S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Art Psychotherapy-Harriet WadesonDocument3 paginiArt Psychotherapy-Harriet WadesonfasfasfÎncă nu există evaluări
- Anxietate de SeparareDocument2 paginiAnxietate de SeparareTabita PetreanÎncă nu există evaluări
- 2.1.7. Guidelines For DV Support Group Facilitators (New)Document17 pagini2.1.7. Guidelines For DV Support Group Facilitators (New)Tabita PetreanÎncă nu există evaluări
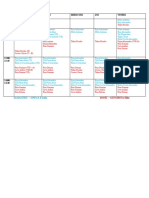
- Orar Grupe - PROVIZORIUDDocument2 paginiOrar Grupe - PROVIZORIUDTabita PetreanÎncă nu există evaluări
- Msi 1114Document78 paginiMsi 1114Tabita PetreanÎncă nu există evaluări
- Editable Coloured SquaresDocument6 paginiEditable Coloured SquaresTabita PetreanÎncă nu există evaluări
- Prezentare CSEI - TabitaDocument2 paginiPrezentare CSEI - TabitaTabita PetreanÎncă nu există evaluări
- An Analysis of The Use and Success of Online Recruitment Methods in The UKDocument41 paginiAn Analysis of The Use and Success of Online Recruitment Methods in The UKKazi MilonÎncă nu există evaluări
- Foarte Bun Overparenting and Young Adult Narcissism - Psychological Control ADocument76 paginiFoarte Bun Overparenting and Young Adult Narcissism - Psychological Control ATabita PetreanÎncă nu există evaluări
- Bun Hock 2001Document16 paginiBun Hock 2001Tabita PetreanÎncă nu există evaluări
- Plastificat PDFDocument31 paginiPlastificat PDFTabita PetreanÎncă nu există evaluări
- Human Resources Management Optimization in The Romanian Armed ForcesDocument1 paginăHuman Resources Management Optimization in The Romanian Armed ForcesTabita PetreanÎncă nu există evaluări
- Rogers and Kohut A Historical Perspective Psicoanalytic Psychology PDFDocument21 paginiRogers and Kohut A Historical Perspective Psicoanalytic Psychology PDFSilvana HekierÎncă nu există evaluări
- Illness ManagementDocument78 paginiIllness Managementresearch9175Încă nu există evaluări
- Adhd HandoutDocument2 paginiAdhd Handoutapi-313986755Încă nu există evaluări
- Owen Et Al. (2011) - Clients' Perceptions of Their Psychotherapists' Multicultural OrientationDocument9 paginiOwen Et Al. (2011) - Clients' Perceptions of Their Psychotherapists' Multicultural OrientationL MÎncă nu există evaluări
- M Phil Clinical PsychologyDocument41 paginiM Phil Clinical PsychologyNazema_SagiÎncă nu există evaluări
- Positive Thinking and Academic PerformanceDocument12 paginiPositive Thinking and Academic Performanceapi-267854035Încă nu există evaluări
- Steven Franklin Greer 1 PDFDocument136 paginiSteven Franklin Greer 1 PDFWKYC.comÎncă nu există evaluări
- Take Art To HeartDocument3 paginiTake Art To HeartAutismeyeÎncă nu există evaluări
- Procrastination A Serious Problem Preval-1Document7 paginiProcrastination A Serious Problem Preval-1Allyza Nuguid FrondozaÎncă nu există evaluări
- PTSD - Diagnostic CriteriaDocument5 paginiPTSD - Diagnostic Criteriagreg sÎncă nu există evaluări
- Positive Vs Negative ReinforcementDocument3 paginiPositive Vs Negative ReinforcementHidayah Roslee100% (1)
- Abraham MaslowDocument13 paginiAbraham Maslowfrediizee WinsÎncă nu există evaluări
- Oxford Textbook of PsychiatryDocument6 paginiOxford Textbook of Psychiatrygolof0% (1)
- Psychology 4 9 18Document15 paginiPsychology 4 9 18rehanakhatun27121999Încă nu există evaluări
- Play Therapy MenassaDocument15 paginiPlay Therapy MenassaNur Hidayah DaniÎncă nu există evaluări
- Chapter 13 OutlineDocument5 paginiChapter 13 OutlineHockeyboy41Încă nu există evaluări
- Anatomy of An EpidemicDocument13 paginiAnatomy of An EpidemicCris RodriguesÎncă nu există evaluări
- Rational Emotive Behavioral Therapy: Josemon P.George V Mba (PT)Document27 paginiRational Emotive Behavioral Therapy: Josemon P.George V Mba (PT)Josemon George ParanilamÎncă nu există evaluări
- Traumatic Antecedents Questionnaire (TAQ)Document9 paginiTraumatic Antecedents Questionnaire (TAQ)TEOFILO PALSIMON JR.Încă nu există evaluări
- Human MemoryDocument16 paginiHuman MemoryJesh Alberto100% (2)
- Somatic Therapy: A Form of Therapy Also Known AsDocument56 paginiSomatic Therapy: A Form of Therapy Also Known AsReginette Pisalbo ChanÎncă nu există evaluări
- Studi Pemberian Antipsikotik Terhadap Beberapa Jenis Skizofrenia Di RSJD Atma Husada Mahakam SamarindaDocument9 paginiStudi Pemberian Antipsikotik Terhadap Beberapa Jenis Skizofrenia Di RSJD Atma Husada Mahakam Samarindawulan faddhylanÎncă nu există evaluări
- Article Six Modes of Decision MakingDocument8 paginiArticle Six Modes of Decision MakingBalamurugan VaradarajanÎncă nu există evaluări
- Ebook PDF Current Psychotherapies 11th Edition by Danny Wedding PDFDocument41 paginiEbook PDF Current Psychotherapies 11th Edition by Danny Wedding PDFcecil.slocum194100% (38)
- Article - What Does The Dreamer Want - Engaging The Inner Healer - International Association For The Study of DreamsDocument3 paginiArticle - What Does The Dreamer Want - Engaging The Inner Healer - International Association For The Study of DreamsTem CuÎncă nu există evaluări
- The To Hypnosis E-Book: by Rory Z FulcherDocument16 paginiThe To Hypnosis E-Book: by Rory Z FulcherConrad SlaterÎncă nu există evaluări
- Psychoanalytic Theory by Sigmund FreudDocument23 paginiPsychoanalytic Theory by Sigmund FreudYongÎncă nu există evaluări
- The Unified Protocol For Transdiagnostic Treatment of Emotional Disorders in Children (UP-C) in Portugal: Feasibility Study ResultsDocument24 paginiThe Unified Protocol For Transdiagnostic Treatment of Emotional Disorders in Children (UP-C) in Portugal: Feasibility Study ResultsAndrade GuiÎncă nu există evaluări
- Natalie Riback, Registered Psychotherapist: RP, CTP Dipl, BaDocument5 paginiNatalie Riback, Registered Psychotherapist: RP, CTP Dipl, BaKevwe KevweÎncă nu există evaluări