Documente Academic
Documente Profesional
Documente Cultură
06chapter PDF
Încărcat de
Prathibha PsTitlu original
Drepturi de autor
Formate disponibile
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentDrepturi de autor:
Formate disponibile
06chapter PDF
Încărcat de
Prathibha PsDrepturi de autor:
Formate disponibile
Chapter
06 Family Planning
Chapter - 06
6.1 INTRODUCTION up to Primary Health Centres (PHCs) and Sub
Centres(SCs) in rural areas as well as the Urban
India was the first country in the world to launch a Family Welfare Centres and Postpartum Centres in
National Programme for Family Planning in 1952. urban areas. There is also extensive engagement of the
Following its historic initiation, the Family Planning community health workers (ASHA) who distribute
program has undergone many transformations in contraceptives and pregnancy testing kits to desirous
terms of policy and actual program implementation. beneficiaries at their doorsteps.
Post International Conference on Population and
Development (ICPD) 1994 held in Cairo, there was Technological advances and enhanced quality of
a de-emphasis on Family Planning globally with the services have also resulted in a rapid fall in the Crude
donors substantially reducing the funding for Family Birth Rate (CBR), Total Fertility Rate (TFR) and
Planning (FP) programmes. However subsequently it growth rate. (2011 Census showed the steepest decline
was realized that without increasing use and access in the decadal growth rate)
to contraceptives, it would be difficult to impact the
high maternal, infant and child mortality. Thereafter
a gradual shift occurred from clinical approach to
the reproductive child health approach. The National
Population Policy (NPP) in 2000 brought about a
holistic and a target free approach which accelerated
the reduction of fertility.
Over the years, the program has expanded to reach
every nook and corner of the country and is available
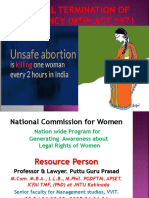
Trend of TFR and CBR
Population increase and growth rate
Annual Report | 2017-2018 85
Chapter - 06
The objectives, strategies and activities of the Family to honour the commitments of the Government of
Planning Division are designed towards achieving India (including ICPD: International Conference on
the family welfare goals and objectives stated in Population and Development, MDG: Millennium
various policy documents (NPP: National Population Development Goals, Sustainable Development Goals-
Policy 2000, NHP: National Health Policy 2002, and SDG, FP2020 Summit and others).
NRHM: National Rural Health Mission) as well as
I. Some facts on Family Planning and related matters
15.7 % expected increase of • From 1210 million in 2011 to 1400 million in 2026.
population in fifteen years Population Projection Report, 2006.
Decline in TFR • Helps to stabilize India’s population growth which in turn spurs the
economic and social progress
Greater investments in family • Helps to mitigate the impact of high population growth by helping
planning women achieve desired family size and avoid unintended and
mistimed pregnancies
• Reduce maternal mortality by 25-35%
• Reduce infant mortality and abortions significantly
Government of India’s • Maternal Mortality Ratio (MMR) to 100/100,000 live births
commitment
• Infant Mortality Rate (IMR) to 30/1000 live births
• Total Fertility Rate (TFR) to 2.1 by 2017 as per 12th Five Year Plan
II. Factors that influence Population Growth
Unmet need of Family Planning • 12.9% as per NFHS-4 (2015-16)
Age at Marriage and first childbirth • 26.8% of the girls get married below the age of 18 years as per
NFHS (2015-2016)
• Out of the total births, 10.7% are among teenagers i.e. 15-19 years
(SRS 2016)
Spacing between Births: • Spacing between two childbirths is less than the recommended
period of 3 years in 48.1% of births (SRS 2016)
15-24 age group • 36.5% contribution in total fertility (SRS 2016)
(women)
• 41% contribution in maternal mortality (SRS 2011-13)
III. Current Demographic Scenario in the Country (CENSUS 2011)
2.4% of world’s land mass • 17.5% of the world's population
1.21 billion • India’s population as per Census-2011
• Equal to the combined population of U.S.A., Indonesia, Brazil,
Pakistan, Bangladesh and Japan put together (1214.3 million).
200 million • Population of Uttar Pradesh - more than the population of Brazil
86 Annual Report | 2017-2018
Chapter - 06
Ratio of Growth of Population in India: IV. Progress in TFR:
TFR Data
Census Population Decadal Average Source
Year (In Crores) Growth (%) Annual
Exponential TFR decline • From 2.9 in 2005 to 2.3 in
Growth (%) 2016
1971 54.82 24.80 2.20 • Decline more significant in
High Focus States.
1981 68.33 24.66 2.22 TFR of 2.1 or • 24 States and Union
less Territories – Sikkim-1.2,
1991 84.64 23.87 2.16
Andaman and Nicobar-1.5,
2001 102.87 21.54 1.97 Chandigarh-1.6, Delhi-1.6,
Tamil Nadu-1.6, West
2011 121.02 17.64 1.64 Bengal-1.6, Andhra
Pradesh-1.7, Daman and
Diu-1.7, Goa-1.7, Himachal SRS
Perceptible decline • Maternal Mortality ratio – 556 Pradesh-1.7, Jammu and 2016
(in last 5 in 1990 to 167 in 2011-13 Kashmir-1.7, Puducherry-1.7, and
decades) Punjab-1.7, Telangana-1.7, NFHS
Tripura-1.7, Karnataka-1.8, IV
• Crude birth rate – 40.8 per 1000 Kerala-1.8, Lakshadweep-1.8,
in 1951 to 20.4 in 2016. Maharashtra-1.8,
Uttrakhand-1.9, Odisha-2.0,
• Infant mortality rate – from 146
Gujarat-2.0, Haryana-2.1,
in 1951-61 to 34 in 2016.
Arunachal Pradesh 2.1
• Total Fertility rate – from 6.0 in TFR 2.2-3.0 • 9 States and Union Territories
1951 to 2.3 in 2016 – Assam-2.3, Dadra & Nagar
• Steepest decline in growth rate Haveli-2.3, Mizoram-2.3,
between 2001 and 2011 from Chhattisgarh-2.5,
21.54% to 17.64%. Jharkhand-2.6, Manipur-2.6,
Rajasthan-2.7, Nagaland-2.7,
• Decline in 0-6 population by Madhya Pradesh-2.8
3.08% compared to 2001
TFR more than • 3 States - Bihar-3.3,
Population added • Lesser than the previous decade, or equal to 3.0 Uttar Pradesh-3.1 and
18.14 crores added during 2001- Meghalaya-3.0
2011 compared to 18.23 crores
during 1991-2011. Impact of High Focus Approach of the Government
of India
Significant decline • There is a 4.1 percentage point
fall from 24.99% in 2001 to Government of India has categorized States as per the
20.92% in 2011 in the growth TFR level into very high-focus (more than or equal to
rate of population in the EAG 3.0), high-focus (more than 2.1 and less than 3.0) and
States non-high focus (less than or equal to 2.1) categories.
(U.P, Bihar, Jharkhand, M.P, There are three States in the very high focus category
Chhattisgarh, Rajasthan, Orissa - Bihar, Uttar Pradesh and Meghalaya. As per recent
and Uttaranchal) after decades SRS figures, Bihar has shown an increase by 0.1 point
of stagnation. from 2015 to 2016 while, the TFR in Uttar Pradesh
• The Birth rate has declined from has remained constant. Meghalaya on the other hand
23.8 in 2005 to the current 20.4 (not covered under SRS) shows a 0.8 point decline
in 2016. from NFHS III (2005-06) to NFHS IV (2015-16).
