhiuÎncă nu există evaluări
- Levels of PreventionDocument5 paginiLevels of PreventionSofia JuliaÎncă nu există evaluări
- Extended and Expanded Roles of Nurses 1Document1 paginăExtended and Expanded Roles of Nurses 1Sivaprasad SÎncă nu există evaluări
- Levels of Disease PreventionDocument4 paginiLevels of Disease Preventionkagehaprecious31Încă nu există evaluări
- Concept of PreventionDocument48 paginiConcept of Preventionmahmoud100% (1)
- Community Medicine: Dr. Maryam M.Phil Physical-Therapy (SMC) BSPT (Uhs)Document28 paginiCommunity Medicine: Dr. Maryam M.Phil Physical-Therapy (SMC) BSPT (Uhs)Aleey ShahÎncă nu există evaluări
- Level of PreventionDocument54 paginiLevel of PreventionArun kumar100% (1)
- Rehabilitation Engg MaterialDocument107 paginiRehabilitation Engg MaterialTamil TskÎncă nu există evaluări
- Communit Y: HealthDocument29 paginiCommunit Y: HealthMa Cecelia PalmeroÎncă nu există evaluări
- Module 4 Levels of PreventionDocument29 paginiModule 4 Levels of PreventionZaren James D. RacaÎncă nu există evaluări
- Health Wellness and IllnessDocument42 paginiHealth Wellness and IllnessTwesigye DeusÎncă nu există evaluări
- Concept of Wellness and IllnessDocument6 paginiConcept of Wellness and IllnessGomathi SharmaÎncă nu există evaluări
- Health Promotion and Ilness PreventionDocument7 paginiHealth Promotion and Ilness Preventionzach felix100% (1)
- CHNDocument27 paginiCHNSamantha Marie100% (1)
- PHN PrinciplesDocument47 paginiPHN PrinciplesSarah MumbaÎncă nu există evaluări
- Final ResearchDocument38 paginiFinal ResearchAnjali ShahÎncă nu există evaluări
- Levels of Prevention PP. Lect. 9 NotesDocument23 paginiLevels of Prevention PP. Lect. 9 NotesAYO NELSONÎncă nu există evaluări
- Quarter Iii - Module Health Trends, Issues and Concern: (Global Level)Document48 paginiQuarter Iii - Module Health Trends, Issues and Concern: (Global Level)Francine ValenzuelaÎncă nu există evaluări
- Concepts in Health 2Document35 paginiConcepts in Health 2kuruvagadda sagarÎncă nu există evaluări
- Introduction To Community Health NursingDocument20 paginiIntroduction To Community Health NursingKrishnaveni MurugeshÎncă nu există evaluări
- Untitled DocumentDocument2 paginiUntitled DocumentKhenyuza Angel ClementeÎncă nu există evaluări
- Unit - 1 Introduction To Public HealthDocument63 paginiUnit - 1 Introduction To Public HealthVedansha SinghalÎncă nu există evaluări
- Levels Od Disease Prevention and ControlDocument38 paginiLevels Od Disease Prevention and ControlFeven AbrahamÎncă nu există evaluări
- Environment Annd Human: StructureDocument19 paginiEnvironment Annd Human: Structuretarakesh17Încă nu există evaluări
- Chapter 2: What Is Primary Health Care (PHC) and Why?Document3 paginiChapter 2: What Is Primary Health Care (PHC) and Why?alphabennydelta4468Încă nu există evaluări
- A Public Health Intervention Is An Organized Effort To Promote Those Specific Behaviors and Habits That Can Improve PhysicalDocument5 paginiA Public Health Intervention Is An Organized Effort To Promote Those Specific Behaviors and Habits That Can Improve PhysicalYonas MamoÎncă nu există evaluări
- Lab CPHDocument73 paginiLab CPHYam100% (1)
- MODULE 6 HealthDocument6 paginiMODULE 6 Healthtalithaonkabetse723Încă nu există evaluări
- Levels of PreventionDocument30 paginiLevels of Preventionethics wixÎncă nu există evaluări
- Foundations For Health Promotion Levels of Prevention: AbstractDocument4 paginiFoundations For Health Promotion Levels of Prevention: AbstractIme ApÎncă nu există evaluări
- Public Health Group AssignmentDocument7 paginiPublic Health Group AssignmentNANNYONGA OLGAÎncă nu există evaluări
- Long AnswerDocument5 paginiLong AnswerBruhathi sreeÎncă nu există evaluări
- Outbreak AssignmentDocument5 paginiOutbreak AssignmentEduard75% (8)
- Health Promotion '12Document32 paginiHealth Promotion '12Justine PlazaÎncă nu există evaluări
- MPH 5103 Lecture 1 - 02092022 - ZTMDocument38 paginiMPH 5103 Lecture 1 - 02092022 - ZTMRezwana SultanaÎncă nu există evaluări
- Introduction To CPH and History of Public Health IDocument6 paginiIntroduction To CPH and History of Public Health IReynajane TugadiÎncă nu există evaluări
- Health Education and Contagious Diseases Group 1Document32 paginiHealth Education and Contagious Diseases Group 1Jason CamaÎncă nu există evaluări
