S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Sirkum Igd RSMS Bulan Januari 2020Document1 paginăSirkum Igd RSMS Bulan Januari 2020Enniq MazayudhaÎncă nu există evaluări
- Bab I ENNIQDocument17 paginiBab I ENNIQEnniq MazayudhaÎncă nu există evaluări
- Keaslian Penelitian Timbang Terima EnniqDocument4 paginiKeaslian Penelitian Timbang Terima EnniqEnniq MazayudhaÎncă nu există evaluări
- Suhu Pre Kompres Suhu Post Kompres CrosstabulationDocument1 paginăSuhu Pre Kompres Suhu Post Kompres CrosstabulationEnniq MazayudhaÎncă nu există evaluări
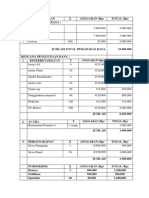
- Ʃ Anggaran (RP) Total (RP)Document2 paginiƩ Anggaran (RP) Total (RP)Enniq MazayudhaÎncă nu există evaluări
- Ʃ Anggaran (RP) Total (RP)Document2 paginiƩ Anggaran (RP) Total (RP)Enniq MazayudhaÎncă nu există evaluări
- L 12 Case Processing Summary NEWDocument2 paginiL 12 Case Processing Summary NEWEnniq MazayudhaÎncă nu există evaluări
- L 12 Case Processing Summary NEWDocument2 paginiL 12 Case Processing Summary NEWEnniq MazayudhaÎncă nu există evaluări
- L 12 Case Processing Summary NEWDocument2 paginiL 12 Case Processing Summary NEWEnniq MazayudhaÎncă nu există evaluări
- L 13 FrekwensiDocument1 paginăL 13 FrekwensiEnniq MazayudhaÎncă nu există evaluări
- L 13 FrekwensiDocument1 paginăL 13 FrekwensiEnniq MazayudhaÎncă nu există evaluări
- 93 507 1 PBDocument6 pagini93 507 1 PBEnniq MazayudhaÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Company Introduction BenoyDocument19 paginiCompany Introduction Benoymohdzafaryab2402Încă nu există evaluări
- Power Electronics Homework SolutionsDocument5 paginiPower Electronics Homework Solutionsafnabzdmfiefxr100% (1)
- Overview of Voltage Sag MitigationDocument7 paginiOverview of Voltage Sag MitigationJjjjpfÎncă nu există evaluări
- Mis S2Document25 paginiMis S2Abin AntonyÎncă nu există evaluări
- Creators2 Lesson7 3rdeditionDocument27 paginiCreators2 Lesson7 3rdeditionLace CabatoÎncă nu există evaluări
- X32 DIGITAL MIXER Preliminary User ManualDocument1 paginăX32 DIGITAL MIXER Preliminary User ManualhrbinaÎncă nu există evaluări
- CS RecordDocument97 paginiCS RecordsharmikbkÎncă nu există evaluări
- Vxworks Installing 6.9Document16 paginiVxworks Installing 6.9Jérémy BouteillerÎncă nu există evaluări
- LITHME Conference 2022 Book of Abstracts v1Document43 paginiLITHME Conference 2022 Book of Abstracts v1Marin VozianÎncă nu există evaluări
- 4U Incline AccelerationDocument4 pagini4U Incline AccelerationUshbah AsimÎncă nu există evaluări
- Catalogo ImportsumaryDocument50 paginiCatalogo ImportsumaryMatthew EnglandÎncă nu există evaluări
- Stream CipherDocument214 paginiStream CipherAyush TibrewalaÎncă nu există evaluări
- Acer Veriton S661 QSDocument3 paginiAcer Veriton S661 QSAspurlah Mohamed Jidi IÎncă nu există evaluări
- Evalue Serve - PRCDocument14 paginiEvalue Serve - PRCJasleen KaurÎncă nu există evaluări
- Oracle Database Cloud Cookbook With Oracle Enterprise Manager 13c Cloud ControlDocument559 paginiOracle Database Cloud Cookbook With Oracle Enterprise Manager 13c Cloud ControlSavo100% (4)
- Ds-2Cd2047G1-L 4 MP Colorvu Fixed Bullet Network CameraDocument5 paginiDs-2Cd2047G1-L 4 MP Colorvu Fixed Bullet Network CameraNazih Ben JemaaÎncă nu există evaluări
- Dilency Dcosta EA - 14112023Document5 paginiDilency Dcosta EA - 14112023manjuhm1707licÎncă nu există evaluări
- How To Calculate Reinforcement WeigDocument3 paginiHow To Calculate Reinforcement Weigyusufchin202Încă nu există evaluări
- Review Problems SolutionsDocument6 paginiReview Problems SolutionsDimitrios PanaÎncă nu există evaluări
- Library and Information ScienceDocument32 paginiLibrary and Information Scienceneilesh300100% (2)
- Digital Pakistan's JounneryDocument4 paginiDigital Pakistan's JounnerysyedchangezafarÎncă nu există evaluări
- Laser Based Intruder AlarmDocument25 paginiLaser Based Intruder Alarmdivyaa76Încă nu există evaluări
- 7.6 Branch and Bound Method: C 1 1 0 0 0 Basic Variables Basic Basic Variables X X S S S Coefficient Variables ValuesDocument8 pagini7.6 Branch and Bound Method: C 1 1 0 0 0 Basic Variables Basic Basic Variables X X S S S Coefficient Variables ValuesKowsalyaÎncă nu există evaluări
- Bölümlere Göre Ki̇tap Li̇stesi̇Document94 paginiBölümlere Göre Ki̇tap Li̇stesi̇NanaNanaÎncă nu există evaluări
- DS-7600NI-I2/P Series NVR: Key FeatureDocument5 paginiDS-7600NI-I2/P Series NVR: Key FeatureFabian BonillaÎncă nu există evaluări
- Electronics and Communication Engineering: Projectbased Lab Report OnDocument21 paginiElectronics and Communication Engineering: Projectbased Lab Report OnGowtham RoxtaÎncă nu există evaluări
- PDF Procedures in Using Ge Survey Systempdf DDDocument21 paginiPDF Procedures in Using Ge Survey Systempdf DDAriel AsunsionÎncă nu există evaluări
- CCTV Fdas Sprinkler Biometrics Access Control Web Development PabxDocument2 paginiCCTV Fdas Sprinkler Biometrics Access Control Web Development PabxKris Larine Orillo-DavisÎncă nu există evaluări
- The Evolution of Project ManagementDocument5 paginiThe Evolution of Project Managementcrib85Încă nu există evaluări
- Service Asset and Configuration ManagementDocument12 paginiService Asset and Configuration ManagementhercexÎncă nu există evaluări