S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Peña-Casanova, J., et al. (2009). Spanish Multicenter Normative Studies (NEURONORMA Project). Norms for the Rey–Osterrieth Complex Figure (Copy and Memory), and Free and Cued Selective Reminding TestDocument23 paginiPeña-Casanova, J., et al. (2009). Spanish Multicenter Normative Studies (NEURONORMA Project). Norms for the Rey–Osterrieth Complex Figure (Copy and Memory), and Free and Cued Selective Reminding TestLuis GómezÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- (Macaulay, M. & Macmillan, M.) The Concept of Mental Age and MaturationDocument4 pagini(Macaulay, M. & Macmillan, M.) The Concept of Mental Age and MaturationLuis GómezÎncă nu există evaluări
- Benson, D. Et Al. (1988) Posterior Cortical AtrophyDocument5 paginiBenson, D. Et Al. (1988) Posterior Cortical AtrophyLuis GómezÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Supplementary Figure 1. Negligible Effects of Covarying For Different Tracer Injection ParametersDocument6 paginiSupplementary Figure 1. Negligible Effects of Covarying For Different Tracer Injection ParametersLuis GómezÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Benson, D. Et Al. (1988) Posterior Cortical AtrophyDocument5 paginiBenson, D. Et Al. (1988) Posterior Cortical AtrophyLuis GómezÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- 1 FCRDocument1 pagină1 FCRLuis GómezÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Anak Coba ImiDocument18 paginiAnak Coba ImiMarchelina Benediktin KaunangÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- (Greenspan, N.) Autism, Evolution, and The Inadequacy of SpectrumDocument4 pagini(Greenspan, N.) Autism, Evolution, and The Inadequacy of SpectrumLuis GómezÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Neurobiology of AgingDocument11 paginiNeurobiology of AgingLuis GómezÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The 2D:4D Ratio and Its Relationship With Other Androgenisation Parameters in Parents of Individuals With Autism Spectrum DisordersDocument8 paginiThe 2D:4D Ratio and Its Relationship With Other Androgenisation Parameters in Parents of Individuals With Autism Spectrum DisordersLuis GómezÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Genetics and Epigenetics of Autism Spectrum DisorderDocument11 paginiGenetics and Epigenetics of Autism Spectrum DisorderPAULAÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Caracteristicas Fisicas y Fenotipo Conductual - Galvan Manso y Otros - ArticuloDocument5 paginiCaracteristicas Fisicas y Fenotipo Conductual - Galvan Manso y Otros - ArticuloPedro Fernández CardellaÎncă nu există evaluări
- Consensus Classification of Posterior Cortical AtrDocument15 paginiConsensus Classification of Posterior Cortical AtrLuis GómezÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- (Zimmerman, D., Et Al.) Independence of Hot and Cold Executive Function Deficits in High - Functioning Adults With Autism Spectrum DisorderDocument15 pagini(Zimmerman, D., Et Al.) Independence of Hot and Cold Executive Function Deficits in High - Functioning Adults With Autism Spectrum DisorderLuis GómezÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
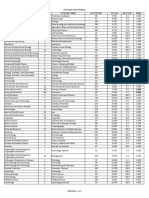
- Annual Review Of: in Category Category Name in Category Factor Half-Life IndexDocument2 paginiAnnual Review Of: in Category Category Name in Category Factor Half-Life IndexLuis GómezÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Large-Scale Brain Networks in Cognition: Emerging Methods and PrinciplesDocument14 paginiLarge-Scale Brain Networks in Cognition: Emerging Methods and PrinciplesLuis GómezÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Author's Accepted Manuscript: Psychiatry ResearchDocument29 paginiAuthor's Accepted Manuscript: Psychiatry ResearchLuis GómezÎncă nu există evaluări
- Mapping The Network For PlanningDocument15 paginiMapping The Network For PlanningLuis GómezÎncă nu există evaluări
- (Revisión) The Cognitive-Affective Neuroscience of The Unconscious (Stein, D., Et Al.)Document5 pagini(Revisión) The Cognitive-Affective Neuroscience of The Unconscious (Stein, D., Et Al.)Luis GómezÎncă nu există evaluări
- BOT-2 Complete Form Sample Report PDFDocument12 paginiBOT-2 Complete Form Sample Report PDFmarioh_40% (1)
- Psychiatric Adverse Drug Reactions in The Paediatric PopulationDocument7 paginiPsychiatric Adverse Drug Reactions in The Paediatric PopulationLuis GómezÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Mapping The Network For PlanningDocument15 paginiMapping The Network For PlanningLuis GómezÎncă nu există evaluări
- (Mizuno, Y., Et Al.) Structural Brain Abnormalities in ChildrenDocument7 pagini(Mizuno, Y., Et Al.) Structural Brain Abnormalities in ChildrenLuis GómezÎncă nu există evaluări
- Bruininks-Oseretsky Test of Motor Proficiency, Second Edition (BOT-2)Document2 paginiBruininks-Oseretsky Test of Motor Proficiency, Second Edition (BOT-2)Luis GómezÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Aging and Alzheimer'S Disease: Lessons From The Nun Study: David A. Snowdon, PHDDocument7 paginiAging and Alzheimer'S Disease: Lessons From The Nun Study: David A. Snowdon, PHDLuis GómezÎncă nu există evaluări
