S-ar putea să vă placă și
- Deep Vein ThrombosisDocument11 paginiDeep Vein ThrombosisTushar GhuleÎncă nu există evaluări
- Unilateral Leg Swelling 1Document67 paginiUnilateral Leg Swelling 1maryam tariqÎncă nu există evaluări
- Thrombophl Ebitis: Santos, Maria Ericka B. BSN Iii - 1Document39 paginiThrombophl Ebitis: Santos, Maria Ericka B. BSN Iii - 1Ericka SantosÎncă nu există evaluări
- Deep Vein Thrombosis (DVT) ExplainedDocument29 paginiDeep Vein Thrombosis (DVT) ExplainedAuliyah SeptianiÎncă nu există evaluări
- DR LulukDocument32 paginiDR LulukluckyariadneeÎncă nu există evaluări
- DEEP VEIN Dr. Samira BelkheirDocument43 paginiDEEP VEIN Dr. Samira BelkheirkalfÎncă nu există evaluări
- Deep Venous Thrombosis: Farouq Muhammad 6-10-11Document59 paginiDeep Venous Thrombosis: Farouq Muhammad 6-10-11farouqmuhdÎncă nu există evaluări
- DVT MatisseDocument31 paginiDVT MatisseMaretha Dyah AnggrainiÎncă nu există evaluări
- Brunner and Suddarth's Textbook of Medical-Surgical Nursing 12th Ed. (Dragged) 6Document1 paginăBrunner and Suddarth's Textbook of Medical-Surgical Nursing 12th Ed. (Dragged) 6jamie carpioÎncă nu există evaluări
- Superficial Venous Thrombophlebitis: Presented by - Nader SaadDocument24 paginiSuperficial Venous Thrombophlebitis: Presented by - Nader SaadNader SaadÎncă nu există evaluări
- Deep Vein Thrombosis (DVT): Causes, Symptoms and TreatmentDocument12 paginiDeep Vein Thrombosis (DVT): Causes, Symptoms and TreatmentJohn Jacob100% (1)
- The Management of DVT: Dr. Heru Sulastomo, SP - JP (K), FIHA Dr. Ahmad Yasa', SP - JP, FIHA, MkesDocument19 paginiThe Management of DVT: Dr. Heru Sulastomo, SP - JP (K), FIHA Dr. Ahmad Yasa', SP - JP, FIHA, MkesDEWI MULYANIÎncă nu există evaluări
- DVT Blok 4.1Document67 paginiDVT Blok 4.1Dz Putra100% (1)
- DVTDocument20 paginiDVTNachiket Vijay PotdarÎncă nu există evaluări
- Nicyela Vascular DiseaseDocument21 paginiNicyela Vascular DiseaseNicyela JillienÎncă nu există evaluări
- Update On The Management of Venous ThromboembolismDocument8 paginiUpdate On The Management of Venous ThromboembolismRoberto López MataÎncă nu există evaluări
- Deep Vein ThrombosisDocument15 paginiDeep Vein ThrombosisAngela TenorioÎncă nu există evaluări
- Swelling in LegDocument3 paginiSwelling in LegNeeraj SethiÎncă nu există evaluări
- Venous Thromboembolism in Urologic Surgery: Prophylaxis, Diagnosis and TreatmentDocument25 paginiVenous Thromboembolism in Urologic Surgery: Prophylaxis, Diagnosis and TreatmentapheatÎncă nu există evaluări
- DVT SlideDocument21 paginiDVT SlideAlifiah100% (1)
- Deep Vein ThrombosisDocument42 paginiDeep Vein ThrombosisNsklm100% (7)
- DVT Deep Vein ThrombosisDocument19 paginiDVT Deep Vein ThrombosisDoctor MusicÎncă nu există evaluări
- Kuliah DVTDocument29 paginiKuliah DVTluluksÎncă nu există evaluări
- DVT Diagnosis and TreatmentDocument56 paginiDVT Diagnosis and TreatmentSrikant Konchada100% (1)
- Thrombosis Prevention by SlidesgoDocument67 paginiThrombosis Prevention by SlidesgoRohanÎncă nu există evaluări
- Venous Thromboembolism (Pe and DVT)Document31 paginiVenous Thromboembolism (Pe and DVT)NinaÎncă nu există evaluări
- Deep Venous ThrombosisDocument22 paginiDeep Venous ThrombosisLenutza LenutaÎncă nu există evaluări
- Management of Rheumatic Heart Disease: Quick Reference Guide For Health ProfessionalsDocument4 paginiManagement of Rheumatic Heart Disease: Quick Reference Guide For Health ProfessionalsgireeshsachinÎncă nu există evaluări