Annual Report | 2017-2018 87
Chapter - 06
Category State SRS 2015 SRS 2016
Very High Focus States for FP Bihar 3.2 3.3
Uttar Pradesh 3.1 3.1
High Focus States for FP Meghalaya 3.8* 3.0#
Madhya Pradesh 2.8 2.8
Nagaland 3.7* 2.7#
Rajasthan 2.7 2.7
Manipur 2.8* 2.6#
Jharkhand 2.7 2.6
Chhattisgarh 2.5 2.5
Mizoram 2.9* 2.3#
Dadar & Nagar Haveli - 2.3#
Assam 2.3 2.3
Source: *NFHS III and #NFHS IV
6.2 CURRENT FAMILY PLANNING A. Injectable Contraceptive MPA under the
EFFORTS ‘Antara’ programme – which has been recently
introduced in the current basket of choices.
Family planning has undergone a paradigm shift and
emerged as a key intervention to reduce maternal and B. Oral contraceptive pills (OCP)
infant mortalities and morbidities. It is well-established
that the States with high contraceptive prevalence rate • These are hormonal pills which have to be
have lower maternal and infant mortalities. taken daily by a woman, preferably at a fixed
time. The strip also contains additional iron
Greater investments in family planning can thus pills to be consumed during the hormonal pill
help mitigate the impact of high population growth free days. The method may be used by majority
by helping women achieve desired family size and of women after screening by a trained provider.
avoid unintended and mistimed pregnancies. Further,
contraceptive use can prevent recourse to induce • At present, there is a scheme for delivery of
abortion and eliminate most of these deaths. OCPs at the doorstep of beneficiaries by ASHA
with a minimal charge. The brand “MALA-N”
6.2.1 Contraceptive services under the National is available free of cost at all public healthcare
Family Welfare Program facilities.
The methods available currently in India can be • Centchroman “Chhaya”- The once a week
broadly divided into two categories, spacing methods non-steroidal oral pill has also been recently
and permanent methods. An additional method introduced in the current basket of choices.
available is the emergency contraceptive pill which is
to be used in cases of emergency. C. Condoms
6.2.2 Spacing Methods- these are the reversible • These are barrier methods of contraception
methods of contraception to be used by couples who which offer the dual protection of preventing
wish to have children in future. These include: unwanted pregnancies as well as transmission
of RTI/STI including HIV. The brand “Nirodh”
88 Annual Report | 2017-2018
Chapter - 06
is available free of cost at government health inserting a long thin tube with a lens in it into
facilities and supplied at doorstep by ASHAs at the abdomen through a small incision. This
minimal cost. laparoscope enables the doctor to see and block
or cut the fallopian tubes in the abdomen. Can
D. Intra-Uterine Contraceptive Devices (IUCD) be done only by trained and certified MBBS
• Copper containing IUCDs are a highly effective doctor or specialist.
method for long term birth spacing. o Post Abortion Sterilisation - This refers to the
• Should not be used by women with uterine sterilization done within 7 days of a complete
anomalies or women with active PID or those abortion.
who are at increased risk of STI/RTI (women B. Male Sterilisation
with multiple partners).
• Through a puncture or small incision in the
• The acceptor needs to return for follow up visit scrotum, the provider locates each of the 2 tubes
after 1, 3 and 6 months of IUCD insertion as the that carries sperm to the penis (vas deferens) and
expulsion rate is highest in this duration. cuts or blocks it by cutting and tying it closed
• Two types: or by applying heat or electricity (cautery).
The procedure is performed by MBBS doctors
o Cu IUCD 380A (10 yrs) trained in these. However, the couple needs
to use an alternative method of contraception
o Cu IUCD 375 (5 yrs)
for first three months after sterilization till no
• New approach of method delivery- postpartum sperms are detected in semen.
IUCD (PPIUCD) insertion by specially trained
• Two techniques being used in India:
providers to tap the opportunities offered by
institutional deliveries. ¾¾ Conventional
• Post Abortion IUCD (PAIUCD) – Repeated ¾¾ on- scalpel vasectomy – no incision,
N
unintended pregnancies and unwanted births or only puncture and hence no stiches.
abortions contributes to increase morbidity and
mortality among mothers and newborns. The 6.2.4 Emergency Contraceptive Pill
provision of effective post abortion services • To be consumed in cases of emergency arising
helps in decreasing maternal morbidities by out of unplanned/unprotected intercourse.
averting unwanted pregnancies.
• The pill should be consumed within 72 hours of
6.2.3 Permanent Methods- these methods may the sexual act and should never be considered a
be adopted by any member of the couple and are replacement for a regular contraceptive.
generally considered irreversible.
6.2.5 Other Commodities - Pregnancy testing kits
A. Female Sterilisation
• Helps to detect pregnancy as early as one
• There are two techniques: week after the missed period, thus proving
o Minilap - Minilaparotomy involves making a an early opportunity for medical termination
small incision in the abdomen. The fallopian of pregnancy, thus saving lives lost to unsafe
tubes are brought to the incision to be cut abortions.
or blocked. Can be performed by a trained • These are available at the sub Centre level and
MBBS doctor. also carried by ASHA.
o Laparoscopic - Laparoscopy involves
Annual Report | 2017-2018 89
Chapter - 06
6.2.6 Service Delivery Points • Permanent methods are generally available at
Primary Health Centre level or above. They
• All the spacing methods, viz. IUCDs, OCPs
are provided by MBBS doctors who have been
and condoms are available at the public health
trained to provide these services. Laparoscopic
facilities beginning from the Sub-Centre level.
sterilization is being offered at CHCs and above
Additionally, OCPs condoms, and emergency
level by a specialist gynecologist/surgeon only.
contraceptive pills (since are not skill based
services) are available at the village level also • These services are provided to around 20 crores
through trained ASHAs. eligible couples. Details of services provided at
different levels of facilities are as follows:
Family Planning Method Service Provider Service Location
LIMITING METHODS
Minilap Trained & certified MBBS doctors & PHC & higher levels
Specialist Doctors
Laparoscopic Sterilization Trained & certified MBBS doctors & Usually CHC & higher levels
Specialist Doctors
NSV(No Scalpel Vasectomy) Trained & certified MBBS doctors & PHC & higher levels
Specialist Doctors
SPACING METHODS
Interval IUCD Trained & certified ANMs, LHVs, Sub Centre & higher levels
SNs and doctors
Post-Partum IUCD Trained & certified nurses and Currently PHC and higher
doctors levels (Delivery Points)
Oral Contraceptive Pills (OCPs) Trained ASHAs, ANMs, LHVs, SNs Village level
and doctors Sub Centre & higher levels
Condoms Trained ASHAs, ANMs, LHVs, SNs Village level
and doctors Sub Centre & higher levels
Injectable Contraceptive MPA Trained doctors, SNs, LHVs an d Medical Colleges and District
ANMs Hospital (In MPV districts at
all levels up to Sub-Centre)
EMERGENCY CONTRACEPTION
Emergency Contraceptive Pills Trained ASHAs, ANMs, LHVs, SNs Village level
(ECPs) and doctors Sub Centre & higher levels
Note: Contraceptives like OCPs, Condoms are also provided through Social Marketing Organizations.
90 Annual Report | 2017-2018
Chapter - 06
6.3 SALIENT FEATURES OF THE FAMILY years’ effectivity), Cu IUCD 375 under the
PLANNING PROGRAMME National Family Planning Programme.
A. On-going interventions • A new method of IUCD insertion (post-partum
IUCD insertion) has been introduced by the
• More emphasis on Spacing methods like Government. The current emphasis is on
PPIUCD and IUCD. provision of PPIUCD services.
