S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- ReflectionDocument11 paginiReflectionSarahJane100% (1)
- ITOM DocumentationDocument12 paginiITOM DocumentationzeeraÎncă nu există evaluări
- Hayek DKKDocument7 paginiHayek DKKwatidinaÎncă nu există evaluări
- Soal 3Document5 paginiSoal 3watidinaÎncă nu există evaluări
- A Conservative Technique For Repairing Class IV Composite RestorationsDocument6 paginiA Conservative Technique For Repairing Class IV Composite RestorationswatidinaÎncă nu există evaluări
- Healing of Tooth Extraction Socket: Dr. Pankaj Datta Dr. Shilpa Khullar Dr. Mittal ADocument3 paginiHealing of Tooth Extraction Socket: Dr. Pankaj Datta Dr. Shilpa Khullar Dr. Mittal AwatidinaÎncă nu există evaluări
- Kanagalingam2015 PDFDocument10 paginiKanagalingam2015 PDFwatidinaÎncă nu există evaluări
- Antiseptics in The Era of Bacterial Resistance A Focus On Povidone IodineDocument14 paginiAntiseptics in The Era of Bacterial Resistance A Focus On Povidone IodinewatidinaÎncă nu există evaluări
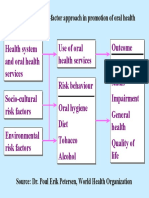
- Figure 5: The Risk-Factor Approach in Promotion of Oral HealthDocument1 paginăFigure 5: The Risk-Factor Approach in Promotion of Oral HealthwatidinaÎncă nu există evaluări
- A Brief Study On Catharanthus Roseus: A Review: Anti-Microbial ActivityDocument5 paginiA Brief Study On Catharanthus Roseus: A Review: Anti-Microbial ActivitywatidinaÎncă nu există evaluări
- Scanned With CamscannerDocument7 paginiScanned With CamscannerwatidinaÎncă nu există evaluări
- Prevention and Control of Noncommunicable DiseasesDocument3 paginiPrevention and Control of Noncommunicable DiseaseswatidinaÎncă nu există evaluări
- A Brief Study On Catharanthus Roseus: A Review: Anti-Microbial ActivityDocument5 paginiA Brief Study On Catharanthus Roseus: A Review: Anti-Microbial ActivitywatidinaÎncă nu există evaluări
- 2 2 15 923 PDFDocument4 pagini2 2 15 923 PDFwatidina100% (1)
- Daftar PustakaDocument1 paginăDaftar PustakawatidinaÎncă nu există evaluări
- Casebook On Human Dignity and Human Rights, Bioethics Core CurriculumDocument144 paginiCasebook On Human Dignity and Human Rights, Bioethics Core CurriculumGlobal Justice AcademyÎncă nu există evaluări
- Health and Fitness Vocab (6799)Document2 paginiHealth and Fitness Vocab (6799)yoanaloÎncă nu există evaluări
- Pyoderma Gangrenosum A Review of Orthopedic Case ReportsDocument4 paginiPyoderma Gangrenosum A Review of Orthopedic Case ReportsIga Nurwani RidwanÎncă nu există evaluări
- Problems With Use of A Foley Catheter In20160222-1033-Xkz5o PDFDocument4 paginiProblems With Use of A Foley Catheter In20160222-1033-Xkz5o PDFjune rondonÎncă nu există evaluări
- ACE Vison Health Consultants Pvt. Ltd. - KandiwaliDocument19 paginiACE Vison Health Consultants Pvt. Ltd. - KandiwalinabhjpÎncă nu există evaluări
- TB Case HXDocument6 paginiTB Case HXatikah_jamilÎncă nu există evaluări
- Tiktok Nasi Anti-Gemuk-2Document5 paginiTiktok Nasi Anti-Gemuk-2PararaeÎncă nu există evaluări
- Medical History Report Medical Prescreen QuestionnaireDocument4 paginiMedical History Report Medical Prescreen Questionnairejames antonioÎncă nu există evaluări
- Sri Ratu Septini Farmasi 4B PDFDocument8 paginiSri Ratu Septini Farmasi 4B PDFWinanda SitinjakÎncă nu există evaluări
- Best Practice'' For Patient-Centered Communication: A Narrative ReviewDocument9 paginiBest Practice'' For Patient-Centered Communication: A Narrative ReviewFernanda BordignonÎncă nu există evaluări
- Systemic Inflammatory Response Syndrome (SIRS) PrognosisDocument16 paginiSystemic Inflammatory Response Syndrome (SIRS) PrognosisIPGDx100% (1)
- Practical Research 2Document18 paginiPractical Research 2Maryrose TrajeBarroÎncă nu există evaluări
- Pengaruh Aplikasi Karbamid Peroksida 20% Dan 35% Terhadap Kekerasan Resin Komposit Mikro HibridDocument5 paginiPengaruh Aplikasi Karbamid Peroksida 20% Dan 35% Terhadap Kekerasan Resin Komposit Mikro HibridAyasha ApriliaÎncă nu există evaluări
- Isbi Practice Guidelines For Burn Care, Part 2: SciencedirectDocument90 paginiIsbi Practice Guidelines For Burn Care, Part 2: SciencedirectDella pinkaÎncă nu există evaluări
- FSPR Masalunga1Document34 paginiFSPR Masalunga1Janela CaballesÎncă nu există evaluări
- Analisis Pengendalian Persediaan Obat-Obatan Instalasi FarmasiDocument20 paginiAnalisis Pengendalian Persediaan Obat-Obatan Instalasi Farmasitri handayaniÎncă nu există evaluări
- Family PlanningDocument42 paginiFamily PlanningRendy BayhaqiÎncă nu există evaluări
- Daftar Pustaka FinalDocument8 paginiDaftar Pustaka FinalBayu DestiawanÎncă nu există evaluări
- Comparison Between Hygiene and SanitationDocument4 paginiComparison Between Hygiene and SanitationtibebuÎncă nu există evaluări
- Referat Mata KeratititsDocument28 paginiReferat Mata KeratititsjantyÎncă nu există evaluări
- ANEXA Nr. 9 Certificat Medical Medical Fitness CertificateDocument1 paginăANEXA Nr. 9 Certificat Medical Medical Fitness CertificatePrisacaru MarianÎncă nu există evaluări
- Report AyendeDocument13 paginiReport AyendeAbubakar RabiuÎncă nu există evaluări
- Handicapped ChildrenDocument36 paginiHandicapped ChildrenAbdur RehmanÎncă nu există evaluări
- CloningDocument6 paginiCloningAngel L.Încă nu există evaluări
- Toprank Midterms Post TestDocument80 paginiToprank Midterms Post TestMaria Ana AguilarÎncă nu există evaluări
- ArticuloDocument8 paginiArticuloAkcyre PalominoÎncă nu există evaluări
- Cardiovascular Conditioning Monitoring ChartDocument2 paginiCardiovascular Conditioning Monitoring ChartDanielle Patricia Valencia OtedaÎncă nu există evaluări
- Vitamin C in Health and Disease PDFDocument300 paginiVitamin C in Health and Disease PDFNany Caroline100% (1)