- Application of Epidemiology in Health Care DeliveryDocument15 paginiApplication of Epidemiology in Health Care DeliveryDebipriya Mistry100% (5)
- Kiran PresentationDocument4 paginiKiran PresentationZaim verseÎncă nu există evaluări
- Community MedicineDocument49 paginiCommunity MedicineRiyaz AhamedÎncă nu există evaluări
- Notes To Read 1Document4 paginiNotes To Read 1Rizzy UgayÎncă nu există evaluări
- Grade 8 Health Quarter 3Document3 paginiGrade 8 Health Quarter 3montenegrokrishamae36Încă nu există evaluări
- Essay GalanDocument1 paginăEssay GalanDaniel Angelo ArangoÎncă nu există evaluări
- Language of PreventionDocument9 paginiLanguage of Prevention1234chocoÎncă nu există evaluări
- An Introduction to Lifestyle Management:: Facilitator’s HandbookDe la EverandAn Introduction to Lifestyle Management:: Facilitator’s HandbookÎncă nu există evaluări
- Revision Notes On Section 1.6 - Belief, Uncertainty & UnbeliefDocument5 paginiRevision Notes On Section 1.6 - Belief, Uncertainty & Unbeliefnisalielisha rodrigoÎncă nu există evaluări
- The Passive Aggressive Disorder PDFDocument13 paginiThe Passive Aggressive Disorder PDFPhany Ezail UdudecÎncă nu există evaluări
- SANCHEZ V DEMETRIOUDocument3 paginiSANCHEZ V DEMETRIOUShenna SunicoÎncă nu există evaluări
- FrankensteinDocument51 paginiFrankensteinapi-272665425100% (1)
- 1 Patient Assessment Form.Document3 pagini1 Patient Assessment Form.Aina HaravataÎncă nu există evaluări
- Possessive Adjectives 3Document1 paginăPossessive Adjectives 3RAMIRO GARCIA CANCELAÎncă nu există evaluări
- Letters of ComplaintDocument3 paginiLetters of ComplaintMercedes Jimenez RomanÎncă nu există evaluări
- Keir 1-2Document3 paginiKeir 1-2Keir Joey Taleon CravajalÎncă nu există evaluări
- Fever and RashDocument14 paginiFever and RashwirdahajaÎncă nu există evaluări
- MNT-Notes Pt. 2Document58 paginiMNT-Notes Pt. 2leemon.mary.alipao8695Încă nu există evaluări
- Sancticity AllDocument21 paginiSancticity AllJames DeHart0% (1)
- Chapter 1 (Research)Document6 paginiChapter 1 (Research)Salome CarpioÎncă nu există evaluări
- Karaf-Usermanual-2 2 2Document147 paginiKaraf-Usermanual-2 2 2aaaeeeiiioooÎncă nu există evaluări
- ) Mark Scheme (Results) January 2019: Pearson Edexcel International GCSE in Mathematics A (4MA1) Higher Tier Paper 1HRDocument22 pagini) Mark Scheme (Results) January 2019: Pearson Edexcel International GCSE in Mathematics A (4MA1) Higher Tier Paper 1HRNewtonÎncă nu există evaluări
- 2011 Physics B Form B Scoring GuidelinesDocument16 pagini2011 Physics B Form B Scoring GuidelinesMichael CÎncă nu există evaluări
- Reflection IntouchablesDocument2 paginiReflection IntouchablesVictoria ElazarÎncă nu există evaluări
- Ansys Flu - BatDocument30 paginiAnsys Flu - BatNikola BoskovicÎncă nu există evaluări
- How To Access Proquest: Off-CampusDocument9 paginiHow To Access Proquest: Off-CampusZav D. NiroÎncă nu există evaluări
- My AnalysisDocument4 paginiMy AnalysisMaricris CastillanoÎncă nu există evaluări
- Diexis in Red by Taylor SwiftDocument11 paginiDiexis in Red by Taylor SwiftNirmana ArtstikaÎncă nu există evaluări
- 5 Reported Speech - T16-6 PracticeDocument3 pagini5 Reported Speech - T16-6 Practice39 - 11A11 Hoàng Ái TúÎncă nu există evaluări
- SjshagavDocument6 paginiSjshagavindah ayu lestariÎncă nu există evaluări
- Ulf Hannerz - Being There and ThereDocument17 paginiUlf Hannerz - Being There and ThereThomás MeiraÎncă nu există evaluări
- Chapter 6 Coming of SpainDocument4 paginiChapter 6 Coming of SpainJayvee MacapagalÎncă nu există evaluări
- Handout For Chapters 1-3 of Bouchaud: 1 DenitionsDocument10 paginiHandout For Chapters 1-3 of Bouchaud: 1 DenitionsStefano DucaÎncă nu există evaluări
- Qsen CurriculumDocument5 paginiQsen Curriculumapi-280981631Încă nu există evaluări
- Gesture and Speech Andre Leroi-GourhanDocument451 paginiGesture and Speech Andre Leroi-GourhanFerda Nur Demirci100% (2)
- mc96 97 01feb - PsDocument182 paginimc96 97 01feb - PsMohammed Rizwan AliÎncă nu există evaluări
- Book - IMO Model Course 7.04 - IMO - 2012Document228 paginiBook - IMO Model Course 7.04 - IMO - 2012Singgih Satrio Wibowo100% (4)
- Health Assessment Finals Review Flashcards - QuizletDocument92 paginiHealth Assessment Finals Review Flashcards - QuizletViea Pacaco SivaÎncă nu există evaluări