S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Stephen Jones - Secrets of TimeDocument237 paginiStephen Jones - Secrets of TimeKld Brn86% (7)
- Organizational Behavior by McShane and Von Gilnow Test BankDocument10 paginiOrganizational Behavior by McShane and Von Gilnow Test BankSharn Linzi Buan MontañoÎncă nu există evaluări
- Political Order in Changing SocietiesDocument83 paginiPolitical Order in Changing SocietiesMichiru2011100% (1)
- CodicilDocument2 paginiCodicilJJ Gapol100% (4)
- Sample Complaint For Foreclosure of Mechanics Lien in CaliforniaDocument3 paginiSample Complaint For Foreclosure of Mechanics Lien in CaliforniacellajonesÎncă nu există evaluări
- Agbayani v. PNB, G.R. No. L-23127, April 29, 1971.full TextDocument5 paginiAgbayani v. PNB, G.R. No. L-23127, April 29, 1971.full TextRyuzaki HidekiÎncă nu există evaluări
- Maintenance and Welfare of Parents and Senior Citizens ActDocument12 paginiMaintenance and Welfare of Parents and Senior Citizens ActKrishna PrasadÎncă nu există evaluări
- Decisive Chip Heath and Dan HeathDocument1 paginăDecisive Chip Heath and Dan HeathHoratiu BahneanÎncă nu există evaluări
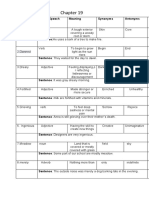
- Tom Sawyer Vocabulary.1681608284879Document22 paginiTom Sawyer Vocabulary.1681608284879Vhone NeyraÎncă nu există evaluări
- Basic Concepts in Contract Drafting Vincent MartoranaDocument92 paginiBasic Concepts in Contract Drafting Vincent MartoranaEllen Highlander100% (1)
- COMPARATIVE PUBLIC LAW and Research Methedology Assignment PDFDocument2 paginiCOMPARATIVE PUBLIC LAW and Research Methedology Assignment PDFKARTHIK A0% (1)
- Patrick Gray & John D. Cox - Shakespeare and Renaissance EthicsDocument322 paginiPatrick Gray & John D. Cox - Shakespeare and Renaissance EthicsEveraldo TeixeiraÎncă nu există evaluări
- Social Studies IiiDocument17 paginiSocial Studies Iiiain_aina9228100% (1)
- Almirez Vs Infinite Loop TechnologyDocument2 paginiAlmirez Vs Infinite Loop TechnologyJulian DubaÎncă nu există evaluări
- Drama - Essay On Feminism Found in The Play, TartuffeDocument4 paginiDrama - Essay On Feminism Found in The Play, Tartuffemorecicero100% (1)
- Abs CBN vs. Ombudsman 2010Document11 paginiAbs CBN vs. Ombudsman 2010Mara VinluanÎncă nu există evaluări
- Contract: Abdul Majid Khalil (LL.M, UK)Document26 paginiContract: Abdul Majid Khalil (LL.M, UK)shershahÎncă nu există evaluări
- 04 Integrated Contractor v. NLRCDocument2 pagini04 Integrated Contractor v. NLRCJill BagaoisanÎncă nu există evaluări
- Anger ManagementDocument12 paginiAnger ManagementKITE Corpuz100% (2)
- BAPMI Rules On ArbitratorsDocument5 paginiBAPMI Rules On Arbitratorsedwina_kharismaÎncă nu există evaluări
- 10 Ways To Show Good CitizenshipDocument4 pagini10 Ways To Show Good CitizenshipJuuri KuranÎncă nu există evaluări
- Social Studies S.B.ADocument25 paginiSocial Studies S.B.AChyrane50% (2)
- ANTONIODocument5 paginiANTONIOAriana TushinÎncă nu există evaluări
- Keogh ComplaintDocument5 paginiKeogh ComplaintWIS Digital News StaffÎncă nu există evaluări
- Shahnama 09 FirduoftDocument426 paginiShahnama 09 FirduoftScott KennedyÎncă nu există evaluări
- MBTI Personality Type Test: Name: - Roll NoDocument4 paginiMBTI Personality Type Test: Name: - Roll NoSaurabh Kulkarni 23100% (1)
- MedicalVerification PDFDocument3 paginiMedicalVerification PDFOptical RecoveryÎncă nu există evaluări
- ICS-Transmile Group BerhadDocument36 paginiICS-Transmile Group Berhadhaliza amirah93% (14)
- 6843 21205 1 PBDocument8 pagini6843 21205 1 PBikc711Încă nu există evaluări
- Literary Theory by Eagleton NotesDocument16 paginiLiterary Theory by Eagleton NotesLarryBajina321Încă nu există evaluări