• Availability of Fixed Day Static Services at all • Promoting Post-partum Family Planning
facilities. services at district hospitals by providing
for placement of dedicated Family Planning
• Emphasis on Minilap tubectomy services Counsellors and training of personnel.
because of its logistical simplicity and
associated with less failure and complication • Home Delivery of Contraceptives (HDC):
rates. ¾¾ The scheme was launched to utilize
• A rational human resource development plan the services of ASHA to deliver
is in place for provision of IUCD, Minilap contraceptives at the doorstep of
and NSV to empower the facilities (DH, CHC, beneficiaries. The scheme is operational
PHC, SHC) with at least one provider each in the entire country.
for each of the services and Sub Centres with ¾¾ ASHA is charging a nominal amount
ANMs trained in IUD insertion. from beneficiaries for her effort to deliver
contraceptives at doorstep i.e. Re 1 for a
• Ensuring quality care in Family Planning
pack of 3 condoms, Re 1 for a cycle of
services by establishing Quality Assurance
OCPs and Rs 2 for a pack of one tablet
Committees at State and district levels.
of ECP.
• Accreditation of more private/ NGO facilities to
• Ensuring Spacing at Birth (ESB):
increase the provider base for family planning
services under PPP. ¾¾ Under this scheme, the services of
ASHAs are utilized for counselling
• Increasing male participation and promoting
newly married couples to ensure spacing
Non- scalpel Vasectomy.
of 2 years after marriage and couples
• Compensation scheme for sterilization with 1 child to have spacing of 3 years
acceptors - under the scheme MoHFW after the birth of 1st child. The scheme
provides compensation for loss of wages to is operational in 18 States (EAG, North
the beneficiary and also to the service provider Eastern and Gujarat and Haryana).
(& team) for conducting sterilizations. The ASHA are paid the following incentives
compensation scheme has been enhanced in 11 under the scheme:
high focus States from the year 2014. ¾¾ Rs. 500/- to ASHA for delaying first child
• ‘National Family Planning Indemnity Scheme’ birth by 2 years after marriage.
under which clients are indemnified in the ¾¾ Rs. 500/- to ASHA for ensuring spacing
eventualities of deaths, complications and of 3 years after the birth of 1st child
failures following sterilization. The providers/
¾¾ Rs. 1000/- in case the couple opts for
accredited institutions are indemnified against
a permanent limiting method up to 2
litigations in those eventualities.
children only
• PPIUCD Incentive for service providers and
ASHAs. • The spacing component of the scheme has been
extended in a few other States where spacing
• MoHFW has introduced short term IUCD (5 is low - Karnataka, West Bengal, Maharashtra,
Annual Report | 2017-2018 91
Chapter - 06
Andhra Pradesh, Punjab, Telangana and Daman under the Mission Parivar Vikas which
& Diu. Dadra & Nagar Haveli also initiated comprises of:
the implementation of the ESB scheme (both
a. Delivering assured services
spacing and limiting components).
b. Building additional capacity/Human
• Pregnancy Testing Kits: resource development for enhanced
service delivery
¾¾ Nishchay - Home based Pregnancy Test
Kits (PTKs) was launched under NRHM c. Ensuring commodity security
in 2008 across the country and anchored
d. Implementing new ‘promotional
with the Family Planning Division on
schemes’
24th January, 2012.
e. Creating an enabling environment
¾¾ The PTKs have been made available at
Sub Centers and to the ASHAs. • Expansion of Basket of Choice - The current
basket of FP choices has been expanded to
¾¾ The PTKs facilitate the early detection include new contraceptives namely Injectable
and decision making for the outcomes of MPA under Antara Programme, POP and
pregnancy. Centchroman (Chhaya).
• Improving contraceptives supply management
up to peripheral facilities.
• Demand generation activities in the form of
display of posters, billboards and other audio
and video materials in the various facilities.
• To improve quality of services rendered, State
and divisional level Family Planning reviews
along with monitoring and comprehensive
supportive supervision visits were undertaken.
• Strong political will and advocacy at the highest
level, especially in States with high fertility
rates.
• Family Planning Logistics Information
6.4 NEW INTERVENTIONS TO IMPROVE
System (FP-LMIS): The FP-LMIS has
ACCESS TO CONTRACEPTION
been launched to manage the distribution of
• Mission Parivar Vikas - The Government contraceptives and strengthen the supply-chain
has conceived Mission Parivar Vikas management system. It will serve as a decision-
for substantially increasing the access to making tool for policy makers, programme
contraceptives and family planning services in managers and logistics personnel to monitor
the high fertility districts of seven high focus and manage the flow of contraceptive supplies,
States with TFR of 3 and above. These 146 in order to reduce stock-outs and overstocks,
districts are from the seven high focus, High and improve the programme’s effectiveness
TFR States (Uttar Pradesh, Bihar, Rajasthan, and contraceptive security. The national
Madhya Pradesh, Chhattisgarh, Jharkhand and trainings for the key stakeholders have been
Assam) which constitutes 44% of the country’s completed and the State and district trainings
population. are underway. The ground stock entry for State
warehouses and Government Medical Store
A five pronged strategy has been developed Depots has been completed.
92 Annual Report | 2017-2018
Chapter - 06
• Clinical Outreach Team (COT) Scheme: One Sterilisation’, for Clinical Outreach Teams
of the main reasons for high fertility in the MPV (COT) operated by accredited organizations in
districts is the scarcity of providers in public the 146 MPV districts.
health facilities and a dearth of private sector
facilities for provision of Family Planning • Media Campaign Phase 2: The second
services. In order to address this issue, the States phase of the 360 degree media campaign was
have been engaging Clinical Outreach Teams launched by the Hon’ble HFM, Shri J. P. Nadda
(COT) comprising a mobile team of trained at the celebration of the World Population Day
health care personnel and equipment, engaged 2017 in July 2017. A multimedia campaign was
through private accredited organizations/ designed with the objective of reaching out to
NGOs, providing sterilization services in far- people of all age groups, regions and strata of
flung and underserved areas. In order to sustain the society to bring about a positive change in
the provision of the quality Family Planning the use of contraception and shatter the myths
services through the mechanism of COT, around it. The media campaign was set out in 3
the Government has carved out an extension different mediums.
from the existing ‘Compensation Scheme in
State Fact Sheets released by Hon. Health Minister Shri J.P. Nadda on World Population Day held on 11th July, 2017 at
New Delhi in the presence of Hon. MoS Smt. Anupriya Patel AS&DG Dr. R.K. Vats JS Smt. Gurnani and EA Smt. P. Nath
• Multi media campaign The TVC’s were based on the following themes:
¾¾ Television Spots/TVC: Four television o Mardangi and Involvement of
spots on various themes were finalized Men: Responsibility of men in family
and developed. The same is being planning is the true sign of masculinity
telecast on National Television and the and the importance of promoting male
audio versions of the spots are also being engagement in family planning.
broadcasted on All India Radio and its
primary channels.
Annual Report | 2017-2018 93
Chapter - 06
o Daadi: Dispelling old notions and aims to mitigate the social pressures faced by newlyweds from elders
and family members on bearing children immediately after marriage
94 Annual Report | 2017-2018
Chapter - 06
o Sangeet/Asha didi: Introduction of new contraceptive injection MPA as an effective method of
contraception for the newlyweds
o Involvement of Men: Promoting Involvement of man in family planning and preparing men to be ideal
grooms & husbands
¾¾ Posters and Hoardings: A series of posters and hoardings were launched. The messages portrayed in these
posters focused on the new contraceptive, involvement of men and family in family planning, spacing
between children and delay in first child.