- (Mizuno, Y., Et Al.) Structural Brain Abnormalities in ChildrenDocument7 pagini(Mizuno, Y., Et Al.) Structural Brain Abnormalities in ChildrenLuis GómezÎncă nu există evaluări
- DualTask Performance in Dysexecutive and Nondysexecutive Patients With A Frontal LesionDocument8 paginiDualTask Performance in Dysexecutive and Nondysexecutive Patients With A Frontal LesionLuis GómezÎncă nu există evaluări
- (Cohen, A. Et Al.) Looking Beyond The Face Area. Lesion Network Mapping of Prosopagnosia PDFDocument16 pagini(Cohen, A. Et Al.) Looking Beyond The Face Area. Lesion Network Mapping of Prosopagnosia PDFLuis GómezÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- (Wilson, H., Et Al.) Imidazoline 2 Binding Sites Reflecting Astroglia Pathology in Parkinson's Disease. An in Vivo 11CBU99008 PET Study PDFDocument13 pagini(Wilson, H., Et Al.) Imidazoline 2 Binding Sites Reflecting Astroglia Pathology in Parkinson's Disease. An in Vivo 11CBU99008 PET Study PDFLuis GómezÎncă nu există evaluări
- Mantra MeditationsDocument3 paginiMantra Meditationsjose_luiz_18Încă nu există evaluări
- MeditationDocument2 paginiMeditationmartin100% (1)
- Mantras For Deep Healing and Personal TransformationDocument4 paginiMantras For Deep Healing and Personal TransformationRhett Ligon100% (1)
- Fujimoto Rindo The Way of Zazen PDFDocument26 paginiFujimoto Rindo The Way of Zazen PDFHenri Thomas Magnetiseur Leguevin100% (3)
- Pema Chodron WisdomDocument17 paginiPema Chodron Wisdomredwalla100% (2)
- Transcendental Meditation MantrasDocument6 paginiTranscendental Meditation MantrasJiesa67% (3)
- Stop OverthinkingDocument81 paginiStop OverthinkingElvie CalaraÎncă nu există evaluări
- 04 UM LessonDocument36 pagini04 UM LessonJohn Leclair100% (1)
- G11 - Module1 - Personal DevelopmentDocument36 paginiG11 - Module1 - Personal DevelopmentCrizhae Ocon100% (10)
- Beyond SufferingDocument344 paginiBeyond SufferingDragoș RusuÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Maha Mrityunjaya Article by Rolf SlovikDocument6 paginiMaha Mrityunjaya Article by Rolf SlovikUjwal Golatkar100% (2)
- Psychic Energy EmpowermentDocument2 paginiPsychic Energy EmpowermentFerizÎncă nu există evaluări
- Karuna ReikiDocument16 paginiKaruna ReikiKoushik Mondal50% (6)
- Living The Field - Directed Intention Pt1 by Lynne McTaggartDocument30 paginiLiving The Field - Directed Intention Pt1 by Lynne McTaggartAnonymous 0fjO2o9X100% (5)
- 02-Science Behind MeditationDocument20 pagini02-Science Behind MeditationadithyaÎncă nu există evaluări
- Cbse Net Yoga Paper 2 Nov 2017Document32 paginiCbse Net Yoga Paper 2 Nov 2017बी० के० शर्माÎncă nu există evaluări
- New Loay Dharma Basics I I Template 2012-DinaDocument1 paginăNew Loay Dharma Basics I I Template 2012-Dinaapi-124274210Încă nu există evaluări
- What Is SamadhiDocument2 paginiWhat Is Samadhijele44100% (1)
- Spiritual Health: FactorsDocument3 paginiSpiritual Health: FactorsMikee MeladÎncă nu există evaluări
- Refuge Recovery Index For 1st InventoryDocument8 paginiRefuge Recovery Index For 1st Inventoryapi-342592117Încă nu există evaluări
- Major ArcanaDocument150 paginiMajor ArcanaRupertPupkin7100% (1)
- Insight MeditationDocument2 paginiInsight Meditationnl711Încă nu există evaluări
- Tantric Sex The Beginner's GuideDocument39 paginiTantric Sex The Beginner's GuideuntungrudyÎncă nu există evaluări
- Astro Yoga PDFDocument11 paginiAstro Yoga PDFNagarajÎncă nu există evaluări
- Yoginis in Persian and Arabic TextsDocument15 paginiYoginis in Persian and Arabic Textsmday83Încă nu există evaluări
- Bikkhu Khantipalo - Calm and Insight A Buddhist PDFDocument152 paginiBikkhu Khantipalo - Calm and Insight A Buddhist PDFFelipe Pizarro CorderoÎncă nu există evaluări
- 123Document1 pagină123Vasi KaranÎncă nu există evaluări
- Concentration and Meditation by Christmas HumphreysDocument245 paginiConcentration and Meditation by Christmas Humphreyssusanvanscoyoc987075% (4)
- So Why A Walking MeditationDocument2 paginiSo Why A Walking MeditationVeronica Boglis100% (1)
- The Manual of BreathingDocument29 paginiThe Manual of Breathinglxman_thapaÎncă nu există evaluări
- The Stoic Mindset: Living the Ten Principles of StoicismDe la EverandThe Stoic Mindset: Living the Ten Principles of StoicismEvaluare: 5 din 5 stele5/5 (5)
- Summary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesDe la EverandSummary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesEvaluare: 5 din 5 stele5/5 (1635)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The 7 Habits of Highly Effective People: The Infographics EditionDe la EverandThe 7 Habits of Highly Effective People: The Infographics EditionEvaluare: 4 din 5 stele4/5 (2475)
- The 16 Undeniable Laws of Communication: Apply Them and Make the Most of Your MessageDe la EverandThe 16 Undeniable Laws of Communication: Apply Them and Make the Most of Your MessageEvaluare: 5 din 5 stele5/5 (73)
- The Power of Now: A Guide to Spiritual EnlightenmentDe la EverandThe Power of Now: A Guide to Spiritual EnlightenmentEvaluare: 4.5 din 5 stele4.5/5 (4125)