S-ar putea să vă placă și
- 6566 - Noções Gerais Sobre o Sistema Circulatório e RespiratórioDocument3 pagini6566 - Noções Gerais Sobre o Sistema Circulatório e RespiratórioDagdaPicks0% (1)
- Lipedema Magazie Volume 4 Number 1Document44 paginiLipedema Magazie Volume 4 Number 1Alexandre Campos Moraes Amato100% (1)
- Lipedema InfograficoDocument1 paginăLipedema InfograficoAlexandre Campos Moraes AmatoÎncă nu există evaluări
- BANNER ProntoDocument1 paginăBANNER ProntoDebora Figueiredo100% (1)
- SS92 - Book - WEB 2Document36 paginiSS92 - Book - WEB 2Alexandre Campos Moraes AmatoÎncă nu există evaluări
- Folha Vascular 247Document20 paginiFolha Vascular 247Alexandre Campos Moraes AmatoÎncă nu există evaluări
- Super Saudavel Ano XXI n92Document36 paginiSuper Saudavel Ano XXI n92Alexandre Campos Moraes AmatoÎncă nu există evaluări
- Folha Vascular 243Document20 paginiFolha Vascular 243Alexandre Campos Moraes AmatoÎncă nu există evaluări
- 13.12.2020 LipedemaDocument1 pagină13.12.2020 LipedemaAlexandre Campos Moraes AmatoÎncă nu există evaluări
- 39 Dicas para Se Proteger Contra Abusos Dos Auditores e PlanosDocument9 pagini39 Dicas para Se Proteger Contra Abusos Dos Auditores e PlanosAlexandre Campos Moraes AmatoÎncă nu există evaluări
- Resolução Normativa - RN #387, de 28 de Outubro de 2015Document16 paginiResolução Normativa - RN #387, de 28 de Outubro de 2015Alexandre Campos Moraes AmatoÎncă nu există evaluări
- Tradução, Adaptação Cultural e Validação Do Questionário de Avaliação Sintomática Do Lipedema (QuASiL) .Document8 paginiTradução, Adaptação Cultural e Validação Do Questionário de Avaliação Sintomática Do Lipedema (QuASiL) .Alexandre Campos Moraes AmatoÎncă nu există evaluări
- Ebook - Como Prevenir Varizes - Dr. ALEXANDRE AMATODocument2 paginiEbook - Como Prevenir Varizes - Dr. ALEXANDRE AMATOAlexandre Campos Moraes AmatoÎncă nu există evaluări
- Folha Vascular 234Document20 paginiFolha Vascular 234Alexandre Campos Moraes AmatoÎncă nu există evaluări
- Inteligência Coletiva Na Era Da InternetDocument2 paginiInteligência Coletiva Na Era Da InternetAlexandre Campos Moraes AmatoÎncă nu există evaluări
- AnexoI Rol-2018 OkDocument98 paginiAnexoI Rol-2018 OkKent RenemberÎncă nu există evaluări
- Programa Nacional de Prevenção e Controle de Infecções Relacionadas À Assistência À Saúde (2013-2015)Document21 paginiPrograma Nacional de Prevenção e Controle de Infecções Relacionadas À Assistência À Saúde (2013-2015)Flavia Oliveira PampolhaÎncă nu există evaluări
- Adesivo Anticoncepcional - Amato InstitutoDocument1 paginăAdesivo Anticoncepcional - Amato InstitutoAlexandre Campos Moraes AmatoÎncă nu există evaluări
- Lipedema Associado A Obesidade, Linfedema e Insuficiência Venosa: Relato de Um CasoDocument5 paginiLipedema Associado A Obesidade, Linfedema e Insuficiência Venosa: Relato de Um CasoAlexandre Campos Moraes AmatoÎncă nu există evaluări
- R$20,00 UMA CONSULTA MÉDICA, Por Valério Augusto RibeiroDocument5 paginiR$20,00 UMA CONSULTA MÉDICA, Por Valério Augusto RibeiroAlexandre Campos Moraes AmatoÎncă nu există evaluări
- Fisiologia GastrointestinalDocument55 paginiFisiologia GastrointestinalThiago LimaÎncă nu există evaluări
- Cronograma PPCSA ManhãDocument3 paginiCronograma PPCSA Manhãamandinha_popi8162Încă nu există evaluări
- Atualização Do Diagnóstico e Tratamento Da Doença de AlzheimerDocument28 paginiAtualização Do Diagnóstico e Tratamento Da Doença de Alzheimerstefanyvs234Încă nu există evaluări