¾¾ WhatsApp messages: Video messages recorded by celebrities - Mr. Ravi Kishen and Ms. Mahi Gill -
promoting new contraceptives and role of men in family planning were developed. These messages will
be disseminated through the medium of WhatsApp.
¾¾ Radio Chat Show: “HUM DO” – a 52 week long show hosted by a couple RJ, air every Sunday, from 10
am to 10.30 am, on FM Rainbow and its primary channels. Each episode covers a topic relevant to Family
Annual Report | 2017-2018 95
Chapter - 06
Planning in the context of a newly married information on family planning. It showcases all
couple who discuss their journey and experiences the current programmatic updates in a simple,
while embarking upon the use of contraceptives consumer friendly manner. In a short period of
methods. It is an interactive show where listeners 3 months, it has already garnered approximately
can call-in or message their queries. Additionally, 29,000 hits proving its popularity.
the 1st Sunday of every month is dedicated to a
National Expert appearing on the show who ¾¾ Dedicated Call Centre: A toll free helpline
further enlightens the listeners on the wide array number 1800 116 555 has been set up for young
of FP choices as well as respond to individual and married couples to call and find out about
queries of callers. information on family planning and address
queries. There has been a substantial increase
¾¾ Website: A dedicated website for Family in the number of callers from 200 to around
Planning Division has been developed www. 1500 per day seeking information about various
humdo.nhp.gov.in. The website is one stop aspects of family planning.
solution for anybody wanting to access accurate
96 Annual Report | 2017-2018
Chapter - 06
• The Social Franchising Scheme for involving as a key spacing method under Family Planning
the private sector in providing quality FP Programme.
services will be implemented in the States of
Uttar Pradesh and Bihar. “Alternative Training Methodology in IUCD” using
anatomical, simulator pelvic models incorporating
6.5 PROGRESS MADE UNDER FAMILY adult learning principles and humanistic training
PLANNING PROGRAMME technique was started in September, 2007 to train
service providers in provision of quality IUCD
Service Delivery services. A comprehensive review of IUCD training
The performance of family planning services (in manual has also been undertaken to strengthen the
lakhs) over the last three years till date is provided IUCD service delivery.
below. 6.5.2 Increasing provider base for IUCD
(Multitasking: Through AYUSH
Practitioners)
o In a policy change, the government allowed
26.1
IUCD 59.71
55.4 AYUSH doctors (except Yoga and Naturopathy
practitioners) to perform IUCD insertions at
19.6 public health facilities after a short refresher
Sterilisation 39.3 course/training.
40.69
6.5.3 Onsite training for IUCD services
0 10 20 30 40 50 60 70
2017-18 (Upto December) 2016-17 2015-16 • Jhpiego, Engender Health and IPAS have been
engaged for onsite training for IUCD services
in all the high focus States as well as those
• Against the backdrop of a continuously falling
States where spacing is an issue.
birth rate and total fertility rate, the performance
in IUCD and sterilisation has been maintained. • To track the progress of training and for better
post training follow up an IUCD tracking
• Considering the current efforts to focus on
software has been designed and is operational
spacing, it is expected that IUCD performance,
now.
especially PPIUCD, would increase in near
future. 6.5.4 Emphasis on Postpartum Family Planning
(PPFP) services
• State wise sterilization and IUCD achievements
is provided at Annexure-1. • In order to capitalize on the opportunity
provided by increased institutional deliveries,
6.5.1 Promotion of IUCDs as a short & long
the Government of India is focusing on
term spacing method
strengthening post-partum FP services.
In 2006, Government of India launched “Repositioning
• PPFP services are not being offered uniformly
IUCD in National Family Welfare Program” with an
at all levels of health system across different
objective to improve the method mix in contraceptive
States of India resulting in missed opportunities.
services and has adopted diverse strategies including
advocacy of IUCD at various levels; community • Insertion of IUCD during the post partum
mobilization for IUCD; capacity building of public period, known as Postpartum Intrauterine
health system staff starting from ANMs to provide Contraceptive Device (PPIUCD), is being
quality IUCD services and intensive IEC activities focused upon to address the high unmet need of
to dispel myths about IUCD. Currently, increased spacing during postpartum period.
emphasis is given to promotion of IUCD insertion
Annual Report | 2017-2018 97
Chapter - 06
6.5.5 Actions taken and achievements ¾¾ Other family planning methods such as
• Strengthening Post-Partum IUCD (PPIUCD) condoms, pills etc.
services at high case load facilities: ¾¾ Ensuring healthy timing and spacing of
pregnancy
o Currently the focus is on placement of
trained providers for PPIUCD insertion ¾¾ Mother & baby care
at district and sub-district hospital level ¾¾ Early initiation of breast feeding
only, considering the high institutional
delivery load at these facilities. ¾¾ Immunization
¾¾ Child nutrition
800000
700000
6.5.6 Assured delivery of family planning
600000
services:
500000
400000
Fixed Day Services (FDS) for IUCD Insertion: States
300000
are facilitated to ensure fixed days IUCD insertion
200000 services at the level of SC and PHC (at least 2 days
in a week).
670505
575180
528003
452238
369635
356639
289660
172723
164988
156293
132170
112613
100000
0
Fixed Day Static Services in Sterilisation at facility
level:
• Operationalization of FDS has following
Top performing states as per total PPIUCD insertions objectives:
(in lakhs)
− To make a conscious shift from camp
• Total 44,07,982 PPIUCDs have been inserted approach to regular routine services.
all across the country since the initiation of the − To make health facilities self sufficient in
PPIUCD programme. provision of sterilization services.
o The performance has been steadily − To enable clients to avail sterilization
increasing with 6, 64,359 PPIUCD services on any given day at their
insertions in 2014-15 followed by designated health facility.
10,65,433 insertions in 2015-16 (increase
by 60% from 2014-15) and 16,90,155 FDS Guidelines for sterilization services
insertions in 2016-17 (increase by 59% Health Facility Minimum frequency
from 2015-16).
District Hospital Twice a week
o In 2017-18, up till December, there have
been 13,48,052 PPIUCD insertions Sub District Hospital Weekly
CHC / Block PHC Fortnightly
• Appointing dedicated counsellors at high
case load facilities: 24×7 PHC / PHC Monthly
o RMNCH+A counsellors are being Note: Those facilities providing more frequent services
appointed at all high case load facilities already must continue to do so.
to provide counselling services in
following areas: 6.5.7 Phasing out Camps – As per the Hon’ble
Supreme Court guidelines, traditional camp approach
¾¾ Post-partum Family Planning (IUCD and for sterilization services will be phased out over the
Sterilisation) next 3 years.
98 Annual Report | 2017-2018
Chapter - 06
Rational placement of trained providers at the • Ensuring translation of the updated consent
peripheral facilities for provision of regular family forms and post-operative instruction cards in
planning services. the local language and clients are explained
about the procedure so that an informed consent
6.5.8 Quality assurance in family planning is obtained from them as per Government of
India guidelines.