- Deep Vein ThrombosisDocument13 paginiDeep Vein ThrombosislucyishakÎncă nu există evaluări
- VTE Prophylaxis in The Hospital: Johan KurniandaDocument35 paginiVTE Prophylaxis in The Hospital: Johan KurniandaadystiÎncă nu există evaluări
- Dr. Witra Irfan, SP.B (K) V - DVTDocument29 paginiDr. Witra Irfan, SP.B (K) V - DVTmuhammad azharanÎncă nu există evaluări
- BrowneDVT and PTSDocument44 paginiBrowneDVT and PTSUddin Mohammad SharafÎncă nu există evaluări
- DVT Guide: Causes, Symptoms and Treatment of Deep Vein ThrombosisDocument46 paginiDVT Guide: Causes, Symptoms and Treatment of Deep Vein ThrombosisLuqman ArifÎncă nu există evaluări
- Kuliah Thrombosis 2015 NNDocument39 paginiKuliah Thrombosis 2015 NNBeladiena Citra SiregarÎncă nu există evaluări
- Cardiovascular-Disorders Group4 3NFDocument10 paginiCardiovascular-Disorders Group4 3NFDarren RobertoÎncă nu există evaluări
- Venous Thromboembolism Pathophysiology and TreatmentDocument11 paginiVenous Thromboembolism Pathophysiology and TreatmentPindha Kurnia JatiÎncă nu există evaluări
- 2.4. Vena LimfeDocument28 pagini2.4. Vena Limfeira citraÎncă nu există evaluări
- UPDATE MENEJEMEN DVTDocument9 paginiUPDATE MENEJEMEN DVTSupandy HasanÎncă nu există evaluări
- C24 LymphaticsDocument23 paginiC24 LymphaticsErneslito LucasÎncă nu există evaluări
- Venous ThromboembolismDocument28 paginiVenous ThromboembolismValeria MolinaÎncă nu există evaluări
- Deep Vein Thrombosis (DVT)Document9 paginiDeep Vein Thrombosis (DVT)Dian PrastiwiÎncă nu există evaluări
- Apixaban Cme SlidesDocument26 paginiApixaban Cme SlidesBharat GuptaÎncă nu există evaluări
- Deep Vein ThrombosisDocument16 paginiDeep Vein ThrombosisB1 TutorialÎncă nu există evaluări
- Treatment and Complications of Chronic Liver DiseaseDocument40 paginiTreatment and Complications of Chronic Liver DiseaseRisydaMKhÎncă nu există evaluări
- WCS 001 - Varicose Veins - by Prof SWK ChengDocument4 paginiWCS 001 - Varicose Veins - by Prof SWK ChengRachelMokÎncă nu există evaluări
- Gastroesophagal VaricesDocument21 paginiGastroesophagal VaricesNurulasyikin MAAÎncă nu există evaluări
- Pulmonary Embolism & Deep Vein Thrombosis Definitions: Virchow's TriadDocument7 paginiPulmonary Embolism & Deep Vein Thrombosis Definitions: Virchow's TriadCitra Eva MeilyndhaÎncă nu există evaluări
- Anticoagulation in OrthopedicsDocument32 paginiAnticoagulation in Orthopedicsehabede6445Încă nu există evaluări
- HIS1-K36 VTE, Diagnosis Klinis DVTDocument26 paginiHIS1-K36 VTE, Diagnosis Klinis DVTPaul Behring ManurungÎncă nu există evaluări
- Pharmacotherapy of VTEDocument80 paginiPharmacotherapy of VTEAbera JamboÎncă nu există evaluări
- Deep Vein Thrombosis & Its ProphylaxisDocument90 paginiDeep Vein Thrombosis & Its ProphylaxisPratik KumarÎncă nu există evaluări
- Deep Vein Thrombosis / Pulmonary EmbolismDocument55 paginiDeep Vein Thrombosis / Pulmonary EmbolismSenti AnnamalaiÎncă nu există evaluări
- KP 2.5.4.5 VteDocument96 paginiKP 2.5.4.5 Vtenurul ramadhiniÎncă nu există evaluări
- Risks of DVT and Prevention StrategiesDocument12 paginiRisks of DVT and Prevention StrategiesShilpaÎncă nu există evaluări
- Venous ThromboembolismDocument26 paginiVenous ThromboembolismShivam SoniÎncă nu există evaluări
- Venous Thromboembolism LumabanDocument17 paginiVenous Thromboembolism LumabanBEA RADAÎncă nu există evaluări
- Venous ThromboembolismDocument6 paginiVenous ThromboembolismAkhilaÎncă nu există evaluări