- Ebook Como Usar Seus Óleos EssesnciaisDocument89 paginiEbook Como Usar Seus Óleos EssesnciaisMariane Gabriela Cesar Ribeiro FerreiraÎncă nu există evaluări
- BetainaDocument2 paginiBetainaNatta ApucaranaÎncă nu există evaluări
- Enterotomia, Enterectomia e EnteroanastomoseDocument34 paginiEnterotomia, Enterectomia e EnteroanastomoseAdriele FernandesÎncă nu există evaluări
- Guia Medico Julho2021Document69 paginiGuia Medico Julho2021Jeniffer AraujoÎncă nu există evaluări
- Pediatria 6 - Crescimento e DesenvolvimentoDocument3 paginiPediatria 6 - Crescimento e DesenvolvimentoBruna da MacenoÎncă nu există evaluări
- Hemograma Completo: #Da Guia: Cliente: Médico: 18/09/2020 2071790 22/06/1984Document1 paginăHemograma Completo: #Da Guia: Cliente: Médico: 18/09/2020 2071790 22/06/1984Fredy MoreiraÎncă nu există evaluări
- Atividade 01 (Aula 01 e 02)Document5 paginiAtividade 01 (Aula 01 e 02)Danilo VQÎncă nu există evaluări
- Tabelas AntibioticosDocument3 paginiTabelas AntibioticosVanessa LimaÎncă nu există evaluări
- Avaliação Da DemênciaDocument44 paginiAvaliação Da Demênciavanfafiafia100% (2)
- EsteNaoeMaisUmLivroDeDietas-BONUS-Diabetes Tipo 2 (Reversão)Document7 paginiEsteNaoeMaisUmLivroDeDietas-BONUS-Diabetes Tipo 2 (Reversão)sergiorsantosÎncă nu există evaluări
- Biomagnetismo e VermesDocument2 paginiBiomagnetismo e VermesAna Paula Brigagão100% (1)
- Planilha Sem Título - Página1Document4 paginiPlanilha Sem Título - Página1Mayara CesarÎncă nu există evaluări
- Manual Biosseguranca PDFDocument80 paginiManual Biosseguranca PDFfabianoÎncă nu există evaluări
- RCP Pediatrico - Ana Elida e Nilcyeli AragaoDocument18 paginiRCP Pediatrico - Ana Elida e Nilcyeli AragaofalaulissesÎncă nu există evaluări
- Audiência Publica LeitosDocument19 paginiAudiência Publica LeitosMetropolesÎncă nu există evaluări
- IST Infecções Sexualmente Transmissíveis O Q Ue É Ist?: A Prevenção É o Melhor RemédioDocument1 paginăIST Infecções Sexualmente Transmissíveis O Q Ue É Ist?: A Prevenção É o Melhor RemédioElisangela ErickaÎncă nu există evaluări
- Alterações Psicológicas Na Gravidez 1Document14 paginiAlterações Psicológicas Na Gravidez 1Angela Borges100% (1)
- GT Cosaude Reuniao 4 ApresentacoesDocument204 paginiGT Cosaude Reuniao 4 ApresentacoesJose Do NascimentoÎncă nu există evaluări
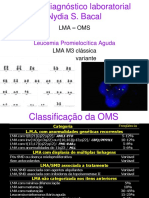
- 48 - Leucemia Promielocitica Aguda-Diagnóstico LaboratorialDocument53 pagini48 - Leucemia Promielocitica Aguda-Diagnóstico LaboratorialAbraham DiazÎncă nu există evaluări
- Diálise PeritonealDocument14 paginiDiálise PeritonealRamon Lima Myazawa100% (1)
- Medicina Pror Medcurso Residencia DPOCDocument7 paginiMedicina Pror Medcurso Residencia DPOCLuis Gustavo Pereira BoutrosÎncă nu există evaluări
- 04 Uso de Barreira de Polipropileno Pós Exodontia Rev. Bras. Impl. 2009 PDFDocument4 pagini04 Uso de Barreira de Polipropileno Pós Exodontia Rev. Bras. Impl. 2009 PDFCarlos AugustoÎncă nu există evaluări
- Manual Diu 08 2018 PDFDocument72 paginiManual Diu 08 2018 PDFIvana FreitasÎncă nu există evaluări
- Resumo Primeiros Socorros - APHDocument3 paginiResumo Primeiros Socorros - APHCamila ContilhoÎncă nu există evaluări
- Esferocitose Hereditaria ArtigoDocument5 paginiEsferocitose Hereditaria ArtigoJaqueline Covatti VargasÎncă nu există evaluări