Quality assurance in family planning services is the
decisive factor in acceptance and continuation of • Preparation of the biannual report and QACs are
contraceptive methods and services. The Hon’ble also to prepare an annual report card, depicting
Supreme Court of India in its Order dated 1.3.2005 statistical as well as non-statistical information
in Civil Writ Petition No. 209/2003 (Ramakant Rai like meetings held, enquiries conducted,
V/s Union of India) has, inter alia, directed the Union remedial steps taken and achievement for the
of India and States/UTs for ensuring enforcement year and upload the same on State/UT website
of Union Government’s Guidelines for conducting to be linked to the website of MOHFW,
sterilization procedures and norms for bringing out Government of India.
uniformity with regard to sterilization procedures by: • Phasing out sterilization camps over a period of
three years and provide services on fixed day
• Creation of panel of Doctors/health facilities for mode by strengthening Primary Health Care
conducting sterilization procedures and laying Centres appropriately.
down of criteria for empanelment of doctors for
conducting sterilization procedures. 6.5.9 Other promotional schemes
Compensation scheme for acceptors of sterilization
• Laying down of checklist to be followed by
every doctor before carrying out sterilization • Government has been implementing a Centrally
procedure. Sponsored Scheme since 1981 to compensate
the acceptors of sterilization for the loss of
• Laying down of uniform proforma for obtaining wages for the day on which he/she attended the
of consent of person undergoing sterilization. medical facility for undergoing sterilization.
• Setting up of Quality Assurance Committee for This compensation scheme for acceptors of
ensuring enforcement of pre and postoperative sterilization services was revised with effect
guidelines regarding sterilization procedures. from 31.10.2006 and has been further improved
with effect from 07.09.2007.
• Bringing into effect an insurance policy
uniformly in all States for acceptors of • In the light of the rise in cost of living, the
sterilizations etc. ever increasing transport cost which enables
a client to travel from his residence/village to
The Hon’ble Supreme Court has recently given the nearest service centre, the prevalent high
specific directions in its order dated 14.9.2016, to be wage compensation for the days requiring
strictly followed by the Government of India, the State recuperation as well as other incidental cost
Governments and Union Territories for delivering the Government in 2014 had further approved
quality family planning services in the country. The an enhancement in the current compensation
key strategic actions to be undertaken under each of package for the 11 high focus States- Uttar
the above directives along with the timeline have been Pradesh, Bihar, Madhya Pradesh, Rajasthan,
shared with all states and are as follows: Chhattisgarh, Jharkhand, Odisha, Uttarakhand,
• Uploading the list of empanelled sterilization Assam, Haryana and Gujarat.
providers and Quality Assurance Committee
• The Government also launched the Mission
members with their names and full particulars
Parivar Vikas for 146 high fertility districts
in the State/UT website is to be linked to the
where an attractive package was introduced.
website of MoHFW, Government of India.
Annual Report | 2017-2018 99
Chapter - 06
Compensation scheme in Public Facilities
States Type of Operation Acceptor ASHA/ Health Others Total
Worker
11 High focus States (UP, BH, VASECTOMY 2000 300 400 2700
MP, RJ, CG, JH, OD, UK, AS,
HR, GJ) TUBECTOMY 1400 200 400 2000
VASECTOMY 3000 400 600 4000
TUBECTOMY 2000 300 500 2800
TUBECTOMY (PPS) 3000 400 600 4000
Mission Parivar Vikas Districts
VASECTOMY 3000 400 1600 5000
(COT)
TUBECTOMY 2000 300 2200 4500
(COT)
Other High focus States (NE VASECTOMY 1100 200 200 1500
States, J&K, HP) TUBECTOMY 600 150 250 1000
VASECTOMY 1100 200 200 1500
TUBECTOMY 600 150 250 1000
Non High focus States
(BPL + SC/ ST only)
TUBECTOMY(APL) 250 150 250 650
Compensation scheme in Private Accredited Facilities
States Type of Operation Facility Others/ Total
Acceptor
11 High focus States (UP, BH, MP, RJ, VASECTOMY (ALL) 2000 1000 3000
CG, JH, OD, UK, AS, HR, GJ)
TUBECTOMY (ALL) 2000 1000 3000
Mission Parivar Vikas Districts VASECTOMY (All) 2500 1000 3500
TUBECTOMY (All) 2500 1000 3500
POST PARTUM 3000 1000 4000
STERILIZATION (PPS)
Other High focus States (NE States, VASECTOMY (ALL) 1300 200 1500
J&K, HP)
TUBECTOMY (ALL) 1350 150 1500
Non High focus States VASECTOMY (ALL) 1300 200 1500
TUBECTOMY (ALL) 1350 150 1500
100 Annual Report | 2017-2018
Chapter - 06
6.6 NATIONAL FAMILY PLANNING except Tamil Nadu, Puducherry and Himachal
INDEMNITY SCHEME (NFPIS) Pradesh where ASHA structure is non-existent.
Contraceptive distribution in these three States
With effect from, 01.04.2013, it has been decided is being done by Anganwadi Workers and
that States/UTs would process and make payment ANMs.
of claims to acceptors of sterilization in the event
of death/failures/complications /Indemnity cover to 6.6.2 Scheme for Ensuring Spacing at births
doctors/health facilities. The States/UTs would make
suitable budget provisions for implementation of the • Under the scheme, services of ASHAs to be
scheme through their respective State/UT Program utilised for counselling newly married couples
Implementation Plans (PIPs) under the National Rural to ensure spacing of 2 years after marriage and
Health Mission (NRHM) and the scheme is renamed couples with 1 child to have spacing of 3 years
as “Family Planning Indemnity Scheme”. after the birth of 1st child.
• The scheme was initially conceived for 18 States
Claims arising out of Sterilization Amount
– 8 EAG, 8 North East, Gujarat and Haryana
Operation (Rs.)
but in later years the spacing component of the
A Death at hospital/ within seven 2,00,000 scheme was rolled out in few other States like
days of discharge Karnataka, West Bengal, Maharashtra, Andhra
B Death following Sterilization 50,000 Pradesh, Punjab, Telangana and Daman & Diu.
(8th – 30th day from discharge) Dadra and Nagar Haveli have also initiated the
implementation of the scheme (both spacing
C Expenses for treatment of 25,000 and limiting components).
Medical Complications
6.6.3 Celebration of World Population Day &
D Failure of Sterilization 30,000
fortnight (July 11 – 24, 2017)
E Doctors/facilities covered for 2,00,000
litigations up to 4 cases per year (per case) The event was observed over a month long period, split
including defense cost into an initial fortnight of mobilization/ sensitization
followed by a fortnight of assured family planning
The Hon’ble Supreme Court has given specific service delivery.
directions in its order dated 14.09.2016, whereby the
• June 27 to July 10, 2017: “Dampati Sampark
quantum of compensation fixed under the FPIS has
Pakhwada” or “Mobilisation Fortnight” was
been doubled, with the balance being paid from the
organised.
State health budget.
• July 11 to July 24, 2017: “Jansankhya Sthirtha
6.6.1 Scheme of Home delivery of contraceptives
Pakhwada” or “Population Stabilisation
by ASHAs at doorstep of beneficiaries
Fortnight” was organised.
• Community based distribution of contraceptives
The National level workshop on World Population
by involving ASHAs and focused IEC/BCC
Day was celebrated in collaboration with Jansankhya
efforts are undertaken for enhancing demand
Sthirata Kosh (JSK) at Vigyan Bhavan. The workshop
and creating awareness on family planning.
in Vigyan Bhavan on “Parivar Niyojan-Sashakt
To improve access to contraceptives by the
Samaj, Rashtra ka Vikas” was presided over by the
eligible couples, services of ASHA are utilised
Hon’ble Union Minister of Health & Family Welfare,
to deliver contraceptives at the doorstep of
Shri J.P.Nadda and Union Minister of State for Health
beneficiaries. The scheme has been rolled out
& Family Welfare, Ms. Anupriya Patel.
in all the districts of the country.
The day marked a series of launches, with the family
• Under HDC scheme, ASHAs are distributing
planning division endeavouring towards promoting
condoms, OCPs and ECPs in all States of India.
good reproductive health practices of the masses.