- Cerebrovascular Hypertension by John Dickinson and Julian PatonDocument272 paginiCerebrovascular Hypertension by John Dickinson and Julian PatonPaul DickinsonÎncă nu există evaluări
- Sympathomimetics in VeterinaryDocument9 paginiSympathomimetics in Veterinaryjose pÎncă nu există evaluări
- Diploma in Human Anatomy and PhysiologyDocument2 paginiDiploma in Human Anatomy and PhysiologyNaveed SakiÎncă nu există evaluări
- CT 2Document16 paginiCT 2TGB LEGENDÎncă nu există evaluări
- Aortic Regurgitation PathophysiologyDocument1 paginăAortic Regurgitation Pathophysiologydana100% (1)
- IsdnDocument5 paginiIsdnWidya JelitaÎncă nu există evaluări
- FREE 2021 ACLS Study Guide - ACLS Made Easy!Document32 paginiFREE 2021 ACLS Study Guide - ACLS Made Easy!Alen ArguellesÎncă nu există evaluări
- Heart Failure - 2022Document106 paginiHeart Failure - 2022Rana Khaled AwwadÎncă nu există evaluări
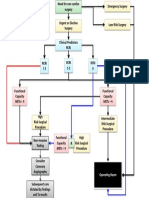
- Cardiac Risk Assessemnt FlowchartDocument1 paginăCardiac Risk Assessemnt FlowchartjamesomooreÎncă nu există evaluări
- Nursing Care Plan For Myocardial InfarctionDocument7 paginiNursing Care Plan For Myocardial InfarctionRocelyn CristobalÎncă nu există evaluări
- Management Arteriosclerosis and ClaudicationDocument41 paginiManagement Arteriosclerosis and ClaudicationLuqman AlwiÎncă nu există evaluări
- Cardiac CycleDocument2 paginiCardiac CycleU Than HanÎncă nu există evaluări
- Tensiometro Cvs PharmacyDocument38 paginiTensiometro Cvs PharmacyAlfredo PonsÎncă nu există evaluări
- Cor PulmonaleDocument14 paginiCor PulmonaleEvangelin MelvinÎncă nu există evaluări
- Protocolo FATE (Eco TT)Document4 paginiProtocolo FATE (Eco TT)darlingcarvajalduqueÎncă nu există evaluări
- Lipid Metabolism and Health - EBOOKOID PDFDocument377 paginiLipid Metabolism and Health - EBOOKOID PDFniluh suwasantiÎncă nu există evaluări
- WBI01 01 Que 20180109Document24 paginiWBI01 01 Que 20180109Anonymous D2HJ7g4OÎncă nu există evaluări
- DORVDocument33 paginiDORVjayasiinputÎncă nu există evaluări
- HypertensionDocument12 paginiHypertensionDr. PARMINDER NAINÎncă nu există evaluări
- Acls Drug OverviewDocument2 paginiAcls Drug OverviewBruce Abramowitz100% (1)
- Activity 1 - Effect of Blood Vessel Radius On Blood Flow Rate PDFDocument5 paginiActivity 1 - Effect of Blood Vessel Radius On Blood Flow Rate PDFTadhg Ó MaoldhomhnaighÎncă nu există evaluări
- Drugs primarily eliminated by liver or kidneysDocument2 paginiDrugs primarily eliminated by liver or kidneysCarl LeeÎncă nu există evaluări
- InterdiabDocument385 paginiInterdiabMihaela IonescuÎncă nu există evaluări
- Dental Management of The Medically Compromised Patient 8Th Ed by Little - Test BankDocument12 paginiDental Management of The Medically Compromised Patient 8Th Ed by Little - Test Bankkritisarena100% (1)
- The Non Invasive Assessment of VascularDocument39 paginiThe Non Invasive Assessment of VascularLilia RadjefÎncă nu există evaluări
- Amity College of Nursing: Nursing Care Plan ON Heart FailureDocument20 paginiAmity College of Nursing: Nursing Care Plan ON Heart Failurejyoti puniaÎncă nu există evaluări
- Cardiorespiratory SystemDocument19 paginiCardiorespiratory SystemEmanuel JheadÎncă nu există evaluări
- Cardio Vascular System NursingDocument2 paginiCardio Vascular System NursingGade BalajiÎncă nu există evaluări
- Drug Study - DigoxinDocument2 paginiDrug Study - DigoxinKian Herrera50% (2)
- ABC of Clinical Electrocardiography Atrial ArrhythmiasDocument6 paginiABC of Clinical Electrocardiography Atrial ArrhythmiasIgnacio Aguilar ValdiviesoÎncă nu există evaluări