Annual Report | 2017-2018 101
Chapter - 06
• Mission Parivar Vikas: A programme launched Programme” and Oral contraceptive pill
in 146 high TFR districts to accelerate the use Centchroman “CHHAYA” have been added to
and awareness of family planning methods. the existing contraceptive basket of choice thus
State and district fact sheets were unveiled providing users with new options.
at the occasion. The fact sheets highlight the
current indicators and trends in these districts • Media Campaign Phase 2: The Ministry of
and will act as the baseline and roadmap for Health and Family Welfare launched the phase 2
future work in these districts. of the media campaign. A multimedia campaign
was designed with an objective to reaching out
• New Contraceptives Launch: The new to people of all age groups, regions and strata
contraceptive Injectable MPA under “Antara of the society. The idea was to resonate with the
Hon’ble Union Minister for Health & Family Welfare Shri J.P. Nadda distributing awards to children - winners of
painting competition on World Population Day 2017
culture of the target audience and bring about a Anupriya Patel to school children who brought laurels
positive change in the use of contraception and to their schools by winning prizes in the painting
shattering the myths around it. competition organized by Jansankhya Sthirata Kosh.
• Family Planning Logistic Information The inaugural session was followed by a panel
System (FP-LMIS): The new commodity discussion which was led by Dr R.K. Vats, AS and
tracking software called FP-LIMS was launched DG (CGHS). The panel comprised of experts – Dr.
to ensure commodity tracking and a smooth S.K. Sikdar, Dr. Rishma Dhillon Pai, Dr. J. K. Das,
delivery system. The software assures to solve Mr. Diego Palacios (UNFPA), Mr. Alkesh Wadhwani
any gap in the commodity delivery system and (BMGF), Ms. Marietou Satin (USAID) and Ms. Preeti
bridge in any gaps. Nath – who presided over the discussion.
The inaugural session of the workshop also witnessed Services Rendered during World Population
prize distribution by the Hon’ble Union Minister Fortnights
of Health & Family Welfare, Shri J. P. Nadda and
Minister of State for Health & Family Welfare, Ms. The overall performance during the fortnight (11th –
24th July, 2017) is as follows:
102 Annual Report | 2017-2018
Chapter - 06
Sl. No. Method 2015 2016 2017*
1 Female Sterilization 1,42,372 1,45,372 1,49,315
2 Male Sterilization 6,035 7,101 5,973
Total Sterilization 1,48,407 1,52,106 1,55,288
3 IUCD Insertions 3,51,444 3,74,880 3,25,321
4 PPIUCD Insertions 43,829 72,433 85756
*Note: Andaman and Nicobar Island and Lakshadweep have not submitted the report.
Some States extended their service provision days The theme for vasectomy fortnight this year was:
further. The States of Assam and Bihar extended their
services till 31st July, 2017 and Jharkhand till 16th “Zimmedar Purush ki yehi hai Pehchan,
August. The total sterilizations that took place during Parivar Niyojan mein jo de Yogdaan”
the WPD fortnight are 1.55 lakhs of which female
sterilizations account for 1.49 lakhs and there were ^^ftEesnkj iq#"k dh ;gh gS igpku]
5973 male sterilizations. The increase in PPIUCD ifjokj fu;kstu esa tks ns ;ksxnku¸
has been on the increasing side with 85,756 insertions
being reported this year. A National Workshop on promotion of male
participation in Family Planning was held on 16th
In female sterilization, Bihar reported the highest November, 2017 under the chairmanship of Ms.
performance, with 22392 female sterilizations, Vandana Gurnani, JS (RCH), with the aim to strengthen
followed by West Bengal (16892) and Odisha
the advocacy on male engagement in family planning
(12650). West Bengal (1135) reported the highest
– wherein opportunities and strategies to engage men
male sterilization followed by Chhattisgarh (994) and
holistically as change makers, responsible partners,
Assam (888).
allies, torchbearers of transformation and gatekeepers
The total IUCD’s (Interval and PPIUCD) inserted of their families were deliberated upon with the active
were 391108 of which Interval IUCD insertions are participation of close to 150 participants from various
314545 and PPIUCD insertions are 76563.The highest International agencies, Development Partners, Civil
Interval IUCD insertions were reported in West Society and officials and NSV surgeons from the State
Bengal (61465) followed by Uttar Pradesh (44334) Government.
and Assam (34599). The PPIUCD insertions were
reported to be the highest in Uttar Pradesh (15023), The Vasectomy fortnight was observed by all the
West Bengal (13245) and Bihar (10472). States/UT for creating awareness on male participation
6.6.4 Observation of Vasectomy Fortnight under FP Programme, generating demand and
(November 21 – December 4, 2017) providing Family Planning services. Mobility
publicity vans were arranged at various levels for
The Vasectomy Fortnight was observed for a fortnight demand generation activities. Sensitization meetings
across the country. The fortnight was split into two were held at the district and block levels to generate
phases: awareness and address the myths and misconceptions
• “Mobilisation Phase” between 21st November related to vasectomy. Health centres were identified in
to 27th November, 2017 the districts and dedicated team of doctors and nurses
were present for the entire fortnight to render FP
• “Service Delivery Phase” between 28th services. Private accredited providers were also roped
November - 4th December, 2017 in for service provision during the fortnight.
Annual Report | 2017-2018 103
Chapter - 06
Services Rendered during Vasectomy Fortnight
The overall performance* during the fortnight (21st November - 4th December, 2017) is as follows:-
Sl.N. Method 2016 2017
1 Number of facilities providing vasectomy services during the service 2623 3129
delivery week
Number of vasectomies conducted during the service delivery week 8083 10,804
2 Total number of condom boxes installed during the service delivery - 56,241
week
Number of condom pieces distributed during the service delivery 36,09,962 53,17,121
week
* Note: - Based on Reports received from 27 States.
10,804 vasectomies were done during the NSV fortnight 2017, an increase of 30% over the last year’s performance.
Chhattisgarh recorded the maximum vasectomies with 2469 vasectomies, followed by Maharashtra (1968)
and Assam (1350). 53,17,121 condom pieces were distributed during the vasectomy week 2017. West Bengal
distributed the highest number of condom pieces at 12,99,244 followed by Maharashtra (7,15,138), Punjab
(5,71,341) and Rajasthan (4,96,971).
104 Annual Report | 2017-2018
Chapter - 06
Annexure - 1
Number Sterilisations and IUCDs by States 2017-18 (Up to December)
States Female Male Total IUCD
Sterilisation Sterilisation Sterilisation
Bihar 2,28,980 1274 2,30,254 2,12,281
Chhattisgarh 30,920 5,988 36,908 69,794
Himachal Pradesh 3,140 172 3312 10,766
Jammu & Kashmir 6,601 140 6747 12,961
Jharkhand 27,455 859 28,314 57,019
Madhya Pradesh 1,73,307 1,973 1,75,280 1,72,720
Odisha 41,607 534 42,141 63,030
Rajasthan 31,379 642 30,737 24,290
Uttar Pradesh 1,22,090 3461 33,213 5,15,516
Uttarakhand 5,378 304 5,672 33,733
Arunachal Pradesh 680 1 679 1,708
Assam 24,447 2,264 26,711 65,014
Manipur 525 44 525 2,595
Meghalaya 1,806 8 1,814 2,587
Mizoram 595 0 595 975
Nagaland 1,214 5 1,219 3,223
Sikkim 81 4 85 446
Tripura 1,197 12 1197 747
Andhra Pradesh 1,34,790 986 1,35,776 55,080
Goa 1,565 4 1,569 670
Gujarat 1,67,332 1,653 1,68,985 3,83,801
Haryana 28,774 1,183 29,957 76,752
Karnataka 2,22,130 65 2,22,786 1,00,698
Kerala 23,264 29 23,557 17,897
Maharashtra 2,78,380 1,973 2,87,222 2,07,491
Punjab 26,965 819 27,784 91,246
Telangana 50,104 3101 53,205 14,339
Tamil Nadu 1,61,960 400 1,62,360 2,00,964
West Bengal 1,11,119 3,326 1,14,445 1,86,529
A & N Islands 215 0 215 70
Chandigarh 1,671 20 1,691 1,938
Dadra & Nagar Haveli 925 6 931 251
Daman & Diu 211 0 211 86
Delhi 10,591 335 10,926 25,405
Lakshadweep 31 0 31 7
Puducherry 4,761 4 4,765 871
TOTAL 19,26,339 39,323 19,65,662 2613590
Source: HMIS
Annual Report | 2017-2018 105
Chapter - 06
6.7 procurement and supply of remaining quantities, open tenders are advertised for
CONTRACEPTIVES procurement from private firms.
The Department of Health and Family Welfare is Quality Assurance: Manufacturers do in-house
responsible for implementation of the National Family testing of stores before offering them for inspection. At
Welfare Programme by, inter-alia, encouraging the the time of acceptance of stores, random samples from
utilization of contraceptives and distribution of the all the batches are picked up and tested in certified lab
same to the States/UTs under Free Supply Scheme and in receipt of ok reports, stores are supplied to the
and Public-Private Partnership (PPP) under Social consignees.
Marketing Scheme. Under Free Supply Scheme,
contraceptives such as Condoms, Oral Contraceptive 6.7.1 Free Supply Scheme: Under Free Supply
Pills, Intra Uterine Device (Cu-T), Emergency Scheme, contraceptives viz. Condoms, Oral
Contraceptive Pills and Tubal Rings are procured Contraceptives Pills (OCPs) (Mala-N), Intra Uterine
and supplied free to the States/UTs. Injectable Device (Copper-T), Tubal Rings, Emergency
Contraceptive (Antara Programme) and Centchroman Contraceptive Pills (ECPs), Injectable Contraceptive,
Contraceptive Pill viz. Chhaya have been introduced Centchroman Contraceptive Pill, Pregnancy Testing
in 2016-17 in Free Supply Scheme. Kits (PTKs) are procured and supplied to the States
with the objective of making them available free of
Procurement procedures: Orders for 75% of the cost to those who cannot afford to pay for it. These are
requirement in case of condoms and 55% of requirement supplied free of cost to the users through dispensaries,
for other contraceptives are placed on HLL Lifecare hospitals, PHCs, Sub Centres etc.
Ltd. (a PSU under the Ministry of Health & FW) for
procurement of contraceptives being manufactured by The following quantities of contraceptives were
them as per captive status awarded to them. For the procured for supply to States during 2016-17
(Including CMSS) and 2017-18:
Item 2016-17 2017-18 *
(Including CMSS) (up to Aug. 2017)
Quantity Value Quantity Value
(Rs. in Crore) (Rs. in Crore)
Condoms (Free Supply) (Million Pieces) 432.82 69.29 206.37 32.92
OCPs (Free Supply) (Lakh Cycles) 311.98 12.15 106.30 04.04
*Figures are Provisional
Item 2016-17 (Including CMSS) 2017-18 *
(up to Aug. 2017)
Quantity Value Quantity Value
(Rs. in Crore) (Rs. in Crore)
Copper – T (Lakh pcs.) 48.11 8.00 11.31 02.71
(IUD 380A, IUD 375)
Tubal Ring (Lakh Pairs) 6.39 01.06 1.28 00.22
ECP (Lakh Packs) 60.83 00.89 12.33 00.27
Centchroman Contraceptive Pill (Lakh Strips) 7.13 1.78 19.00 04.56
Injectable Contraceptive (Lakh doses) -- -- 27.00 07.43
PT Kits (Lakh Kits) 124.60 5.00 44.25 01.77
*Figures are Provisional
106 Annual Report | 2017-2018
Chapter - 06
6.7.2 Social Marketing Scheme Presently, one Government brand (Deluxe Nirodh) and
12 different SMOs brands of condoms (i.e. Rakshak,
The National Family Welfare Programme initiated the Ustad, Josh, Mithun, Style, Thril, Kamagni, Sawan,
Social Marketing Programme of Condoms in 1968 and Milan, Bliss, Ahsaas and KLY-MAX) are sold in the
that of Oral Pills in 1987. On the advice of Planning market through SMOs. Similarly for Oral Pills, one
Commission (Now NITI Aayog) and Ministry of Government brand (Mala-D) and seven SMOs brands
Finance, a study was conducted by UNFPA to evaluate of Pills (i.e. Arpan, Pearl, Ecroz, Sunehri, Apsara,
the Social Marketing Scheme which submitted the Khushi and Smartt Cycle) are sold.
report in December, 2015. The recommendations of
UNFPA were examined in the Ministry and the Social SMOs have sold the following quantities during 2016-
Marketing Programme was rejuvenated. The price 17 & 2017-18 (upto June/Sept. 2017):
of the SMO brand contraceptives i.e Deluxe Nirodh
(Govt. Brand) was revised from Rs. 3/- for a pack of 5 Sale of Condoms (Quantity in Mpcs.)
pieces to Rs.5/- for a pack of 5 pieces and SMO brand Sl. Social Marketing 2016-17 2017-18
condoms from Rs. 2.00 for one piece to a maximum of No. Organization (Provisional)
Rs. 3.33 per piece ( Rs. 10.00 for a pack of 3 pieces).
The price of the oral pills of Govt. Brand and SMO 1. HLL Lifecare Ltd, 354.00 37.97*
brand has also been revised i.e. Mala –D (Govt. Brand) Thiruvananthapuram
from Rs.3.00 per cycle to Rs. 5.00 per cycle while the 2. Parivar Seva Sanstha, 00.00 00.00
SMO brand price range was retained at a maximum Delhi
price of Rs. 10.00 per cycle. SMOs have the flexibility 3. Janani, Patna 08.00 4.70*
to fix the price of branded condoms and OCPs within 4. Population Health 35.00 7.60**
the range fixed by the Government. Condoms and services (I)
Oral Pills are made available to the people at highly Hyderabad
subsidized rates, through diverse outlets. Promotional
and Packaging incentives which were being 5. PCPL, Kolkata 00.00 NR
reimbursed to the SMOs has been withdrawn after 6. World Health Partner 2.00 NR
revision of prices of Condoms and Oral Contraceptive Total 399.00 50.27
Pills (OCPs). The issue price of both condom and
OCP has been retained at Rs.0.40 per condom and *Upto June, 2017
Rs.1.60 per cycle of OCPs. The SMOs are required **Upto September, 2017
to be remit 35% advance payment to the Government
before placement of indent for the value of quantity of Sale of Oral Contraceptive Pills (Quantity in Lakh
stock intended by them and the balance 65% payment Cycles)
shall be remitted in the form of bank guarantee at the
Sl. Social Marketing 2016-17 2017-18 *
time of remitting 35% payment. The balance 65%
No. Organisation (up to Aug.
amount of the issue price of both Condom and Oral
2017)
Contraceptive Pills for which bank guarantee was given
1 HLL Lifecare Ltd., 139.61 15.78
by SMOs should be paid by the SMO to Government
Thiruvananthapuram
by Demand Draft at the time of issue of release orders
to reduced financial burden on them. The agreements 2 Parivar Seva Sanstha, Delhi 5.52 NR
with the SMOs are now signed for a period of three 3 Janani, Patna 4.77 10.62
years to facilitate SMOs to plan their activities for a 4 Population Health services, 41.00 6.00
longer period. The extent of subsidy ranges from 70% Hyderabad
to 85% depending upon the procurement price in a 5 PCPL, Kolkata NR NR
given year. Both these contraceptives are distributed 6 World Health Partner, New 3.38 NR
through Social Marketing Organizations (SMOs). Delhi
There are presently seven SMOs registered viz. HLL Total 194.28 32.40
Lifecare Ltd., PHS(I), PCPL, Janani, PSS, World
Health Partner and DKT (I) (Recently registered). *Figures are Provisional
Annual Report | 2017-2018 107
Chapter - 06
6.7.3 Centchroman (Oral Pills) 6.8 Central Medical Supplies
Society (CMSS)
Since December, 1995, a non-steroidal weekly Oral
Contraceptive Pill, Centchroman (Popularly known as With a view to assure procurement and distribution
Saheli & Novex), to prevent pregnancy is also being of supplies in time, the government has now set up
subsidized under the Social Marketing Programme. an autonomous agency viz. Central Medical Supplies
The weekly Oral pill is the result of indigenous research Society (CMSS) whose sole responsibility would be
of CDRL, Lucknow. The pill is now available in the to ensure uninterrupted supplies of commodities in the
market at Rs. 3.125 per tablet (Rs. 25/- per strip of 8 States. This agency would be able to cut the proverbial
tablets). The Government of India provides a subsidy bureaucratic tape by laying down a firm procurement
of Rs. 2.51 per tablet towards product and promotional and distribution system in the country, thereby
subsidy. transforming the committed goals into a reality. A
statement showing the quantities of contraceptives
Performance of Social Marketing Programme in procured from private manufacturers during 2016-17
the sale of contraceptives and 2017-18 (upto August, 2017) by CMSS alongwith
the indent for 2017-18 is given below:
Item 2016-17 2017-18 *
(up to Aug.
2017)
Condoms (Million Pieces) 399.00 50.27
Oral Pills(Social 194.28 32.40
Marketing) (Lakh Cycles)
SAHELI (Lakh Tablets) 321.76 0.04160
*: Figures are Provisional
Sl. Item Quantity Quantity Quantity Value (Rs. in
No. Procured Indented Procured in Crore) for
in 2016-17 for 2017-18 2017-18 up to procurement upto
August, 2017* August, 2017
1. Condoms (Million Pieces)
Free Supply 155.13 137.58 114.11 18.22
SMO Brand 113.50 277.75 314.13 47.06
Free Supply for NACO 56.42 39.40 68.04 10.75
2. OCP (Lakh Cycles)
Free Supply 139.21 115.96 141.39 05.37
SMO Brand 36.90 147.60 82.83 03.42
3. EC Pills (Lakh Packs) 56.64 20.18 25.78 00.57
4. IUCDs/Copper–T (in Lakh Pieces) 44.34 18.50 -- --
5. Tubal Rings (in Lakh Pairs) 6.39 2.09 9.92 01.72
6. Pregnancy Test Kits (PTK) (in 46.04 72.41 91.91 03.69
Lakh Pieces /Kits)
*Figures are Provisional
108 Annual Report | 2017-2018
S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Eugenics: K.Jeyanthi Shanmugam Associate Professor RVS College of Nursing, Sulur, CoimbatoreDocument10 paginiEugenics: K.Jeyanthi Shanmugam Associate Professor RVS College of Nursing, Sulur, CoimbatoresanthiyasandyÎncă nu există evaluări
- AbortionDocument39 paginiAbortionMerielLouiseAnneVillamilÎncă nu există evaluări
- Continental Steel Manufacturing Corporation vs. MontanoDocument1 paginăContinental Steel Manufacturing Corporation vs. MontanoEthan Kurby100% (1)
- Position PaperDocument6 paginiPosition PaperZeñun Olegna RehmÎncă nu există evaluări
- Prenatal Development Final 1Document4 paginiPrenatal Development Final 1api-447499660Încă nu există evaluări
- Pro Con ChartDocument2 paginiPro Con Chartapi-410305129100% (1)
- 》 The first two weeks after conception 》: Germinal StageDocument4 pagini》 The first two weeks after conception 》: Germinal StageMichelle ArregLado VistalÎncă nu există evaluări
- Surrogacy Laws in IndiaDocument20 paginiSurrogacy Laws in IndiaSUDHIR'S PHOTOGRAPHYÎncă nu există evaluări
- Disenfranchised Grief 10.22Document20 paginiDisenfranchised Grief 10.22dofiajoijÎncă nu există evaluări
- Senate Democrats & Governor Cuomo Call For Roe v. Wade CodificationDocument4 paginiSenate Democrats & Governor Cuomo Call For Roe v. Wade CodificationNew York State Senate Democratic ConferenceÎncă nu există evaluări
- Medical Termination of Pregnancy (MTP) Act, 1971 Gp2Document12 paginiMedical Termination of Pregnancy (MTP) Act, 1971 Gp2Guru PrasadÎncă nu există evaluări
- Sentence Gap Filling AdvancedDocument3 paginiSentence Gap Filling Advancedrencsi0611Încă nu există evaluări
- Child AbortionDocument12 paginiChild AbortionShada Banguih Dela TorreÎncă nu există evaluări
- Abortion Final DraftDocument7 paginiAbortion Final DraftKaleo Regalmuto0% (1)
- Ukraine Baby FactoriesDocument14 paginiUkraine Baby Factories3adrianÎncă nu există evaluări
- AbortionDocument28 paginiAbortionjeanpesky100% (4)
- Therapeutic AbortionDocument2 paginiTherapeutic Abortionapi-224695265Încă nu există evaluări
- Abortion - Constructive SpeechDocument4 paginiAbortion - Constructive SpeechRydl Pnp100% (1)
- Dont Split The Baby How The Us Could Avoid Uncertainty and Unnecessary Litigati PDFDocument32 paginiDont Split The Baby How The Us Could Avoid Uncertainty and Unnecessary Litigati PDFSean CouttsÎncă nu există evaluări
- Asis ProjectDocument6 paginiAsis Projectmercy relotaÎncă nu există evaluări
- BibliographyDocument3 paginiBibliographyKim Andrei Estrella ApeñaÎncă nu există evaluări
- OG Informing Abortion Debate DR Christine BaileyDocument2 paginiOG Informing Abortion Debate DR Christine BaileyYwagar YwagarÎncă nu există evaluări
- A Synoptic Essay About Birth Control in The PhilippinesDocument10 paginiA Synoptic Essay About Birth Control in The PhilippinesJulie AbanesÎncă nu există evaluări
- AbortionDocument11 paginiAbortionKopal GargÎncă nu există evaluări
- Legalizing Male Sterilization in MyanmarDocument16 paginiLegalizing Male Sterilization in MyanmarHla Myat TunÎncă nu există evaluări
- SHS 12 CLF 3: BioethicsDocument2 paginiSHS 12 CLF 3: BioethicsjulianaÎncă nu există evaluări
- Policy On Family PlanningDocument2 paginiPolicy On Family PlanningLILIW RHUÎncă nu există evaluări
- Senate Bill No 2635Document5 paginiSenate Bill No 2635CBCP for LifeÎncă nu există evaluări
- 11 Imbong vs. Ochoa 721 Scra 146Document4 pagini11 Imbong vs. Ochoa 721 Scra 146Beatta Ramirez0% (1)
- Issues of Maternal and Child HealthDocument10 paginiIssues of Maternal and Child Healthjeelani saima100% (2)